
Abstract
This study aimed to investigate deep vein thrombosis (DVT) in patients with lower extremity fractures who received anticoagulation treatment in the perioperative stage. We collected the patients’ clinical data and diagnosed DVT using Doppler ultrasonography. Preoperative, postoperative, and 1-month postoperative examinations were performed. The patients were divided into thrombosis and non-thrombosis groups according to ultrasonographic findings. A total of 404 patients were included in the study. The preoperative, postoperative, and 1-month postoperative incidence rates were, respectively, 35%, 55%, and 40% for DVT and 12%, 22%, and 20% for DVT in the uninjured contralateral lower extremity. The incidence of perioperative DVT decreased over time from 223 (55%) to 161 (40%). Multivariate analysis revealed that the independent risk factors for preoperative that of DVT were age (odds ratio [OR]: 1.03; 95% CI: 1.01-1.04; P = .000); postoperative that of DVT were age (OR: 1.04; 95% CI: 1.03-1.05; P = .000), blood loss (OR: 1.001; 95% CI: 1.000-1.002; P = .018), and American Society of Anesthesiologists classification (OR: 2.07; 95% CI: 1.16-3.72; P = .014); and 1-month postoperative that of DVT were age (OR: 1.05; 95% CI: 1.03-1.07; P = .000), respectively. In conclusion, the incidence of perioperative DVT decreased over time in patients who received anticoagulation treatment. Age was an important risk factor for perioperative DVT.
Introduction
Deep vein thrombosis (DVT) of the lower extremities is a common complication in trauma patients. The incidence of DVT after trauma was reported to be approximately 9.1% to 11.1%. 1,2 Deep vein thrombosis should be prevented and treated in a timely manner; otherwise, it can lead to chronic pain, secondary varicose veins, or ulcers, which seriously affect patients’ quality of life. Fatal pulmonary embolism can also occur in some cases. 3 In recent years, orthopedists have paid increasing attention to the prophylaxis and treatment of DVT.
Currently, pharmacological prevention is considered among the most effective methods to decrease the incidence of lower extremity DVT. 4 Traditional low-molecular-weight heparin (LMWH) 5 –7 is a popular choice. However, it can lead to local pain and even subcutaneous induration, while some patients develop heparin-induced thrombocytopenia that leads to bleeding and other adverse events. New oral anticoagulants (selective factor Xa inhibitors such as rivaroxaban 8 and apixaban 9 ) have made postoperative anticoagulant therapy more convenient and provided a sustained treatment strategy for venous thrombosis. 10
For patients with high risk of thrombosis, perioperative prevention is needed in addition to continued anticoagulant therapy after discharge to prevent fatal pulmonary embolism caused by DVT. In our hospital, LMWH was used during hospitalization, and rivaroxaban was used after discharge.
In one study with >2000 patients from a Chinese population, 8 patients were given rivaroxaban or LMWH to prevent DVT at admission and while awaiting for surgery and then shortly after surgery. However, lower extremity vascular ultrasonography or angiography to screen for new DVT was only performed when lower limb swelling, local tenderness, or unexplained fever occurred. As most cases of lower extremity DVT could change during the operation, 11 noninvasive vascular ultrasonography should be used as a routine examination modality, especially at different time points in the perioperative period. In this study, the objective was to investigate the different onset times and perioperative changes of DVT in patients with lower extremity fractures who received LMWH and rivaroxaban therapy.
Methods
Ethics Statement
This study analyzed the data of patients with lower extremity fractures who were admitted between June 1, 2016, and March 31, 2017, in Honghui Hospital, Xi’an Jiaotong University. The study was approved by the ethics review board of Xi’an Jiaotong University.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: (a) age of ≥16 years; (b) acute fractures that require surgical treatment, including pelvic, femoral, tibial, fibular, ankle, and foot injuries; and (c) preoperative, postoperative, and 1-month postoperative ultrasonographic results are available.
The exclusion criteria were as follows: fractures with delayed treatment (>3 weeks from injury to surgery), open soft tissue fractures, serious medical problems that make the patient unsuitable for surgery, and poor treatment compliance. We excluded delayed fractures because of the long interval between the fracture onset and operation, and the complex surgical procedure required. In addition, patients with anticoagulation contraindications (at high risk of stroke or bleeding) were excluded from the study.
Treatment
All the patients who were admitted to the hospital were routinely assessed using the Risk Assessment Profile for Thromboembolism score for thromboembolism risk. 12 At the same time, we also assessed whether the patients had anticoagulation contraindications. For patients without anticoagulation contraindications, LMWH (3800 IU/0.4 mL once per day, Fraxiparine; Glaxo Wellcome Production, GlaxoSmithKline) was subcutaneously injected to prevent DVT. Then, Doppler ultrasonography was performed to screen for DVT. The patients with DVT received subcutaneous injections of LMWH (3800 IU/0.4 mL, twice per day). The therapeutic anticoagulation protocol was guided with hospital consultation from the department of vascular surgery. When the results of the preoperative ultrasonography performed by the department of vascular surgery showed central or mixed thrombosis, an inferior vena cava filter was used to prevent fatal pulmonary embolism if needed. The anticoagulant therapy was discontinued 12 hours before surgery and resumed 24 hours after surgery. When the patient was discharged, the protocol was changed to rivaroxaban therapy (10 or 20 mg once daily, Xarelto; Bayer HealthCare AG) until 35 days after operation. 13
In addition, mechanical thromboprophylaxis (foot intermittent pneumatic compression sleeve, 20 minutes twice a day) was used. Blood samples were collected on admission (2 hours after admission), 1 day before operation, and 1 and 5 days after operation, and 30 days after operation. The aim testing indexes included
We used Doppler ultrasonography to diagnose DVT. The diagnostic criterion for fresh thrombosis was the presence of a constant intraluminal filling defect. 14 The patients were examined before, after operation, and 1 month after surgery. All the patients underwent ultrasonography in both lower limbs 1 day before the planned surgery and on the third to the fifth day after operation, and 1 month after surgery. The DVT cases were classified into 3 types as follows: central (femoral and iliac veins), peripheral (calf muscle, fibular, and anterior/posterior tibial veins), and mixed thrombosis (both central and peripheral thromboses). 13 According to their ultrasonography results, the patients were divided into 2 groups: a thrombosis group and a non-thrombosis group.
Statistics Analyses
Statistical analysis was performed using SPSS Version 19.0 (SPSS Inc.). The incidence was reported as a percentage. An independent-sample t test and a χ2 test were used for the statistical analyses. If the P value of a factor was <.1 in the univariate analysis, then the variable was selected for multivariate analysis. A multivariate analysis was used to detect the risk or protective factors. The difference was considered to indicate statistical significance if the P value was less than .05.
Results
Patient Demographic and Clinical Characteristics
A total of 404 patients who met the inclusion criteria were included in the study, between June 1, 2016, and March 31, 2017. Of the patients, 208 were female and 196 were male, aged 18 to 88 years. In total, 193 patients had left lower extremity fractures; 185, right lower extremity fractures; 5, bilateral lower extremity fractures; and 21, pelvic and acetabular fractures. Of 263 knee proximal fractures, 69 were around the knee and 72 were distal to the knee. Combined multiple injuries were diagnosed in 50 patients. The number of patients with specific comorbidities was as follows: 68, primary hypertension; 60, coronary heart disease; 32, diabetes; and 14, cerebral stroke. None of the patients developed pulmonary embolism in the hospital.
Incidence of DVT on Preoperative Ultrasonography
In the preoperative ultrasonography result, 143 patients had thrombosis (35%; Table 1). Of all the DVT cases, 31% were peripheral; 1%, central; and 3%, mixed. Peripheral DVT constituted 88% (126/143) of all the DVT cases. Symptomatic DVT was found in 24 patients (17%).
Patient Characteristics According to Preoperative Ultrasound.a

Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; CRP, C-reactive protein; HGB, hemoglobin; HCT, Hematocrit.
a Coronary heart disease includes chronic myocardial ischemia, ST segment changes without clinical symptoms, and delayed myocardial infarction in electrocardiograms. Stroke includes fresh and delayed cerebral ischemia and hemorrhage in computed tomography or magnetic resonance imaging.
Of the 26 patients with bilateral limb or pelvic fractures, 4 (15%) had evidence of DVT. Among the remaining 378 cases, DVT occurred in 139 (37%). Of the 139 patients, 93 had DVT in the injured ipsilateral lower extremity, 20 had DVT in the uninjured contralateral lower extremity, and 26 had DVT in both lower extremities. The incidence of DVT on the uninjured side was 12% (46/378), accounting for 33% (46/139) of all the preoperative DVT cases. The multivariate analysis revealed that age (odds ratio [OR]: 1.03; 95% CI: 1.01-1.04; P = .000) was an independent risk factor for preoperative DVT (Table 2).
Multivariate Analysis of Preoperative, Postoperative, and 1-Month Postoperative DVT.

Abbreviations: ASA, American Society of Anesthesiologists; DVT, deep vein thrombosis; OR, odds ratio; SE, standard error.
Incidence of DVT on Postoperative Ultrasonography
In the postoperative ultrasonography result, thrombosis was found in 223 patients (55%; Table 3). Of all the DVT cases, 49% were peripheral; 1%, central; and 5%, mixed. Peripheral DVT constituted 88% (196/223) of all the DVT cases. Symptomatic DVT was found in 56 patients (25%).
Patient Characteristics According to Postoperative Ultrasound.

Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; CRP, C-reactive protein; EF, external fixation ORIF, open reduction internal fixation; THR, total hip replacement; HGB, hemoglobin; HCT, Hematocrit.
Of the 26 patients with bilateral limb or pelvic fractures, 13 (50%) had evidence of DVT. Among the remaining 378 cases, DVT occurred in 210 (55%). Of the 210 patients, 128 had DVT in the injured ipsilateral lower extremity, 18 had DVT in the uninjured contralateral lower extremity, and 64 had DVT in both lower extremities. The incidence of DVT on the uninjured side was 22% (82/378), accounting for 39% (82/210) of all postoperative DVT cases. The results of the multivariate analysis showed that age (OR: 1.04; 95% CI: 1.03-1.05; P = .000), blood loss (OR: 1.001; 95% CI: 1.000-1.002; P = .018), and ASA classification (OR: 2.07; 95% CI: 1.16-3.72; P = .014) were independent risk factors for postoperative DVT (Table 2).
Incidence of DVT on 1-Month Postoperative Ultrasonography
The postoperative ultrasonography result showed that 161 patients had thrombosis (40%; Table 4). Of all the DVT cases, 36% were peripheral; 1%, central; and 3%, mixed. Peripheral DVT constituted 91% (146/161) of all DVT cases. Symptomatic DVT was found in 10 patients (6%).
Patient Characteristics According to 1-Month Postoperative Ultrasound.

Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; CRP, C-reactive protein; EF, external fixation; ORIF, open reduction internal fixation; THR, total hip replacement.
Of the 26 patients with bilateral limb or pelvic fractures, 6 (23%) had evidence of DVT. Among the remaining 378 cases, DVT occurred in 155 (41%). Of the 155 patients, 81 had DVT in the injured ipsilateral lower extremity, 26 had DVT in the uninjured contralateral lower extremity, and 48 had DVT in both lower extremities. The incidence of DVT on the uninjured side was 20% (74/378), accounting for 48% (74/155) of all 1-month postoperative DVT cases. The results of multivariate analysis showed that age (OR: 1.05; 95% CI: 1.03-1.07; P = .000) was an independent risk factor for 1-month postoperative DVT (Table 2).
Perioperative Changes of DVT Before and After Operation
The perioperative changes of DVT before, after, and 1 month after operation are shown in Figure 1. Of all 404 patients, 66% showed no changes in DVT status from pre- to post-op ultrasonography (40.10% no DVT, 24.26% peripheral, 0.25% central, and 0.99% mixed DVT). Moreover, 5% (3.96% peripheral, 0.25% central, and 0.5% mixed DVT) of the patients who had preoperative DVT no longer had thrombosis postoperatively. In addition, 25% (22.03% peripheral, 0.74% central, and 1.73% mixed DVT) of the patients progressed from having no thrombosis preoperatively to having peripheral, central, or mixed DVT postoperatively.
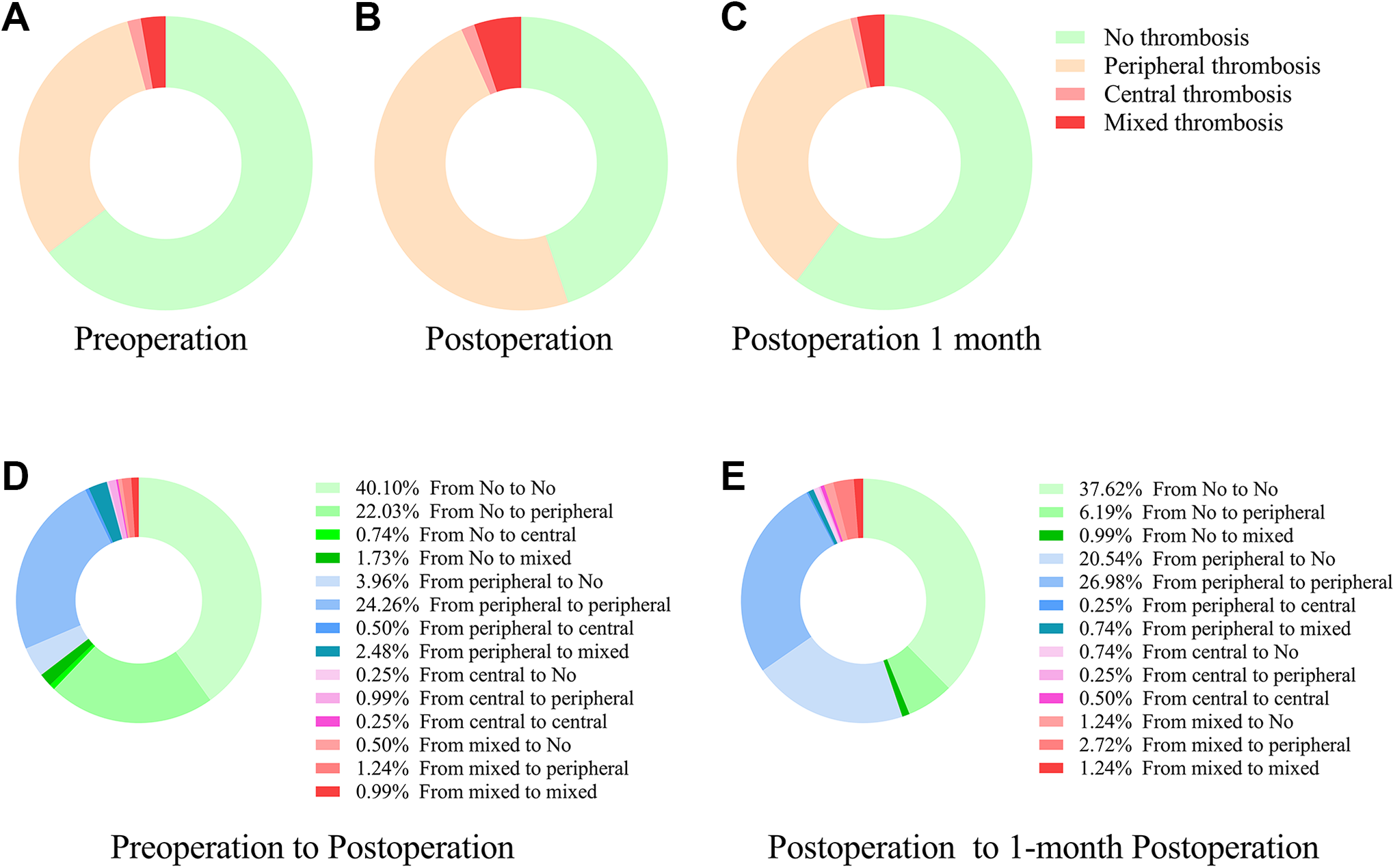
The incidence of preoperative deep vein thrombosis (DVT) (A), postoperative DVT (B), 1-month postoperative DVT (C), and the perioperative changes of DVT from pre-operation to post-operation (D), and from post-operation to 1-month post-operation (E).
Of the 404 patients, 66% (37.62% no DVT, 26.98% peripheral, 0.50% central, and 1.24% mixed DVT) showed no changes after hospital discharge. Moreover, 23% (20.54% peripheral, 0.74% central, and 1.24% mixed DVT) of the patients who had postoperative DVT no longer had thrombosis postoperatively 1 month. In addition, 7% (6.19% peripheral and 0.99% mixed DVT) of the patients progressed from having no thrombosis postoperatively to having peripheral or mixed DVT 1-month postoperatively. From the postoperative to the 1-month follow-up ultrasound, there was a decrease in overall prevalence of DVT from 223 (55%) to 161 (40%).
Discussion
We investigated the effects of LMWH administration followed by rivaroxaban therapy in the prevention of DVT in patients with lower extremity fractures. Our basic findings were as follows: (a) the incidence of perioperative DVT decreased over time. The incidence of postoperative DVT was 55% and that of 1-month postoperative DVT was 40%. (b) The incidence rates of preoperative, postoperative, and 1-month postoperative DVT on the uninjured side were 12%, 22%, and 20%, respectively. (c) The most variable DVT was peripheral DVT, which constituted 88%, 88%, and 91% of all preoperative, postoperative, and 1-month postoperative DVT cases, respectively. (d) Age was an independent risk factor for perioperative DVT.
Many factors contribute to the formation of thrombosis after trauma, 15,16 including age, sex, hypertension, diabetes, cerebral infarction, myocardial infarction, and so on. These are risk factors for thrombosis, especially in cases of fracture and surgery. 17,18 In this study, age showed a close relationship with thrombosis. Further, sex also plays an important role in thrombosis but is not an independent risk factor. Many studies have shown that females had high risk of DVT. 13,14 Increasing evidence suggests that women had higher platelet activity levels than men, 19 –21 and estrogen likely plays a crucial role in the transcriptional regulation of coagulation protein genes. 22
This study is the first research on perioperative changes of DVT before, after, and 1 month after the surgery. In this study, we found that the incidence and severity of DVT were highest after the surgery. Compared with the preoperative incidence of DVT, the postoperative incidence of DVT tended to increase. The number of DVT cases increased by 89 new peripheral DVT cases, 7 new mixed DVT cases, and 3 new central DVT cases. Immobility due to severe pain after fracture and operation may cause venous stasis in the lower extremities, thus increasing the risk of DVT in these patients. 23 Twenty-nine new DVT cases (7%) occurred in the patients receiving rivaroxaban therapy, of which 25 were peripheral and 4 were mixed. We found 17 hip fractures, 3 patellar fractures, 5 tibial and fibular fractures, 2 pelvic and acetabular fractures, and 2 distal femoral fractures. Through a review, we found that most of these patients were elderly and confined in bed for a long time. This serves as a reminder of the importance of early weight bearing.
The incidence at 1 month after surgery showed a decreasing tendency as compared with that after operation. Selby et al reported a significant hypercoagulability within the first 24 hours after trauma, a state that was maintained for 5 to 14 days. 24 Meissner et al suggested that this hypercoagulation state persists for at least 1 month after injury in 80% of patients. 25 This may explain why 40% of patients had resisted DVT at 1 month after surgery despite the use of rivaroxaban for prophylaxis or therapy.
We also divided the patients according to fracture site. We found that the incidence of preoperative thrombosis was similar among the hip, knee, and ankle fractures. The incidence rates of DVT in hip and knee fractures were, respectively, 60% (158/263) and 59% (41/69) immediately after surgery, and 44% (117/263) and 41% (28/69) 1 month after surgery. The incidence rates of DVT were lower in the ankle fractures. Basques et al reported that the incidence of DVT in ankle factures was 0.8%, 26 and Pelet et al reported an incidence rate of 2.66%. 27 Shin et al reported an 11.1% incidence rate of hip preoperative DVT. 1 These findings suggest that fractures in the hip and knee are more prone to DVT than those in other regions of the lower extremity.
Peripheral DVT is the most variable form in the early stage and can occur in the calf muscle veins, fibular vein, and anterior/posterior tibial vein. Peripheral DVT occurred in 31% (126/404) of the patients before surgery, 49% (196/404) immediately after surgery, and 36% (146/404) at 1 month after surgery. Peripheral DVT accounted for 88%, 88%, and 91% of all preoperative, postoperative, and 1-month postoperative DVT cases, respectively. Palareti et al reported that the proportions of peripheral DVT cases ranged from 23.4% to 59.7%. 28 The calf muscle veins are among the most frequent areas for the development of DVT. 29 This is the reason why peripheral DVT is variable and changeable. Galanaud et al reported that the mortality rate is significantly lower in patients with isolated peripheral DVT than in those with proximal DVT. 30 Thus, peripheral DVT is relatively safer than proximal DVT, but peripheral DVT must be prevented from transitioning to proximal DVT or mixed DVT.
This study has some limitations. First, Doppler ultrasonography, which was used in the study, is not the gold standard method for the diagnosis of DVT. However, it is highly convenient and noninvasive as compared with radiography, and orthopedists have accepted ultrasonography as a diagnostic modality for DVT. Second, we did not specially analyze for symptomatic DVT because, in a recent study, asymptomatic DVT accounted for most overall DVT cases. 28 In this study, we investigated the perioperative changes of DVT and analyzed the overall incidence of DVT but not symptomatic DVT.
Conclusion
In conclusion, the incidence of perioperative DVT decreased over time in the patients who received anticoagulation treatment. Age was an important risk factor for perioperative DVT.
Footnotes
Authors’ Note
Bin-Fei Zhang and Peng-Fei Wang contributed equally to this work. Z.Y., Z.K helped in conceptualization of the study; F.C., S.K., Q.S.W., L.J.H., K.C., X.X., Y.K., and L.P. contributed for data curation; Z.B.F. and W.P.F contributed to the formal analysis; Z.B.F. and W.P.F contributed to the Roles/Writing-original drafting of the manuscript. The survey was implemented by Xi’an Honghui Hospital. According to relevant regulations, the data could not be shared. The study was approved by the ethical board of Xi’an JiaoTong University (No. 2014026).
Acknowledgments
Bin-Fei Zhang especially wishes to thank his wife Jiao Wang and families, who have given him persisting courage and confidence on the road of academic research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Social Development Foundation of Shaanxi Province (grant numbers 2017-ZDXM-SF-009, S2019-YF-YBSF-0003 and 2020JQ-961).