
Abstract
Inflammation and coagulation pathways are implicated in circulatory disease, but their interaction has not been completely deciphered yet. In this study, we investigated the association of coagulation and inflammation indices (activated clotting time [ACT], C-reactive protein, neutrophils) in hospitalized patients. Blood samples were drawn from consecutive patients at admission and at 48 hours for the assessment of the aforementioned parameters (n = 63). Healthy controls matched for sex and age were also examined (n = 39). Activated clotting time positively correlated with CRP on admission (r = 0.354, P = .005), while the correlation was more robust on the second day (r = 0.775, P < .001). Activated clotting time was significantly more prolonged in patients with abnormal CRP or abnormal absolute neutrophil count compared to patients with normal inflammatory markers (U = 55.0, P < .001 and U = 310.5, P = .035, respectively). At 48 hours, a positive relationship was observed between ACT and relative percentage of neutrophils (r = 0.358, P = .004). These findings suggest a link between ACT and inflammation indices for the first time in humans. Further research is needed to determine whether these interrelations can be used to improve patient management.
Introduction
The acute phase response to inflammation is a prominent systemic reaction mediated by the activation of inflammatory cells and release of cytokines and acute phase proteins. 1 The number of circulating neutrophils and the level of C-reactive protein (CRP) are considered as classical biomarkers of inflammation and commonly recognized diagnostic tools for this acute phase response. 2 Inflammatory process also results in the expression of procoagulant molecules on the vascular endothelium and stimulation of white blood cells (WBCs), leading to activation of coagulation pathways. 3,4 Subsequent consumption coagulopathy and decreased levels of coagulation factors have been suggested to cause prolongation of clot-based assays of coagulation in severe inflammatory conditions. 5 In this respect, it has been proposed that systemic inflammation is followed by activation of the coagulation system, and conversely, components of the coagulation system significantly affect the inflammatory cascade/balance. 6
Several coagulation parameters have been used to examine the hyper- or hypocoagulant status of the patients with systemic inflammation. Prothrombin time with international normalized ratio (INR), activated partial thromboplastin time (aPTT), activated clotting time (ACT), fibrinogen concentration, and
Activated clotting time can be impacted by a wide variety of variables (such as drugs, inflammation, cellular activation), yet it is universally used for assessing patient hemostasis. It has the advantage that it measures a whole blood sample and the time for the whole blood to clot. It evaluates the intrinsic coagulation pathway concurrently with the effect of phospholipids and platelets number in clot formation and thus determines patient hemostasis, in contrast to PT, aPTT, thrombin time (TT), and fibrinogen level that assess just hemostasis without the incorporation of tissue materials in systemic circulation and in coagulation cascade. 8,9
Technically, ACT requires less blood sample, is faster, and is more applicable to nonlaboratory personnel, while the danger of sample deterioration is reduced when compared to other traditional coagulation assays such as PT and aPTT. 8 –12
Despite the clear benefits of ACT as opposed to other coagulation assays in determining patient hemostasis and not plasma hemostasis, the only available data supporting the relation between ACT and inflammation come from animal studies. 13
The aim of the study was to investigate for the first time in humans the relation of ACT with established markers of inflammation in patients admitted to an intensive care unit (ICU) due to cardiovascular diseases and/or respiratory failure.
Methods
In this prospective observational cohort study, we included 63 consecutive patients admitted to a tertiary medical ICU from October 2017 to June 2018. The reason for admission was acute coronary syndrome (ACS), heart failure, rhythm disturbances, myocarditis, and/or respiratory failure. Patients with known coagulopathy, with known systemic inflammatory disease, with indication for long-term treatment with anticoagulants, with severe hepatic failure or kidney dysfunction (glomerular filtration rate <30 mL/min/1.73 m2), and requiring treatment with hemodialysis were excluded from the study. Blood samples for the determination of the markers of inflammation and coagulation assays were drawn at the time of admission and at 48 hours during hospitalization. α “2-syringe” technique was used discarding at least 2 mL of blood. In patients in need of short-term anticoagulation treatment, blood was drawn before the initiation of anticoagulants and 12 or 24 hours after the last administered dose of unfractionated heparin (UFH) or low-molecular-weight heparin (LMWH), respectively. Patients with ACS were sampled before the initial anticoagulant bolus and were all revascularized within 24 hours, permitting the interruption of the anticoagulation. Complete blood count (total and differential WBC counts, platelet count) was performed via an ADVIA SIEMENS automated analyzer. C-reactive protein was measured by an immunofluorescent assay using the B•R•A•H•M•S CRPus KRYPTOR kit, while aPTT and INR were determined with the use of a BCS XP system (Siemens). For ACT measurement, venous blood was collected into a cartridge with liquid suspended kaolin activator and immediately (within 1 minute) placed into the ACT plus Automated Coagulation Timer System (Medtronic) device. In patients who previously received parenteral UFH or LMWH, blood sampling took place at least 12 hours and 24 hours after discontinuation of the drug, respectively. As a control group, we used 39 healthy adults matched for sex and age, visiting the preventive cardiology outpatient clinic and were tested for the aforementioned parameters only once. The study design was approved by the hospital research ethics committee.
Statistical Analysis
Data are expressed as mean ± 1 SD for continuous variables and as percentages for categorical data. The Kolmogorov-Smirnov test was used in order to assess the normality of distributions. Continuous variables were compared using the unpaired t test and the nonparametric Mann-Whitney U test as appropriate. All performed tests were 2 sided. Correlation of parameters of coagulation with markers of inflammation was investigated using correlation coefficient. The correlation coefficients were determined using ln-transformed data. A receiver operating characteristic (ROC) curve analysis was implemented in order to evaluate the reliability of the coagulation markers in discriminating normal from elevated markers of inflammation. The Youden index was used to identify the optimal cutoff points, thereby determining the sensitivity and specificity. A P value <.05 was used for determination of statistical significance. All statistical analysis was performed using SPSS (version 20.0; SPSS Inc).
Results
Sixty-three patients (study group) were included in the study and were compared to 39 patients (control group). Table 1 shows the demographics, the clinical syndrome, and the outcome of both study and control groups. Activated clotting time, CRP, and INR of the studied group were significantly increased both on admission and after 48 hours compared to the controls, while aPTT showed no significant difference between groups (Table 2). On admission, ACT was correlated with CRP (r = 0.354, P = .005; Figure 1A), with the correlation to be more robust on the second day (r = 0.775, P < .001) of hospitalization (Figure 1B). On the second day of hospitalization, ACT was significantly more prolonged in patients with abnormal CRP or abnormal absolute neutrophil count compared to patients with normal markers of inflammation (U = 55.0, P < .001 and U = 310.5, P = .035, respectively; Figure 2). Interestingly, this finding was not observed on admission (U = 106.0, P = .363).
Demographics and Clinical Syndrome of Patients Included in the Study.

Abbreviations: ACT, activated clotting time; ACS, acute coronary syndrome.
Inflammation and Coagulation Parameters of the Control and Study Group (at Admission and 48 Hours Later).a

Abbreviations: ACT, activated clotting time; aPTT, activated partial thromboplastin time; CRP, C-reactive protein; INR, international normalized ratio; NEU, neutrophil count; PLT, platelet count; WBC, white blood cell count.
a The P value refers to the comparison between the control group and the mean of the 2 measurements of the studied group. Data are given as mean ± SD or median (interquartile range).
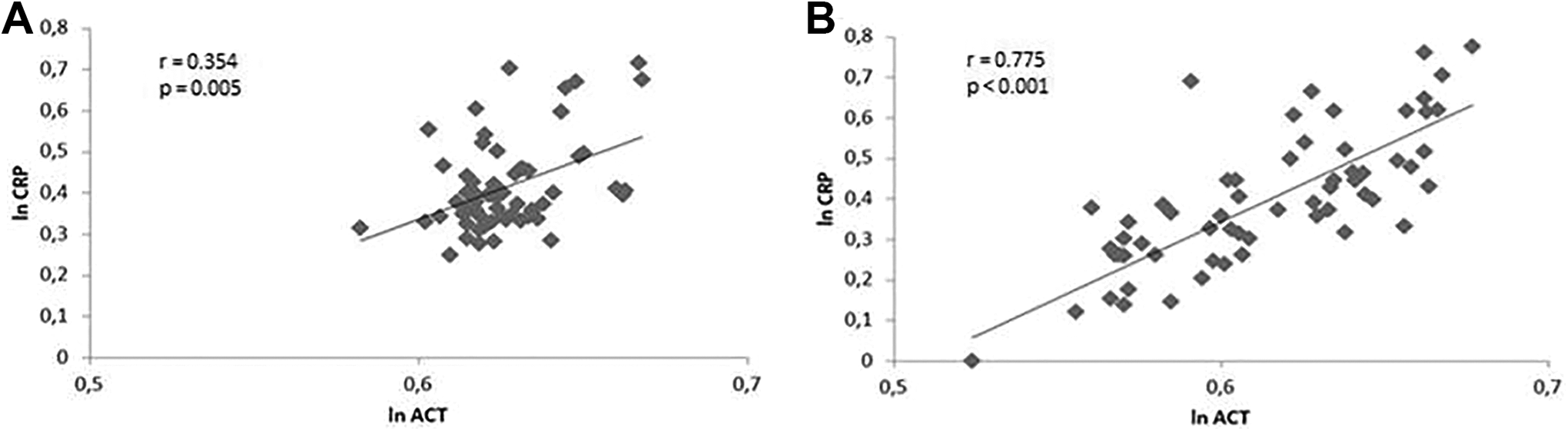
Scatterplot reflecting association of the natural log (ln) of the activated clotting time (ACT) and C-reactive protein (CRP) in the study population (n = 63) at admission (A) and on the second day (B).

Box plots of activated clotting time (ACT) for normal (A) and elevated (B) C-reactive protein (CRP) at 48 hours.
The area under the calculated ROC curve, constructed by plotting ACT against elevated CRP, was 0.931 (P < .001), demonstrating good performance. An ACT value >116.5 seconds was identified as the optimal cutoff point for the prediction of elevated CRP, with a sensitivity of 82% and a specificity of 94% (Figure 3).
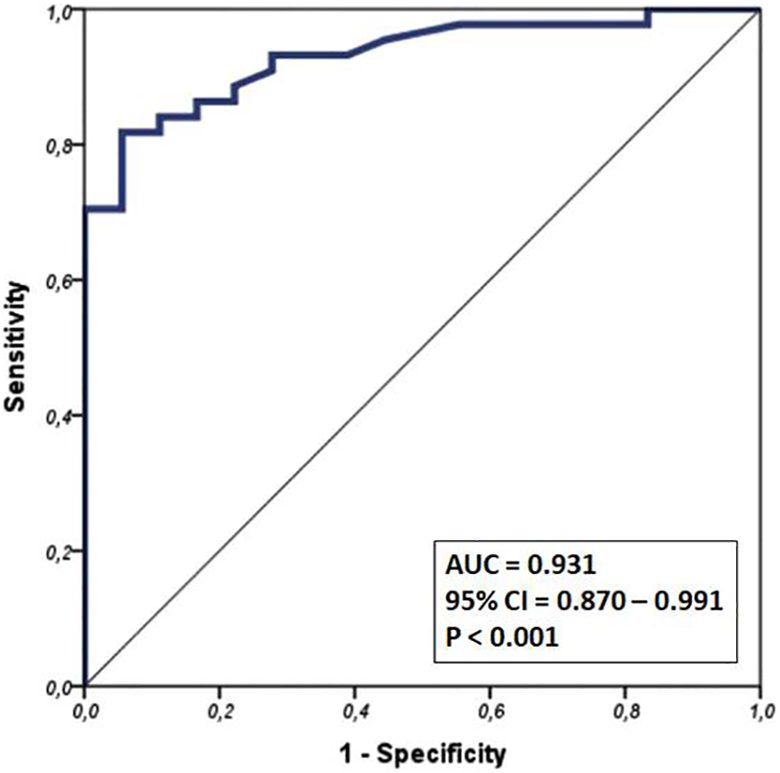
Receiver operating characteristic (ROC) curve constructed by plotting activated clotting time (ACT) against elevated C-reactive protein (CRP) and corresponding area under the curve (AUC).
At 48 hours, a weak positive relationship was observed between ACT and relative percentage of neutrophils (r = 0.358, P = .004) while ACT was negatively correlated with lymphocytes count (r = −0.366, P = .003). With regard to the remaining parameters, no relationship was found with inflammatory markers, except for INR which showed a weak correlation with CRP at 48 hours (r = 0.326, P = .01).
In the control group (n = 39), ACT ranged from 70 to 99 seconds with a median value of 83 seconds. C-reactive protein had a median of 3.9 mg/L (range: 0.5-9.0 mg/L). All CRP and ACT measurements were within normal range, and no correlation was noted between them.
Discussion
The results of the present study show for the first time that in a selected group of patients who need hospitalization in the ICU there is a strong positive correlation between CRP and ACT 48 hours postadmission. Elevated ACT values at 48 hours interrelated with higher CRP values in the group of hospitalized patients, while at the time of admission, the correlation was also present albeit weaker. This finding could be attributed to the consumptive coagulopathy observed in systemic inflammatory syndromes and/or inflammatory response following exacerbations of cardiovascular disease such as ACS. 14 –17 Several studies suggest that endothelial injury along with hemolysis and the emancipation of phospholipids, platelets, and other metabolic components in systemic circulation can trigger an inflammation-induced procoagulant activation and finally result in consumption coagulopathy and decreased levels of coagulation factors. 5,18 –21 This explains the prolongation of the time to clot formation in coagulation screens in critically ill patients. 14
The exact timing at which inflammatory-induced activation of coagulation evolves to systemic hypocoagulation is not known. 22 Various studies support that a time period of hours is frequently required for the detection of alterations in traditional plasma coagulation parameters indicating the establishment of intravascular coagulopathy, but the broad pathophysiology of the phenomenon, the underlying disease, the concomitant medication, and clinical status of the patient can lead to significant time variations. 18 –20,23 –26 Moreover, none have used ACT as a marker of upcoming or clinically established systemic consumptive coagulopathy in humans to our knowledge. Based on our results, we assumed that coagulation derangement requires several hours and up to 48 hours to develop, and thus, ACT prolongation was not apparent on admission. The excellent performance of ACT in predicting elevated CRP values, as concluded by the ROC curve, implies a potential role for ACT in the clinical setting of inflammation. A high ACT value, above 116.5 seconds, was found to predict the contemporarily elevated CRP with excellent specificity and a satisfactory sensitivity and can therefore provide valuable clinical information to the attending physician with regard to the underlying inflammatory status of the patient. Furthermore, the above results raise the question if in cases where high levels of inflammatory activation are expected (such as coronary bypass surgery), high ACT values, heparin treatment, and dosing should also be evaluated and tailored, respectively, in the context of a triggered and ongoing inflammatory process.
Activated clotting time at 48 hours correlated with the relative percentage of neutrophils. This finding was statistically weak and no relation was established with the absolute number of WBCs or neutrophils. However, neutrophil count and type are affected by several factors, irrespective to the inflammatory status, namely catecholamines, glucocorticoids, antibiotic therapy, or cancer, and thus is a nonspecific marker. 27 –30
Activated PTT is also known to be prolonged in severe systemic inflammatory response syndrome complicated by thrombotic coagulopathy. 31,32 In our study, no significant correlation was observed between aPTT and inflammatory indices. The fact that ACT is influenced by more variables related to hemostasis than aPTT such as platelet number and function or phospholipids could offer a possible explanation.
Clinical Implication
Activating clotting time is a quick and easily accessible to nonlaboratory personnel coagulation test that requires small amounts of blood and carries less risk for sample degradation with time, in contrast to other commonly used coagulation indices. Nevertheless, as a method, it provides a more thorough estimation of patient’s hemostasis, incorporating the platelets and phospholipids interaction in the intrinsic coagulation pathway integrity and in thrombus formation, when compared to other traditional assays of coagulation such as PT, aPTT, TT, and fibrinogen that require longer time periods for accessible results, assess only plasma hemostasis, and do not evaluate the integration of tissue materials in systemic circulation and coagulation cascade. A quick assessment of the coagulation status, the determination of a possible underlying inflammation, and the interrelation between them are of utter importance for critically ill patients. Additionally, clinicians ought to be constantly alert for signs of rapid clinical deterioration, especially in patients requiring anticoagulation treatment. Assessment of ACT could offer a swift evaluation of the inflammatory status in selected groups of patients, although further studies are required to certify the above hypothesis.
Study Limitations
Certain limitations of the present study should be acknowledged. Firstly, this study represents a single-center cohort report of consecutive patients admitted in the ICU. Secondly, other parameters of coagulation such as clotting factors or antithrombin were not measured. However, the advantages and the characteristics of ACT when compared to most of the other clotting factors offer a potential clinical benefit in the choice of the specific agent. As in the present study, we focused mainly on the correlation of easily applicable, widespread assays, we suggest that prospective research efforts on the subject could include the analysis of coagulation factors, protein C, protein S, antithrombin, and cytokine levels. Future studies focusing on the in-depth interpretation of selective tuning and specificity of these assays might provide more cues toward the development of novel therapeutic strategies during abnormal coagulation and inflammatory process.
Conclusion
In patients admitted to the ICU, there is a strong correlation between ACT and CRP, which is most prominent 48 hours postadmission. Activated clotting time could be used to predict elevated CRP values with a good diagnostic yield. High ACT values in the absence of anticoagulant medication or known coagulopathy could enhance awareness regarding a coexistent inflammatory process.
Footnotes
Authors’ Note
Andreas Synetos, Konstantinos Tampakis, and Hector Anninos contributed equally as co-second authors. The study fulfills the ethical requirements of the Declaration of Helsinki, regarding the research with human subjects, and was approved by the hospital’s ethical committee. Informed consent was obtained from all individual participants who were included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.