
Abstract
Nowadays, the development of factor VIII and IX inhibitors in patients with hemophilia is considered as the most challenging in the treatment of hemophilia. Immune tolerance induction (ITI) therapy is an approach for eradication of inhibitors. Some ITI protocols are routinely in use for the eradication of inhibitors in patients with hemophilia. Moreover, such a therapeutic regimen may facilitate the tendency to reduced bone density in patients with inhibitor. This study scheduled to investigate whether that predisposing role of ITI protocols with an immunosuppressive agent has considered or not. By a literature review, published ITI protocols in hemophilia with inhibitors were evaluated. Among them, 51 papers found and studied thoroughly. None of them had performed the bone mineral examination in patients with hemophilia and inhibitor under treatment. Since there are 2 coexisting facilitating factors in these protocols, considering the bone mineral density study for patients with inhibitor who are undergoing ITI protocols with an immunosuppressive agent is recommended.
Keywords
Introduction
Hemophilia, the most common bleeding disorder, has a prevalence of around 400 000 individuals worldwide. 1,2 Different genetic abnormalities in factor VIII and IX genes terminate to the absence or reduced plasma levels of factor VIII and IX in the blood. 3 These diverse defects translate to various types of bleeding manifestations in the clinical aspect. The standard therapeutic approach is replacement therapy using plasma-derived or recombinant factor VIII and IX concentrate. The main adverse events of replacement therapy include the development of an inhibitor, the risk of thrombosis, and allergic reaction. The development of inhibitors is considered the most challenging topics in hemophilia care in the current decade. 4 Inhibitors neutralize infused coagulation factor concentrates and makes it an extremely challenging complication in the management of hemorrhagic episodes. 5 It causes treatment of hemorrhagic episodes in hemophilia more exigent topics and also the economically more expensive treatment for the health providers’ system. 4,6 Improving health and safety surveillance are noticeable topics in a lifelong disease such as hemophilia. 7 Hence, recognizing, evaluating, and communicating treatment-related adversarial complications are particularly important and should be monitored as early as possible.
Inhibitors in Hemophilia
Development of inhibitors in hemophilia is a multifactorial process that dynamically comprises inherited factors (ABO blood group, 8 ethnicity, 9 human leukocyte antigen, 10 haplotype, 11 type of factor VIII or factor IX mutations, 12,13 and family history of developing inhibitors 14 ) and environmental factors (infection and vaccination, 15 –17 type of infused coagulation factor, 18 and age at start of treatment). 8,4,19 About 30% of patients with severe hemophilia A, 0.9% to 7% of patients with moderate and mild hemophilia A, 20 and around 3% to 4% of individuals with severe hemophilia B develop inhibitors. 21 –23 The development of inhibitors significantly complicates the control of hemorrhagic episodes in patients with hemophilia and makes challenges for hematologists because bleeds may not respond to conventional replacement therapy. 24,25 Therefore, the development of inhibitors is associated with poor quality of life, higher morbidity rate, and a higher cost of care for health provider systems. 26 Patients with a high dose of inhibitors (>5 Bethesda unit) do not respond to standard replacement therapy and need to be managed by a bypassing therapy. 27 The current treatment strategy for high-titer inhibitors comprises utilizing a bypassing agent, including activated prothrombin complex concentrates (APCC) FEIBA (Takeda Company) or recombinant activated factor VII (rFVIIa; NovoSeven; Novo Nordisk). 28 –30 In practice, the failure rate of treatment with bypassing agents ranges from 10% to 30%. 31 Another widely used therapeutic approach is immune tolerance induction (ITI), which leads to an eradication rate of about 70% to 85% of inhibitors. 32 Hence, ITI is the first choice option, especially in children with inhibitors. 33 –35 The hallmark protocols for ITI regimens include the Bonn, van Creveld, and Malmö protocols. 36 –38
Susceptibility of Patients With Severe Hemophilia to Reduced Bone Density
Several surveys have demonstrated reduced bone density in patients with severe hemophilia compared to age- and sex-matched control group. 39 –47 It seems osteopenia and osteoporosis in hemophilia is a multifactorial process. It needs to be cleared pathophysiologically. 48 Because patients with hemophilia usually experience hemophilia arthropathy secondary to bleeding into joints, they have low physical activity. This phenomenon may cause reduced peak of bone mass during childhood. It can translate to reduced bone density in later stages of life. 49 The influence of some blood-borne viruses, including hepatitis C virus and HIV, has brought up. 45 The development of osteoporosis in hemophilia increases the risk of bone fracture during normal daily activities when an occurrence of fracture seems to be an illogical event. 50 Despite these truths, hemophilia does not considered as a secondary cause of osteoporosis. 48
Clinical Question
What are the defects of ITI protocol with an immunosuppressive agent that are in employing for the eradication of inhibitors in patients with hemophilia regarding predisposing patients to reduced bone density? How can these defects be improved?
Method
The Strategy of Search
Assessment of the published articles was carried out to unravel whether the facilitator effect of ITI therapies with an immunosuppressive agent to reduced bone density has considered and paid attention or not. Hence, medical search engines of PubMed and Scopus were searched without any time limitation. The literature review was done on English language papers from the past till March 15, 2019. The following keywords were used for searching: “hemophilia A + hemophilia B + immune tolerance induction + ITI + immunosuppressive + inhibitor.” The authors screened the retrieved articles, relevance separately. All types of published articles or e-print of ahead papers, including original article, case series, case report, brief report, and letter to the editor that contains data on patient with hemophilia and inhibitors who underwent ITI protocol, entered to the study. The review articles that discussed ITI protocol and patients with hemophilia and inhibitors were not included in the study. All discrepancies and cross-checking of identifying papers were resolved in a debriefing session. From the target articles, some data were extracted, such as the type of hemophilia, number of treated patients, year of publishing data, type of administrated immunosuppressive agent, the country in which protocol was done, and whether bone density has done or not. And moreover, it was investigated whether the supplementary regimen for protection against reduced bone density has administrated or not?
Results
Overall, 196 related abstracts were identified through the search strategy. After deleting repeated titles, 114 abstracts were selected. Among them, 111 full texts were selected. All 111 full texts read to clear administration of an immunosuppressive agent as part of the ITI protocol and also evaluation of patients for reduced bone density. Among them, 12 review articles and 3 abstracts were excluded from the study. The whole 96 original articles were read. As reflected in the flow diagram of the study, 51 surveys had used at least one of the immunosuppressive agents in their ITI protocols, 37,51 -99 while 45 studies had used a version of ITI without any immunosuppressive agent (Figure 1). Among the 51 reported studies on the eradication of inhibitors in hemophilia A and B using an immunosuppressive agent or combination of them, the used immunosuppressive agents included mycophenolate mofetil, corticosteroid, rituximab, rapamycin, Solumedrol, dexamethasone, hydrocortisone, prednisolone, prednisone, cyclophosphamide, methylprednisolone, fluprednisolone, and cyclosporine A (Table 1). At the reviewing of articles, about 284 patients with hemophilia A, B, or acquired hemophilia had undergone one of the ITI protocols with at least an immunosuppressive agent in various countries across the world. There was no evidence of the detection status of bone density among studied patients. Moreover, no evidence found about prescription for supplementary calcium for the patients. Among the founded articles in this survey on published articles about the eradication of inhibitors, 29 studies had published between 2000 and 2018 and 22 articles published before 2000. Moreover, Sweden and the United States had reported the most studies (9 articles by each country).
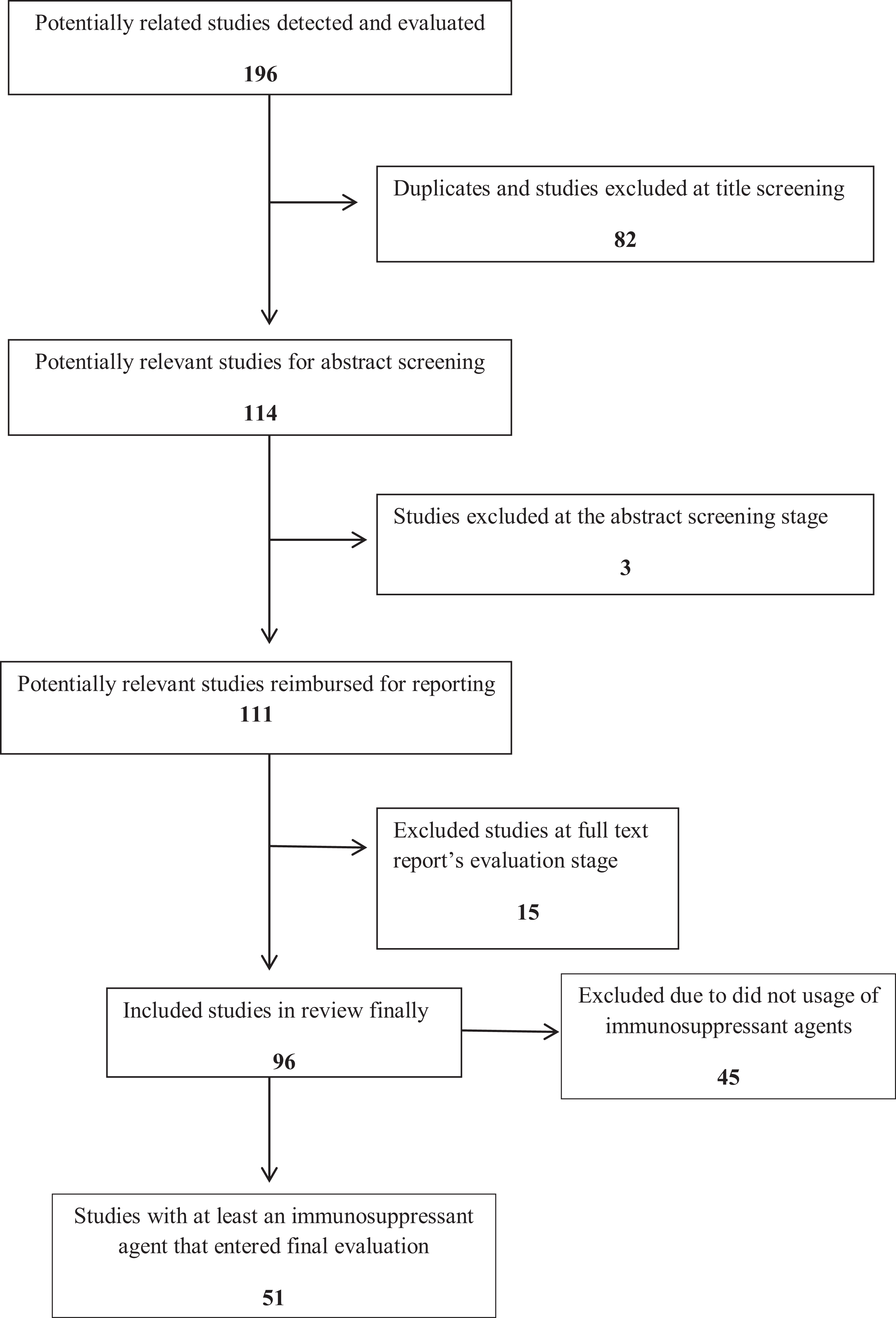
The inclusion and exclusion flow diagram of studies.
The List of Published Original Articles on Eradication of Factor VIII or IX Inhibitors by ITI Protocols, Including Immunosuppressant Agents Before November 2015.a

Abbreviations: AHA, acquired hemophilia A; BMD, bone mineral density evaluation; IV, intravenous; M, multicenter; MMF, mycophenolate mofetil; NC, not cited.
a In the current study, 11 cases have been reported, but only 1 case has received cyclophosphamide and prednisone.
bThe first author of this manuscript is Batlle J.
cOne family members exists in this study.
What Does the Reviewing of the Evidence Conclude?
The landscape of the treatment of patients with hemophilia has undergone very speedy and significant advances during recent decades. The various available therapeutic regimens span from plasma-derived coagulation factor concentrate to bypassing agents (rFVII and APCC). 100,101 The coagulation factor concentrates are switching from plasma-derived form to recombinant coagulation factors, and half-life extended coagulation factor. 102 Now bispecific monoclonal antibody that mimics the function of factor VIII (emicizumab) is on trial and usage in developed countries. 103 There are also multiple therapeutic regimens for eradication of inhibitors too. The ITI protocols consider as the mainstay of eradication of inhibitors in hemophilia. 104 Suppression of T cells, induction of T-cell anergy, inhibition of B cell, and usage of anti-idiopathic antibodies comprise the mechanism action of ITI protocol. 105 Hence, ITI protocols are in use with a 60% to 80% success rate in hemophilia A now. 106,107 On the other hand, there is no therapeutic agent that can provide 100% protection against all hemorrhagic episodes in all patients without concern about the development of inhibitors.
Discussion
Osteoporosis, a disease that involves reduced bone density, results in the impaired and abnormal texture of bone mass that may lead to unforeseen fractures during normal daily activities. Osteoporosis is a significant cause of mortality and morbidity in adults. Indeed, the balance between bone development during childhood and the subsequent bone loss during adulthood comprises the bone mass. The factors, such as smoking, alcoholism, thalassemia, hypogonadism, hematological malignancies, vitamin D deficiency, and some drugs such as exogenous glucocorticoid excess, anticoagulants of warfarin, and heparin, consider to be the secondary predisposing factors toward reduced bone density (RBD). Moreover, the risk of bone fracture correlates with bone architecture in various races, which is evaluated by fracture risk assessment tool (Frax).
Hemophilia presents with a bleeding tendency and reduced plasma levels of coagulation factors VIII and IX in the blood. 1 Some researchers have shown that there is reduced bone density both in the lumbar spine and the femoral bone of males who have hemophilia via several case–control trials. 41,48,108 Osteoporosis in various races’ groups of patients with hemophilia has adequately studied in evidence of the literature. Despite this, hemophilia has not been considered a cause of secondary osteoporosis yet. 109
Apart from this, the development of inhibitors of relevant transfused coagulation factors is a major challenge that complicates the treatments for hemophilia bleeding. There are various types of neutralizing antibodies that bind to relevant coagulation factors and may impair functions of coagulation proteins in the coagulation system. The frequencies of developing inhibitors have generally ranged from approximately 18% to 28% in hemophilia A. The predisposing factors for developing inhibitors determine the severity of hemophilia, the underlying genetic defects, the age of patients at the time of treatment onset, the type of infused coagulation factor concentrates (plasma derived or recombinant factors), and the ethnic background of patients.
Immune tolerance induction is a therapeutic protocol for the eradication of inhibitors in hemophilia. The specific function by which ITI works is not completely clear. Among the suggested targets, it seems that factor VIII-specific T and B cells are more significant. 110 The use of ITI therapy may require 12 months of treatment to observe improvements. It may require 2 years or longer period in more complicated patients with hemophilia and inhibitors. 111,112 Some ITI protocols comprise the use of one or more immune suppressant agents (corticosteroids, cyclophosphamide, etc). Additionally, glucocorticoid-induced osteoporosis has addressed entirely in the literature. 113,114 It seems safety, pharmacoeconomic, and efficacy aspects of ITI therapy need to be designated. 115 Hence, for patients with hemophilia and inhibitor who tend to have reduced bone density, when they undergo ITI protocol (with at least an immunosuppressive agent) for the eradication of inhibitors, it is expected that they will have a higher risk for reduced bone density.
The limitation of the current study includes restricting the search to English papers. Although English is the universal language for scientific reports of studies, there may be other published papers in this field and this topic in local languages has been missed in our literature review.
Conclusion
Various ITI protocols are in use for the eradication of factor VIII and IX inhibitors in patients with hemophilia A and B. Some of ITI protocols include one or more immunosuppressive agent that has known to be associated with the side effect of reduced bone density. On the other hand, it has demonstrated that patients with hemophilia tend to have reduced bone density secondary to various factors. These 2 ameliorating factors push patients with hemophilia and inhibitors who are receiving ITI protocols with an immunosuppressive agent toward reduced bone density. This gap has not considered in the treatment of the current patients and needs to pay attention as a part of the ITI protocols for the patients with hemophilia and inhibitors. The ultimate goal of this study is to follow patients with hemophilia and inhibitor about bone mineral status before beginning of any ITI protocol with an immunosuppressive agent. Apart from this, in future versions of ITI protocols, evaluation of bone mineral density would be taken account. According to the current literature review, there is a body of evidence that implies bone mineral density in patients with inhibitors has not been considered. It is, thus, clearly accepted that well-planned randomized trials will shed more light on this issue.
Future Prospects
At the moment, the bone mineral examination is not routinely performed for patients with hemophilia. At present, tendency to reduced bone density has demonstrated in patients with hemophilia. And moreover, immunosuppressive agents pave the way toward osteopenia, and it would be expected that bone mineral examination should to be done for them. In addition, for patients with hemophilia and inhibitors who want to eradicate inhibitors by an immunosuppressive agent, a supplementary regimen of calcium and vitamin D would be considered. The prevention of osteopenia in patients with hemophilia is very cheaper than treatment of broken bones in hemophilia. Hence, implementation of bone density examination as part of the ITI protocols will be beneficial for both patients and health provider systems.
On the other hand, it would be expected that hemophilia to be considered as a risk factor in Frax criteria assessment tool. As a part of the ITI protocols, it is a good idea and essential to perform bone mineral density scans and provide calcium, vitamin D supplements, or bisphosphonate and anti-RANKL as protective drugs to the patients. Finally, assessment of BMD before and after ITI therapy for patients with hemophilia and inhibitor is recommended.
Footnotes
Authors’ Note
Z.R. gave idea; extracted and reviewed the piece of literatures, concluded of the findings, revised, and approved final draft of the manuscript. H.M. searched the medical search engines, extracted, and reviewed the literature, concluded of the findings, and wrote the primary version of draft.
Acknowledgments
The authors would like to thank the Mashhad University of Medical Sciences for financial support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Mashhad University of Medical Sciences [grant number of 951533].