
Abstract
Shear stress (SS)-induced platelet activation is suggested as an essential mechanism of the acute coronary syndrome (ACS). We aimed to compare SS-induced thrombotic and thrombolytic activities among 3 treatment regimens in patients with ACS who underwent percutaneous coronary intervention (PCI). Patients were nonrandomly enrolled and treated with one of 3 regimens (TICA: ticagrelor 180 mg/d; RIVA: clopidogrel 75 mg/d and rivaroxaban 5 mg/d; CLP: clopidogrel 75 mg/d), administered in addition to aspirin (100 mg/d) for 30 days. The global thrombosis test was applied to measure SS-induced thrombotic (occlusion time [OT]) and thrombolytic activity (lysis time [LT]) at day 2 and 30. Aspirin reaction unit (ARU) and P2Y12 reaction unit (PRU) were simultaneously measured using VerifyNow. Group differences in the OT, LT, ARU, and PRU were evaluated. Seventy-five patients (25 patients in each group) finished 30 days of follow-up. Clinical and angiographic characteristics did not differ among the 3 groups, except ACS subtype and pre-PCI coronary flow. No major adverse cardiovascular events occurred in any group during follow-up. The OT and LT did not differ among the 3 groups at day 30 (OT: TICA, 447.2 ± 87.1 vs RIVA, 458.5 ± 70.3, vs CLP, 471.9 ± 90.7, LT: 1522.3 ± 426.5 vs 1734.6 ± 454.3 vs 1510.2 ± 593.9) despite significant differences in the PRU among the 3 groups. Shear stress–induced thrombotic and thrombolytic activities did not differ among the 3 investigated antithrombotic treatments.
Introduction
Potent platelet inhibition is a cornerstone in the management of acute coronary syndrome (ACS), and the role of thrombin beyond platelets has been revisited in the management of patients with ACS. Ticagrelor has demonstrated survival benefits for patients with ACS and has been recommended as a drug of choice in the current practice guidelines. 1 –3
Furthermore, recent studies suggest that the addition of very-low-dose rivaroxaban on top of aspirin and thienopyridine reduces cardiac and all-cause mortality compared to that achieved using a dual therapy of aspirin and thienopyridine. 4,5 Although these potent antithrombotic regimens are recommended in ACS, the use of these medications is limited in patients with a high risk of bleeding or specific drug side effects, such as shortness of breath. Clopidogrel (CLP) is still a reliable option, especially in patients who cannot be treated because of these limitations. 1,2
Acute coronary syndrome arises from coronary atherosclerosis with superimposed thrombosis. Shear stress (SS)-induced platelet activation has been reported as one of the main mechanisms of ACS. 6,7 Current platelet function tests, such as the VerifyNow test (Accriva Diagnostics, Inc, San Diego, California), show the degree of ex vivo platelet activation by chemical agonists. However, this methodology cannot reflect the SS conditions in ACS nor can it evaluate the effect of anticoagulants.
The global thrombosis test (GTT; Thromboquest Ltd, London, United Kingdom) is a comprehensive test of platelet reactivity, thrombin generation, and endogenous thrombolytic activity. The GTT evaluates both high shear-induced thrombotic reactions and subsequent thrombolysis by using nonanticoagulated blood samples. 8 –10 Recent prospective studies have shown that impaired endogenous thrombolysis can be detected in a significant number of patients with ACS using the GTT and that it is a reliable marker of future cardiovascular risk. 11 –13
Ticagrelor is the most commonly recommended P2Y12 inhibitor in ACS, and very-low-dose rivaroxaban is currently the only proven oral direct thrombin inhibitor in ACS, while CLP is still widely used in patients with ACS in real-world practice, especially in Korea. 14 –16 Nevertheless, a direct comparison of the antithrombotic efficacy under in vitro SS conditions among these 3 common strategies has not yet been performed. Therefore, we aimed to comprehensively compare the antithrombotic activities of ticagrelor (TICA), very-low-dose rivaroxaban with CLP (RIVA), and CLP using both the GTT and the VerifyNow test.
Methods
Participants
This nonrandomized prospective cohort study was performed at Seoul National University Bundang Hospital, Seongnam, Republic of Korea. Among the 452 patients who underwent percutaneous coronary intervention (PCI) due to ACS between April 2017 and January 2018, 81 were enrolled in the present study (Figure 1). We excluded patients with atrial fibrillation, previously treated with antiplatelet agents, at high risk of bleeding, or administered a glycoprotein IIb/IIIa inhibitor, as well as those who refused to participate in the study. The study protocol was reviewed and approved by the institutional review board. Written informed consent was obtained from all enrolled patients. Baseline clinical characteristics, angiographic findings, and laboratory data were collected during the hospitalization for ACS. Medication adherence was checked at the 30-day follow-up whether the patient completed taking medication during follow-up.

Study flowchart. ACS indicates acute coronary syndrome; GP IIb/IIIa, glycoprotein IIb/IIIa; SNUBH, Seoul National University Bundang Hospital.
Procedures
Percutaneous coronary intervention was performed according to standard techniques. Loading doses of aspirin (300 mg) and CLP (300 to 600 mg) or ticagrelor (180 mg) were administered before PCI, and the addition of low-dose rivaroxaban (2.5 mg twice a day) was done just after PCI according to physician’s decision. Drug compliance was evaluated using a patient diary. Blood samples were taken on day 2 and 30 after revascularization. Blood samples on day 2 were obtained after 12 to 24 hours from the study drug administration, according to previous studies. 17 –19 Aspirin (100 mg/d) was maintained irrespective of other antithrombotic medications, and the use of ticagrelor (90 mg twice a day), CLP (75 mg/d) plus rivaroxaban (2.5 mg twice a day), or CLP (75mg/d) was maintained for 1 month. Otherwise, patients were treated as per international and local guidelines for ACS management. 1,2 Global thrombosis test and VerifyNow were performed on day 2 and day 30 after revascularization.
Blood Sampling
Blood samples were directly obtained from the antecubital vein using a 21-G needle, with tourniquet loosening after vein puncture. The first 2 to 3 mL of blood was discarded to ensure accurate test results. The subsequent 8-mL sample was divided into four 3.2% citrated tubes (2 mL each) for the VerifyNow test. Next, a 4-mL sample was collected for the GTT using another syringe. The VerifyNow test was conducted within 30 minutes from blood sampling, and the GTT was conducted within 20 seconds.
VerifyNow
The VerifyNow is an optical aggregometry that uses light transmission detection to measure platelet aggregation. 20 The aspirin assay uses arachidonic acid as an agonist to enhance platelet aggregation to fibrinogen-coated microbeads in the cartridge. The resulting change in light transmission is known as the aspirin reaction unit (ARU). The P2Y12 assay has a similar mechanism but differs in the type of agonist; it uses adenosine 5′-diphosphate (ADP) and prostaglandin E1 as agonists to enhance platelet aggregation. And the resulting change in light transmission is known as the P2Y12 reaction unit (PRU). 21
Global Thrombosis Test
The GTT uses native and noncoagulated blood and does not require specific agonists during the test. The test tube in the GTT has narrow gaps where the blood can flow, and this high in vitro SS enhances thrombin generation from platelets 22,23 (Supplement Figure 1). As a result of this in vitro SS, a fibrin-stabilized thrombus is formed in the tube. The GTT has a sensor to monitor the time interval between consecutive blood drops from the test tube. The time interval increases as more thrombi are formed. When the time interval increases by more than 15 seconds, the time is recorded as the occlusion time (OT). The “thrombi stabilization period” follows the OT (typical setting: 300 seconds). After this period, the time of the first blood drop, as the result of endogenous thrombolysis, is recorded as the lysis time (LT) (Supplement Figure 1). The validity of the GTT as a monitoring system has been reported in the previous studies. 9,10,23,24 An OT between 300 and 800 seconds reflects an effective antithrombotic activity, and an OT under 300 seconds reveals platelet hyperreactivity. 23 An LT below 3000 seconds reflects regular spontaneous thrombolytic activity, and an LT over 3000 seconds demonstrates a lack of thrombolytic activity. 11
Study End Points and Clinical Follow-Up
The primary purpose of this study was to compare the OT and LT between each group at days 2 and 30 after the initiation of drug administration. We also compared the ARU and PRU at the same time points.
Major adverse cardiac events (MACEs) and bleeding events during follow-up were recorded. Major adverse cardiac event was defined as a composite of cardiac death, myocardial infarction (MI), target lesion revascularization, and ischemic stroke. The cause of death was regarded as cardiovascular unless there was documented evidence of a clear noncardiovascular cause. Myocardial infarction was defined as a troponin I or creatinine kinase myocardial band 3 times the upper limit of the normal range. 25 Target lesion revascularization was considered clinically driven when it was associated with typical symptoms on clinical assessment, typical signs on a stress test, or 70% diameter stenosis on angiographic follow-up. Ischemic stroke was defined as a new focal neurologic deficit of vascular origin lasting at least 24 hours that was proven to be nonhemorrhagic by either computed tomography or magnetic resonance imaging scanning. 18
Safety assessments, including the occurrence of any bleeding complications, were evaluated during follow-up according to the Bleeding Academic Research Consortium criteria. 26
Statistical Analysis
Continuous variables are expressed as means and standard deviation. Group differences in the mean values and proportions of variables were evaluated in one-way analyses of variance (ANOVAs), with post hoc testing using the Bonferroni method. Pearson correlation analysis was used to investigate the relationships between the PRU and the OT and LT. A P value < .05 was considered statistically significant.
In the previous study, mean and standard deviation of OT were 428 and 155, respectively. 11 We anticipated differences in OT as 128. Sample size was 23 for each group whose means are to be compared in a one-way ANOVA study. The total sample of 69 patients achieves 81% power to detect differences among the means,in contrast to the alternative of using equal means, using an F test with a .05 significance level. The size of the variation in the means is represented by their standard deviation, which is 60.34. The common standard deviation within a group is assumed to be 155.0. Final sample size was estimated to be 25 per each group after assuming a 10% of dropout rate. Statistical analyses were performed using SPSS version 25.0 (IBM Co, Armonk, New York) and PASS Software (NCSS, LLC, Kaysville, Utah).
Results
Three out of 81 patients withdrew consent during the follow-up period. Another 3 patients could not finish the study medications due to minor bleeding complications, such as blood-tinged sputum and oral cavity bleeding. Finally, 1-month follow-up data were obtained in a total of 75 patients.
The patients were divided according to their antithrombotic medications into TICA (n = 25, aspirin/ticagrelor), RIVA (n = 25, aspirin/rivaroxaban/CLP), and CLP groups (n = 25, aspirin/CLP; Figure 1). There were no significant differences in drug compliance among the groups (TICA, n = 24 [96%] vs RIVA, n = 23 [92%] vs CLP, n = 25 [100%], P = .353).
Baseline Characteristics
The prevalence of MI (P = .015) and pre-PCI Thrombolysis in Myocardial Infarction flow (P = .012) significantly differed among the 3 groups. Additionally, the groups significantly differed with regard to the white blood cell count (TICA, 9.8 ± 3.0 vs RIVA, 9.6 ± 3.7 vs CLP, 7.3 ± 2.3, P = .007) and serum triglyceride levels (132.7 ± 48.3 vs 173.5 ± 102.4 vs 116.4 ± 69.0, respectively, P = .031). No other baseline characteristics, including anthropometric findings, underlying diseases, laboratory data, and angiographic findings, significantly differed among the 3 groups (Tables 1 and 2).
Baseline Clinical Characteristics.
Abbreviations: CKD, chronic kidney disease; CK-MB, creatine kinase myocardial band; CLP, aspirin/clopidogrel; CVA, cerebrovascular accident; HDL, high-density lipoprotein; INR, international normalized ratio; LDL, low-density lipoprotein; NSTEMI, non-ST-segment elevation myocardial infarction; PT, prothrombin time; RIVA, aspirin/clopidogrel/very low-dose rivaroxaban; STEMI, ST-segment elevation myocardial infarction; TICA, aspirin/ticagrelor; WBC, white blood cell.
Baseline Angiographic Characteristics.

Abbreviations: CLP, aspirin/clopidogrel; LAD, left anterior descending artery; LCX, left circumflex artery; PCI, percutaneous coronary intervention; RCA, right coronary artery; RIVA, aspirin/clopidogrel/very low-dose rivaroxaban; TICA, aspirin/ticagrelor; TIMI, Thrombolysis in Myocardial Infarction.
Clinical Outcomes
No MACEs occurred in any group during follow-up and there were no group differences in the incidence of major or minor bleeding complications (TICA, 1 [4.0%] vs RIVA, 1 [4.0%] vs CLP, 0 [0.0%], P = .598). However, the decrease in hemoglobin levels during follow-up significantly differed among the groups (TICA, −0.3 ± 0.9 g/dL vs RIVA, −0.6 ± 0.7g/dL vs CLP, −0.1 ± 0.4g/dL, P = .037).
Differences in Antiplatelet Activities
The ARU did not differ among the groups at day 2 (TICA, 488.8± 77.7 vs RIVA, 461.1 ± 74.7 vs CLP, 451.6 ± 77.2, P = .227) and at day 30 (447.2 ± 87.1 vs 458.5 ± 70.3, vs 471.9 ± 90.7, respectively, P = .577). However, there was a significant difference in the PRU among the 3 groups at day 2 (TICA, 33.7 ± 59.1 vs RIVA, 138.9 ± 66.6 vs CLP, 162.6 ± 65.4, P < .001) and at day 30 (43.6 ± 57.1 vs 159.9 ± 64.3 vs 188.7 ± 44.1, respectively, P < .001; Figure 2). Post hoc analyses revealed that the PRU was significantly lower in the TICA group than in the RIVA and CLP groups at both day 2 (TICA vs RIVA, P < .001, RIVA vs CLP, P = .581, TICA vs CLP, P < .001) and day 30 (P < .001, P = .216, P < .001, respectively).

Results of the VerifyNow test on day 2 (A) and day 30 (B). ARU indicates aspirin reaction unit; CLP, aspirin/clopidogrel; PRU, P2Y12 reaction unit; RIVA, aspirin/clopidogrel/very low-dose rivaroxaban; TICA, aspirin/ticagrelor.
Differences in Global Thrombotic and Thrombolytic Activities
The OT at day 2 (TICA, 491.5 ± 86.1 vs RIVA, 534.2 ± 100.9 vs CLP, 522.8 ± 68.1, P = .199) and at day 30 (542.1 ± 98.1 vs 598.5 ± 118.0 vs 577.6 ± 85.9, respectively, P = .146) did not significantly differ among the 3 groups. Similarly, the LT at day 2 (TICA, 1663.6 ± 755.5 vs RIVA, 1700.3 ± 482.1 vs CLP, 1515.1 ± 329.9, P = .457) and at day 30 (1522.3 ± 426.5 vs 1734.6 ± 454.3 vs 1510.2 ± 593.9, respectively, P = .207) did not significantly differ among the 3 groups (Figure 3). The number of patients with an LT over 3000 seconds was not significantly different among the 3 groups at day 2 (TICA, 2 [8.0%] vs RIVA, 0 [0.0%] vs CLP, 0 [0.0%], P = .128) and at day 30 (1 [4.0%] vs1 [4.0%] vs 1 [4.0%], P = 1.000).
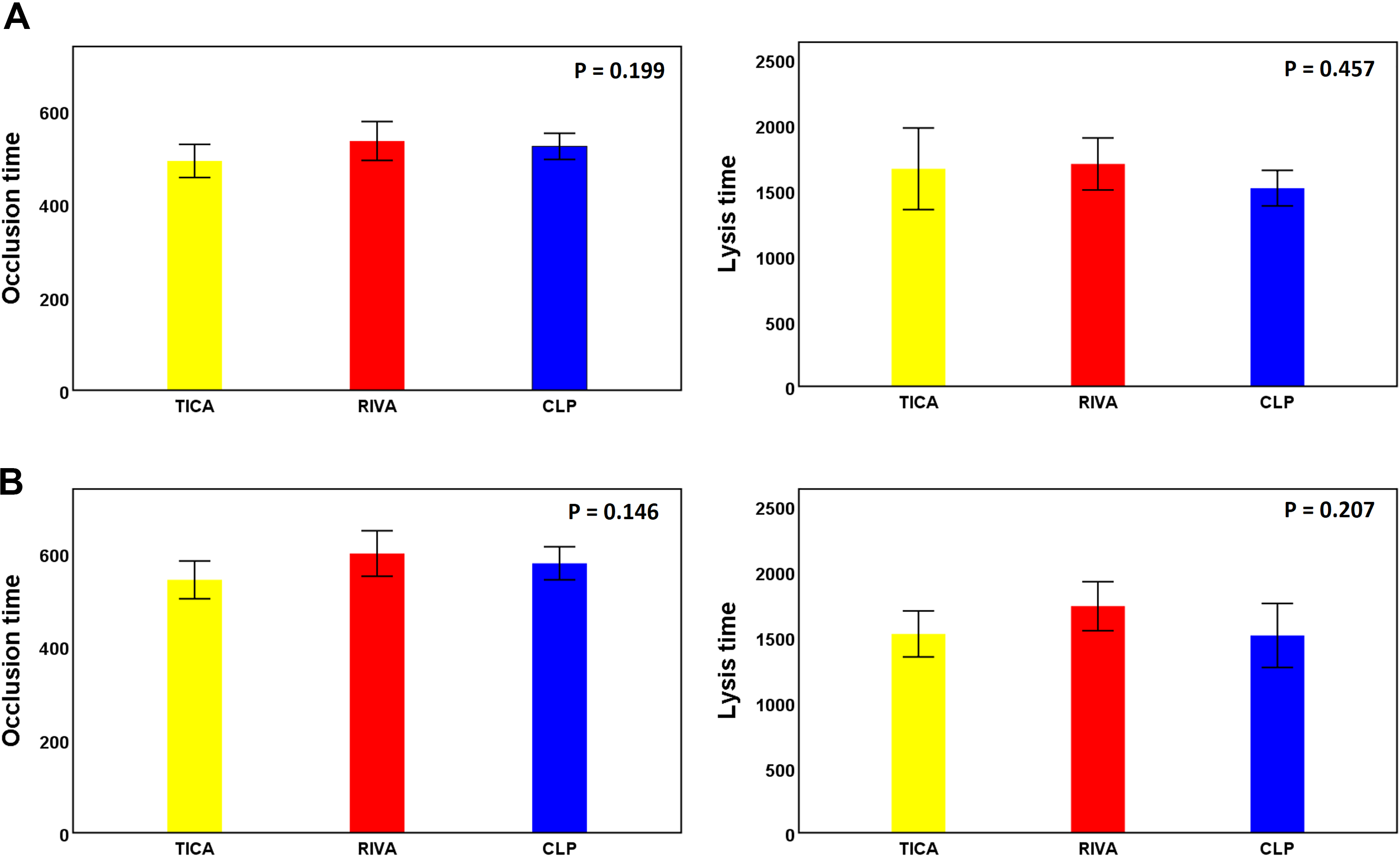
Results of the global thrombosis test on day 2 (A) and day 30 (B). CLP indicates aspirin/clopidogrel; RIVA, aspirin/clopidogrel/very low-dose rivaroxaban; TICA, aspirin/ticagrelor.
Differences in Antiplatelet Activities and Global Thrombotic and Thrombolytic Activities According to ACS Subtype
A subgroup analysis was performed according to ACS subtype (ST-segment elevation myocardial infarction [STEMI], non-ST-segment elevation myocardial infarction [NSTEMI], and unstable angina). Within each ACS subtype, the ARU, OT, and LT did not significantly differ among the 3 treatment regimens; however, the PRU still significantly differed among the 3 treatment regimens (Supplemental Figure 2).
Correlation Between the PRU and OT or LT
The PRU and OT were not significantly correlated at day 2 (r = 0.067, P = .566) and day 30 (r = 0.025, P = .831). Similarly, the PRU and LT were not significantly correlated at day 2 (r = 0.038, P = .744) and day 30 (r = 0.114, P = .331; Figure 4).

Correlations between the PRU and the occlusion analysis times. A, Day 2. B, Day 30. PRU indicates P2Y12 reaction unit.
Discussion
The main finding of the present study was that the global thrombotic and thrombolytic activities under in vitro SS conditions were not different among ticagrelor, very-low-dose rivaroxaban with CLP, and CLP treatment groups, despite a significant difference in the on-treatment ADP-induced platelet activity.
VerifyNow is one of the most commonly used platelet function tests, and its measurement values are associated with clinical outcomes. 27 However, VerifyNow uses citrate-anticoagulated blood. In citrated blood, thrombin is not generated by activated platelets. Therefore, in response to activation, only platelet aggregates, not fibrin-stabilized thrombi, are formed. Also, the VerifyNow test necessitates the separate use of various platelet agonists; the assessment of the actual overall thrombotic status from these different measurements can be difficult.
The GTT has some merits over conventional platelet function tests, such as the VerifyNow test. First, the GTT uses nonanticoagulated blood leaving the plasma calcium ion concentration within physiological levels. Second, the GTT is simple, and its mechanism is relevant to the pathology of ACS, as the initial activating stimulus is high SS. 11 Third, the endogenous thrombolytic activity can be measured using the GTT. As VerifyNow measures the platelet function by mixing agonists with stable blood, it can hardly reflect the actual conditions of ACS. The GTT applies in vitro SS conditions, without any additives, and can indicate actual thrombosis and endogenous fibrinolysis. Therefore, we hypothesized that the GTT would be complementary to the VerifyNow test in comparing antithrombotic strategies.
In the present study, patients administered ticagrelor showed much lower on-treatment ADP-induced platelet reactivity compared to that in the patients administered rivaroxaban plus CLP or only CLP (in addition to aspirin). However, there were no significant differences in the OT among the 3 groups on days 2 and 30. Additionally, there were no correlations between the PRU and the OT and LT. These results suggest that the prescription of a potent antiplatelet agent or the addition of an anticoagulant on top of CLP may not be useful for preventing SS-induced thrombi formation, which is one of the main mechanisms of ACS. 6,28 These findings are consistent with recent studies that failed to prove the benefit of ticagrelor compared to CLP in recent studies, 14,29,30 and they can be a clue to explain why ticagrelor was unable to verify better outcomes than CLP that in vitro SS-induced antithrombotic and lytic activities did not significantly differ among the regimens. The finding of the present study suggests that enhancing antithrombotic potency cannot always be beneficial to every patient with ACS.
The LT reflects the endogenous thrombolytic activity. Impaired endogenous thrombolysis in patients with ACS, defined as an LT ≥3000 seconds, is associated with cardiovascular death and nonfatal MI. 11 Recently, Gorog et al reported that impaired endogenous fibrinolytic activity is associated with recurrent cardiovascular event risk in patients with STEMI and that endogenous fibrinolysis assessment could identify patients with STEMI who remain at a very high risk of cardiovascular events. 13 In the present study, the LT did not significantly differ among antithrombotic strategies at both time points. Previous studies suggested that protease-activated receptor 1 inhibitor, cangrelor, or apixaban may enhance endogenous thrombolysis. 31,32 However, these studies were performed in patients with different conditions, such as stable angina or atrial fibrillation. Further studies will be needed to assess whether impaired endogenous fibrinolysis is a modifiable risk factor and targetable by pharmacotherapy in patients with ACS. Additionally, future research should focus on the variability of endogenous thrombolytic activity in patients with a high risk of cardiovascular events.
Study Limitations
The present study has several limitations. First, this was a nonrandomized study, and there were differences among the 3 treatment groups in terms of the ACS subtype and coronary flow before PCI. Although we cannot rule out potential biases, we were able to confirm similar findings in each ACS subgroup (STEMI, NSTEMI, and unstable angina). Second, this study was planned as a pilot study. Therefore, the sample size was small, and we could not compare clinical outcomes among groups with adequate statistical power. Third, we only used the GTT and VerifyNow; thus, the present results cannot be extrapolated to other assays.
Conclusion
Shear stress–induced global thrombotic and lytic activities did not differ among patients treated with ticagrelor, very-low-dose rivaroxaban plus CLP, or CLP, despite marked differences in ADP-induced platelet aggregation.
Supplemental Material
Supplemental_Figure_Legends - Comparison of Shear Stress–Induced Thrombotic and Thrombolytic Effects Among 3 Different Antithrombotic Regimens in Patients With Acute Coronary Syndrome
Supplemental_Figure_Legends for Comparison of Shear Stress–Induced Thrombotic and Thrombolytic Effects Among 3 Different Antithrombotic Regimens in Patients With Acute Coronary Syndrome by Minsuk Kim, Si-Hyuck Kang, Jeong-Ran Kim, Jin Joo Park, Young-seok Cho, Tae-Jin Youn, In-Ho Chae and Jung-Won Suh in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
Supplement_figure_1 - Comparison of Shear Stress–Induced Thrombotic and Thrombolytic Effects Among 3 Different Antithrombotic Regimens in Patients With Acute Coronary Syndrome
Supplement_figure_1 for Comparison of Shear Stress–Induced Thrombotic and Thrombolytic Effects Among 3 Different Antithrombotic Regimens in Patients With Acute Coronary Syndrome by Minsuk Kim, Si-Hyuck Kang, Jeong-Ran Kim, Jin Joo Park, Young-seok Cho, Tae-Jin Youn, In-Ho Chae and Jung-Won Suh in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
Supplement_figure_2-A1 - Comparison of Shear Stress–Induced Thrombotic and Thrombolytic Effects Among 3 Different Antithrombotic Regimens in Patients With Acute Coronary Syndrome
Supplement_figure_2-A1 for Comparison of Shear Stress–Induced Thrombotic and Thrombolytic Effects Among 3 Different Antithrombotic Regimens in Patients With Acute Coronary Syndrome by Minsuk Kim, Si-Hyuck Kang, Jeong-Ran Kim, Jin Joo Park, Young-seok Cho, Tae-Jin Youn, In-Ho Chae and Jung-Won Suh in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
Supplement_figure_2-A2 - Comparison of Shear Stress–Induced Thrombotic and Thrombolytic Effects Among 3 Different Antithrombotic Regimens in Patients With Acute Coronary Syndrome
Supplement_figure_2-A2 for Comparison of Shear Stress–Induced Thrombotic and Thrombolytic Effects Among 3 Different Antithrombotic Regimens in Patients With Acute Coronary Syndrome by Minsuk Kim, Si-Hyuck Kang, Jeong-Ran Kim, Jin Joo Park, Young-seok Cho, Tae-Jin Youn, In-Ho Chae and Jung-Won Suh in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
Supplement_figure_2-B1 - Comparison of Shear Stress–Induced Thrombotic and Thrombolytic Effects Among 3 Different Antithrombotic Regimens in Patients With Acute Coronary Syndrome
Supplement_figure_2-B1 for Comparison of Shear Stress–Induced Thrombotic and Thrombolytic Effects Among 3 Different Antithrombotic Regimens in Patients With Acute Coronary Syndrome by Minsuk Kim, Si-Hyuck Kang, Jeong-Ran Kim, Jin Joo Park, Young-seok Cho, Tae-Jin Youn, In-Ho Chae and Jung-Won Suh in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
Supplement_figure_2-B2 - Comparison of Shear Stress–Induced Thrombotic and Thrombolytic Effects Among 3 Different Antithrombotic Regimens in Patients With Acute Coronary Syndrome
Supplement_figure_2-B2 for Comparison of Shear Stress–Induced Thrombotic and Thrombolytic Effects Among 3 Different Antithrombotic Regimens in Patients With Acute Coronary Syndrome by Minsuk Kim, Si-Hyuck Kang, Jeong-Ran Kim, Jin Joo Park, Young-seok Cho, Tae-Jin Youn, In-Ho Chae and Jung-Won Suh in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
Supplement_figure_2-C1 - Comparison of Shear Stress–Induced Thrombotic and Thrombolytic Effects Among 3 Different Antithrombotic Regimens in Patients With Acute Coronary Syndrome
Supplement_figure_2-C1 for Comparison of Shear Stress–Induced Thrombotic and Thrombolytic Effects Among 3 Different Antithrombotic Regimens in Patients With Acute Coronary Syndrome by Minsuk Kim, Si-Hyuck Kang, Jeong-Ran Kim, Jin Joo Park, Young-seok Cho, Tae-Jin Youn, In-Ho Chae and Jung-Won Suh in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
Supplement_figure_2-C2 - Comparison of Shear Stress–Induced Thrombotic and Thrombolytic Effects Among 3 Different Antithrombotic Regimens in Patients With Acute Coronary Syndrome
Supplement_figure_2-C2 for Comparison of Shear Stress–Induced Thrombotic and Thrombolytic Effects Among 3 Different Antithrombotic Regimens in Patients With Acute Coronary Syndrome by Minsuk Kim, Si-Hyuck Kang, Jeong-Ran Kim, Jin Joo Park, Young-seok Cho, Tae-Jin Youn, In-Ho Chae and Jung-Won Suh in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Authors’ Note
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the Seoul National University Bundang Hospital Research Fund (02-2013-077) and a grant from Yuhan Pharmaceutical Co, Ltd (Seoul, Korea). The sponsors of the study had no role in the design and conduct of the study, including the collection, management, analysis, and interpretation of the data, and the preparation, review, and approval of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.