
Abstract
Despite the development of new oral agents over the last decade, vitamin K antagonists (VKAs) remain the most widely used anticoagulants for treating and preventing thromboembolism worldwide. In Chile, the Ministry of Health indicates that acenocoumarol should be used in preference to any other coumarin. Complications of inappropriate dosing are among the most frequently reported adverse events associated with this medication. It is well known that polymorphisms in pharmacokinetic and pharmacodynamic proteins related to coumarins (especially warfarin) influence response to these drugs. This work analyzed the impact of CYP2C19*2 (rs4244285), CYP1A2*1F (rs762551), GGCx (rs11676382), CYP2C9*2 (rs1799853), CYP2C9*3 (rs1057910), CYP4F2 (rs2108622), VKORC1 (rs9923231), VKORC1 (rs7294), CYP3A4*1B (rs2740574), and ABCB1 (rs1045642) polymorphisms on time to therapeutic range for oral anticoagulants in 304 Chilean patients. CYP2C9*3 polymorphisms were associated with time to therapeutic range for acenocoumarol in Chilean patients, and the CYP4F2 TT genotype, MDR1 A allele, CYP1A2 A allele, and CYP3A4T allele are promising variants that merit further analysis. The presence of polymorphisms explained only 4.1% of time to therapeutic range for acenocoumarol in a multivariate linear model. These results improve our understanding of the basis of ethnic variations in drug metabolism and response to oral anticoagulant therapy. We hope that these findings will contribute to developing an algorithm for VKA dose adjustment in the Chilean population in the near future, decreasing the frequency of stroke, systemic embolism, and bleeding-related adverse events.
Introduction
Cardiovascular disease (CVD), the leading cause of death worldwide, includes a group of disorders of the heart and blood vessels, such as hypertension, coronary heart disease and myocardial infarction, cerebrovascular disease and stroke, peripheral vascular disease, heart failure, rheumatic heart disease, congenital heart disease, and various cardiomyopathies. An estimated 17.9 million people die from CVD each year, 85% due to heart attack or stroke, 1 and deaths are projected to reach 23.6 million per year by 2030. Most CVD can be prevented by addressing behavioral risk factors (such as tobacco use, diet, physical activity, and alcohol abuse). 1,2 In Chile, CVD (ICD-10 I00-I99) accounted for 27.6% of total mortality in 2016, representing 28 148 deaths, at a rate of 154.73 per 100 000 inhabitants (158.69 and 150.85 in males and females, respectively). These deaths were mainly due to stroke (8603 deaths, 48.28/100 000 inhabitants) and acute myocardial infarction (8102 deaths, 45.47/100 000 inhabitants). 3 The pathophysiology of CVD is partly based on failure of the hemostatic response. Activation of factors II, VII, IX, and X in this coagulation cascade depends on the vitamin K cycle, which consists of 2 enzymes, vitamin K epoxide reductase C1 (VKORC1), responsible for metabolizing vitamin K epoxide to its reduced form (hydroquinone), and reduced vitamin K, a cofactor of the enzyme gamma-glutamyl carboxylase (GGCx), whose function is to activate coagulation factors II, VII, IX, and X through posttranslational modification, carboxylating glutamyl residues to gamma-carboxyglutamic acid residues on these factors and generating vitamin K epoxide. In parallel, the CYP4F2 isoenzyme metabolizes reduced vitamin K for excretion through the urine, thereby decreasing the reduced vitamin K available in the cycle. 4 Vitamin K antagonists (VKAs) or coumarin (acenocoumarol and warfarin) drugs competitively inhibit VKORC1 due to their structural similarity to vitamin K epoxide, preventing its binding to the active site. This inhibition decreases reduced vitamin K production and consequently lowers active II, VII, IX, and X factors levels, effectively inhibiting the coagulation cascade. 5,6 Vitamin K antagonists are administered in weekly doses and adjusted based on the patient’s international normalized ratio (INR) values, which are measured at each visit. The target anticoagulation level for a given patient, expressed as an INR range, depends on the pathology for which anticoagulation was indicated. 7,8 It may take 6 months or longer to achieve a stable therapeutic range, defined as 3 consecutive visits with a therapeutic INR value at the same dose. 9,10
Vitamin K antagonists have a narrow therapeutic margin, and there are many variables that influence their efficacy, such as consumption of green leafy vegetables (which are high in vitamin K), use of CYP2C9-agonist/antagonist drugs, and genetic factors. 11 Complications of inappropriate dosing of coumarin drugs, particularly warfarin, are among the adverse events most frequently reported to the US Food and Drug Administration and one of the most common reasons for emergency consultations associated with such medications. 12 Bleeding is the most common complication of antithrombotic therapy and predicts future cardiovascular events. Although the mechanisms that link acute hemorrhage with these later episodes are not well understood, bleeding prevention can be expected to decrease related morbidity and mortality. 13 These complications might be decreased with a lower time to therapeutic range (TtTR) through proper adjustment of coumarin therapy.
Pharmacogenetic studies have assessed the relationship between genetic factors and required coumarin or VKA dose. The most studied polymorphisms include CYP2C9*2 (rs1799853), CYP2C9*3 (rs1057910), CYP4F2 (rs2108622), vitamin K epoxide reductase complex subunit 1 (VKORC1, rs9923231 and rs7294), gamma-glutamyl carboxylase (GGCx rs11676382), and P-glycoprotein (P-gp), the product of multidrug resistance gene 1 (MDR1, ABCB1 rs1045642), which plays a key role in metabolism of oral anticoagulants. 14 –18 Polymorphisms in enzymes VKORC1, GGCX, CYP2C9, CYP4F2, CYP3A4, CYP1A2, CYP2C19, and MDR1 affect response to a given VKA dose in patients treated with oral anticoagulants. 19,20 Thus, the main objective of this study was to determine the frequencies of these genetic polymorphisms in a representative group of Chilean patients and their relationship with time to therapeutic dose of VKA. These findings could be useful in developing a pharmacogenomic algorithm for coumarin medications in the Chilean population.
Methods
Study Design and Sample Size
This retrospective study assessed patients treated with the VKA acenocoumarol as an antithrombotic at the Western Metropolitan Health Service in the Santiago and Melipilla provinces of Chile. International normalized ratio measurements were performed with a capillary sample using CoaguChek pro II equipment (Roche Mannheim, Germany). The sample size was determined according to the frequency of variant allele carriers in the population under study, using PS Power and Sample Size Calculations Version 3.0, 2009.
Patients
Blood samples were obtained from 279 patients aged 18 years or older. The study was approved by the Western Metropolitan Health Service Ethics Committee (protocol 027/2016), and all study activities were performed in compliance with in the Declaration of Helsinki (Declaration of Helsinki, 1964), Chilean laws 20.120, 20.584, and 19.628, and the Good Clinical Practices guidelines. All participants signed a written consent form. Recruitment was performed from June 2016 until December 2017. Table 1 shows the general characteristics of the study population.
Baseline Characteristics of Patients.a

Abbreviations: INR, international normalized ratio; SD, standard deviation.
a n = 279.
b Time to therapeutic range (INR, 2.0-3.0).
Data Collection and Calculation of TtTR
Patient data were obtained from clinical centers and managed with the statistical module of the anticoagulant treatment dosing software TAONet (Roche Diagnostics, Mannheim, Germany). Patient-level TtTR was estimated by assigning in-range INR values to each day between 3 consecutive in-range readings by linear interpolation, as described by Rosendaal et al. 21
Genotyping
Potentially functional single-nucleotide polymorphisms (SNP) encoding the proteins related to coumarin response were obtained from the NCBI dbSNP database (https://www.ncbi.nlm.nih.gov/snp) and SNPinfo Web Server (https://snpinfo.niehs.nih.gov) based on the level of evidence for each SNP. Genomic DNA was isolated from peripheral blood samples from patients using the High Pure PCR Template Preparation Kit (Catalog Number, 11796828001; Roche Diagnostics GmbH, Mannheim, Germany). CYP2C19*2 (rs4244285), CYP1A2*1F (rs762551), GGCx (rs11676382), CYP2C9*2 (rs1799853), CYP2C9*3 (rs1057910), CYP4F2 (rs2108622), VKORC1 (rs9923231), VKORC1 (rs7294), CYP3A4*1B (rs2740574), and ABCB1 (rs1045642) were analyzed using the TaqMan SNP Genotyping Assay (catalog number 4362691; Thermo Fisher Scientific, Waltham, Massachusetts) in a Stratagene Mx3000p real-time PCR system (Agilent Technologies, Santa Clara, California). For quality assurance, we repeated the analysis on a randomly selected 20% of samples. The context sequences for the TaqMan probes and descriptions of each polymorphism are shown in Table 2.
Context Sequences for TaqMan Probes, Used in This Study.a
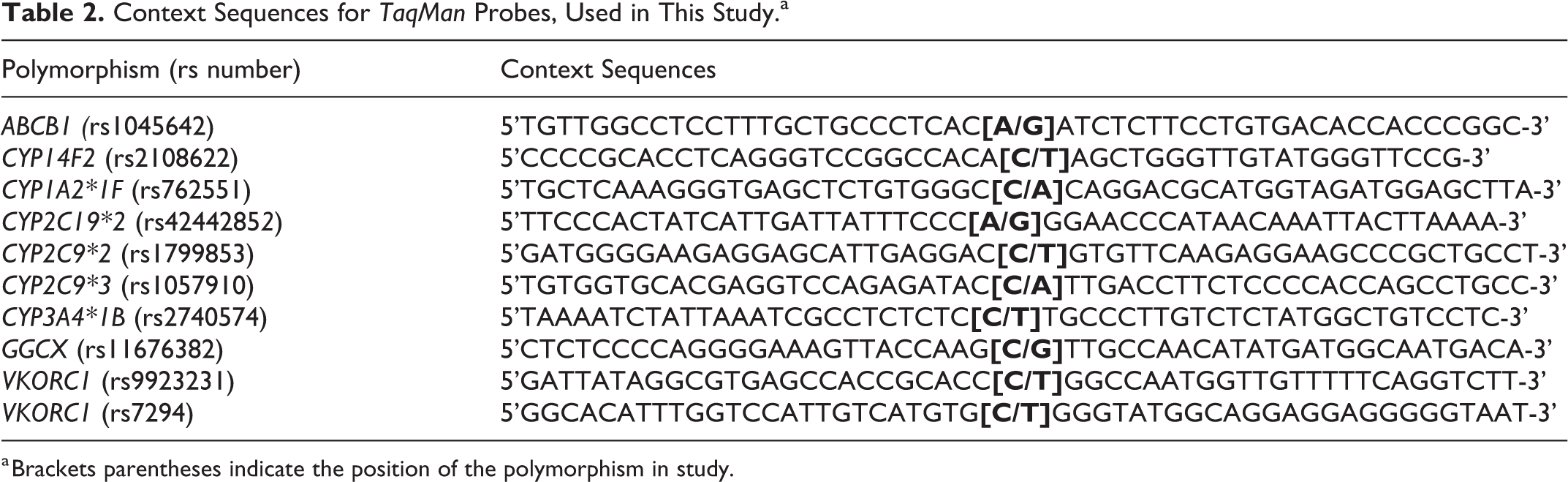
a Brackets parentheses indicate the position of the polymorphism in study.
Statistical Analyses
We performed a Mann-Whitney U analysis to evaluate TtTR by genotype. We then developed a multivariate linear regression model using variables with a value P ≤ .2 (cutoff) in the univariate analysis to adjust the R2. All comparative studies were assayed by testing 3 genetic models of inheritance (dominant, codominant, and recessive), choosing the parameters with the optimal statistical association for each analysis. We used Stata software, version 12.0 (StataCorp LP, College Station, Texas) for all tests. A P value of ≤.05 was considered statistically significant. We did not evaluate for Hardy-Weinberg equilibrium (HWE) as our sample does not meet basic conditions for HWE. The patients do not represent a random sample from a random mating population, a control group, or the general population 22 ; rather, the group was selected for disease. This point is significant as the SNP under study may also be related to susceptibility to cardiovascular disorders.
Results
Demographic characteristics are shown in Table 1. A total of 279 Chilean patients (66.49 ± 14.11 years old, 54.5% men, 45.5% women) were included and analyzed. Patients were ethnically representative of the Chilean population, which is predominantly Caucasian or Amerindian Caucasian (8.72%). 23 Table 1 also provides the TtTR along with the median and interquartile range. The genotype and allele frequencies for the 10 polymorphisms analyzed are shown in Table 3.
Genotype and Allele Frequencies in Patients.a

a n = 279.
Table 4 shows the comparative analysis for TtTR by genotype. As described earlier, the relationship between the 10 SNP and TtTR was assessed using 3 different inheritance models, namely, codominant, where each genotype is assumed to have a different and nonadditive comparative risk; dominant, where a single copy of the SNP is assumed to be sufficient to modify the risk; and recessive, where 2 copies are assumed to be necessary to modify risk. 24 Only the CYP2C9*3 (rs1057910) A allele was found to be statistically associated with higher TtTR, in the codominant (P = .026) and dominant models (P = .014). However, the CYP4F2 TT genotype, MDR1 A allele, and CYP3A4 T allele showed promising associations that merit further study (P = .069, P = .066, and P = .078, respectively).
Relationship of the Genotypes in Study and the Days that Elapsed to Achieve a Dose Adjusted.a

Abbreviations: INR, international normalized ratio; NA, not applicable; ND, no data available; Ref., reference.
a N = 279.
b Therapeutic range = INR 2.0-3.0.
c IQR: Interquartile range.
d P < .05 is considered as statistically significant.
After a forward stepwise procedure, using P < .2 as the cutoff, a multivariate linear regression analysis was performed. Table 5 shows results of this analysis, which included the MDR1 (rs1045642), CYP4F2 (rs2108622), CYP3A4*1B (rs2740574), CYP1A2*1F (rs762551), and CYP2C9*3 (rs1057910) variant alleles. The model explained only 4.12% of the variation in TtTR (adjusted R2) in the population studied.
Multivariate Linear Regression Analysis Between the Time to Reach the Therapeutic Range and Genetic Polymorphisms.

Abbreviation: CI, confidence interval.
a P < .05 is considered as statistically significant.
Discussion
The indicator most often used to evaluate the efficacy of oral anticoagulant treatment is time in therapeutic range (TTR). 25 A study on the prognostic role of TTR in patients treated with coumarins indicated that rates of stroke, systemic embolism, and bleeding were significantly lower in patients with a TTR above 65%, which also translated to lower mortality. 26 The National Institute for Health and Care Excellence recommends a TTR above 65%, and the European Society of Cardiology recommends a target of at least 70% for optimal anticoagulation control with VKA drugs. 27,28 In Chile, few studies have characterized patients treated with coumarin derivatives. However, the GARFIELD-AF study, which assessed Chilean patients with atrial fibrillation, reported in 2017 that the median TTR was 40% for 971 patients treated in several public hospitals and private clinics. 29 In a previous work, we reported that acenocoumarol is the most widely used anticoagulant in Chile (representing 87.8% of anticoagulant prescriptions) and that the median TTR was 50% for patients being treated with oral anticoagulants in the Western Metropolitan Health Service network. 10 These 2 TTR values fall below standards for adequate anticoagulation control.
In this study, we examined whether genetic polymorphisms might influence TtTR in Chilean patients treated with acenocoumarol, as starting dosage might be defined more accurately using pharmacogenetics tools. It is well known that patients whose initial dosage is based on a genotype-guided algorithm require less time to reach the therapeutic range and spend more time within range than patients who receive a standard dose without this tool. 30
The general characteristics of the study sample (Table 1) reflect an overweight adult population (body mass index =29.32 ± 5.77), which is consistent with the results of the Chilean National Health Survey 2017. According to that survey, 41.2% of Chilean people in the age range of the patients in this study were overweight, and 34.5% were obese. 31 Overweight and obesity are important risk factors for cardiovascular disease. Strikingly, TtTR varied from 30 to 2531 days, with an average of 335 and median of 229 days. Patients are at high risk of stroke or hemorrhage during this time. This wide range of TtTR may explain the lack of significance of some variants in the comparative statistical analysis shown in Table 4. However, several interesting observations can be highlighted. The CYP2C9*3 (rs1057910) A allele is significantly associated with higher TtTR in the codominant (P = .026) and dominant models (P = .014), demonstrating a crucial role of this enzyme in acenocoumarol metabolism. Furthermore, there is a clear tendency toward a longer TtTR among patients carrying the CYP4F2 TT genotype, MDR1 A allele, CYP1A2 AA genotype, and CYP3A4 T allele, suggesting that these variants may also have a role in TtTR for this drug. Of course, larger and better controlled retrospective studies will be needed to corroborate this finding. Conversely, the VKORC1 rs7294 and rs9923231, CYP2C9*2 (rs1799853), CYP1A2*1F (rs762551), CYP2C19*2 (rs4244285), and GGCx (rs11676382) variant alleles do not seem to correlate with TtTR, suggesting that these polymorphisms do not affect the time needed to reach a therapeutic dose (INR = 2.0-3.0). In some cases, the low number of patients carrying the genotype (eg, GGCx rs11676382 GG and CYP2C9 TT) or haplotype (CYP2C9*2/*3) did not allow for statistical association analyses (data not shown).
To analyze interactions among genotypes and TtTR, we performed a multivariate linear regression using a forward stepwise procedure based on the results from the univariate linear regression analysis, as suggested in the biostatistical literature. 32 Table 5 shows that a multivariate model including MDR1 (rs1045642), CYP4F2 (rs2108622), CYP3A4*1B (rs2740574), CYP1A2*1F (rs762551), and CYP2C9*3 (rs1057910) variant alleles explained only 4.12% of the variation in TtTR (adjusted R2) in the population studied. This is a low level of explanation, but we were not able to find any other study worldwide to which we might compare this result. This model seems to be the first reported for TtTR and VKA-related pharmacokinetic/pharmacodynamic genetic polymorphisms.
In addition, it is well known that ethnicity plays an important role in the pharmacokinetics and pharmacodynamics of drugs, 32 –36 and it might be assumed that the situation is even more complex in “mestizo” groups such as South American populations. As a first step, we compared the allele frequencies for the polymorphisms analyzed in our study population with those reported in international studies on patients treated with anticoagulants (Table 6). We did not find any data for CYP1A2*1F (rs762551), CYP2C19*2 (rs4244285), CYP3A4*1B (rs2740574), or GGCx (rs11676382) in patients treated with VKA. Interestingly, however, the allele frequencies for VKORC1 rs9923231 and CYP2C9*2 (rs1799853) in our investigation were similar to values from studies performed in Puerto Rico and Colombia, suggesting similarities among patients from these Latin American regions. In contrast, there are apparent differences between the allele frequencies found here and those reported for an African American population, likely attributable to the differences in ethnic background between the 2 study groups. The Chilean population is largely a mixture of Native Americans and Caucasians (mostly Spaniards), and persons of African American descent or “afrochilenos” do not contribute significantly to the admixture, 41 although this situation has changed notably over the last 5 years due to an increase in immigrants of African descent (mainly from Venezuela, Peru, Haiti, and Colombia). 42
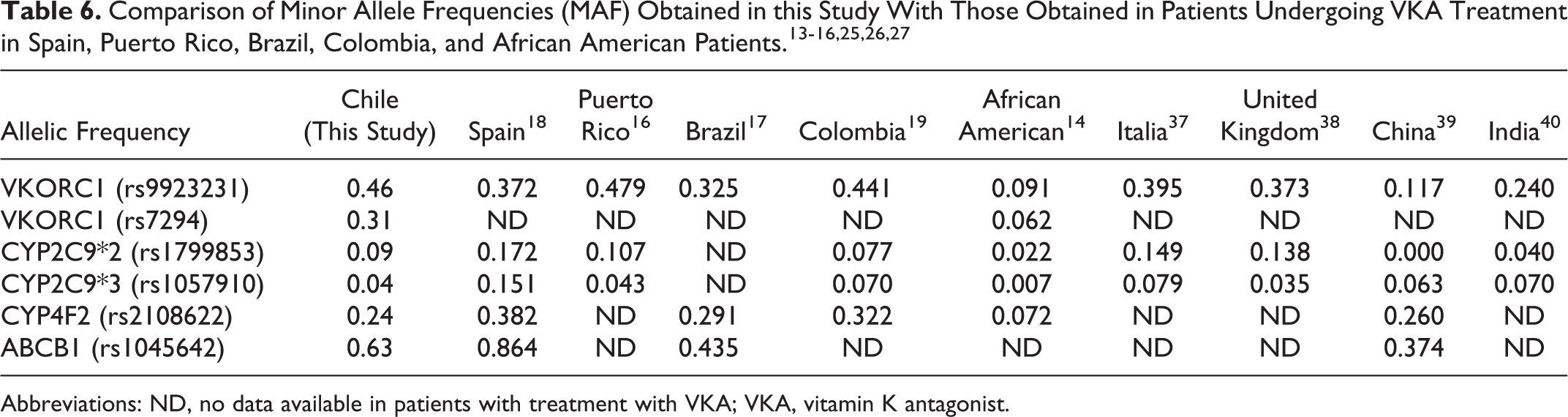
Abbreviations: ND, no data available in patients with treatment with VKA; VKA, vitamin K antagonist.
This study has some limitations. Although we had a relatively appropriate sample size, the small number of patients could mask associations, especially for polymorphisms with a low minor allele frequency in this population (CYP2C9*2, CYP2C9*3, and GGCx rs1167638). Furthermore, Chile has not yet developed official standards for anticoagulant therapy (although these guidelines are in progress). Therefore, the starting dose is empirical, based on clinical criteria. This approach increases the variability of the dosage and concomitantly the variability in TtTR, as dosing depends partly on the clinical center and attending physician. Moreover, some patients eventually drift back out of range after reaching a therapeutic INR (2.0-3.0, three consecutive measurements) due to factors such as use of over-the-counter medications, changes in bowel flora or bowel function due to intercurrent or chronic diseases, and poor compliance with medication and dietary instructions. These factors were not analyzed in this study. Finally, other potentially relevant genes and polymorphisms were not evaluated in this study, such as calumenin (CALU) rs2290228, an Arg4Gln sequence change recently identified as a candidate involved in the pharmacogenetics of acenocoumarol anticoagulant therapy. 41,43.
Conclusion
We found that CYP2C9*3 polymorphisms are associated with TtTR for VKA in Chilean patients and that the CYP4F2 TT genotype, MDR1 A allele, and CYP3A4 T allele are promising variants that merit further analysis. These results advance our understanding of the basis of ethnic variations in drug metabolism and response to oral anticoagulant therapy. We hope that this information on genetic variants that might affect oral anticoagulation treatment will contribute to developing an algorithm for VKA dose adjustment in the Chilean population in the near future. This tool might be used along with INR values to more precisely adjust VKA dosage, thereby improving the quality of anticoagulation therapy as measured through TTR while decreasing the rate of adverse events including stroke, systemic embolism, and bleeding.
Footnotes
Acknowledgments
The authors wish to thank the patients from the Western Metropolitan Health Service (WMHS) in the Santiago and Melipilla provinces for their altruistic collaboration in pursuit of the common welfare. The authors also thank the Latin American Society of Pharmacogenomics and Personalized Medicine (SOLFAGEM) for sponsoring this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partially supported by Roche Diagnostics Chile and CYTED Grant nº 219RT0572.