
Abstract
This study evaluates coagulation profiles of single ventricle (SV) patients in relationship to liver function, hemodynamic variables and outcome. Twenty-six children with SV anatomy were included. Advanced coagulation profiles, invasive preoperative hemodynamic parameters and clinical course were retrospectively analyzed. Median (interquartile range) age and weight at the time of blood sampling was 25.5 (31) months and 10.5 (6.9) kg. Sixteen patients (16/26; 62%) showed decreased antithrombin and/or protein C (PC) and/or free protein S (PS) function and/or free PS antigen. Two patients showed abnormal activated PC resistance ratio due to heterozygous factor V Leiden mutation and 1 heterozygous prothrombin G20210A mutation. Group comparison (abnormal coagulation profile [group 1; n = 16] versus normal coagulation profile [group 2; n = 10]) showed longer postoperative hospitalization time (p = .04), longer postoperative catecholamine support (p = .01), a higher incidence of thromboembolic events (p = .04), and chylothoraxes (p = .007) in group 1. In 5 (31%) of 16 group 1 patients, thromboembolic complications occurred: cerebral stroke (n = 1), intestinal ischemia (n = 2), thrombus formation in inferior caval vein (n = 1), and pulmonary vein (n = 1). Abnormalities in coagulation parameters are common in SV patients. Coagulation abnormalities constitute a preoperative risk factor and affect postoperative course.
Introduction
The Fontan palliation for patients with single ventricle (SV) anatomies was developed in the 1970s. 1 The introduction of appropriate surgical techniques 2 led to a significant improvement in the survival of these patients. 3 Nowadays, a total (extracardiac) cavopulmonary connection is created in most functional univentricular hearts (UVH), where this is felt to be the only option to separate the systemic and pulmonary circulation. 4 However, this palliation has intrinsic limitations 5 and the management of long-term complications is still a major topic in the care of these patients. 6
Thrombotic and thromboembolic events are a widely recognized complication with an estimated prevalence ranging from 7% to 33%, 7 especially during the postoperative management of these patients. The associated mortality can be as high as 25% and a pathologic coagulation profile influences the functional state of Fontan patients. 7 Because of the complexity of the coagulation system and a large number of candidate risk factors, assessing the individual patients’ risk is difficult and the management of the anticoagulation therapy in these patients is still controversial. Therefore, it seems important to find clinically useful markers to identify children at increased risk for thrombotic events.
Several reports 8 –19 have shown a higher prevalence of coagulation factor abnormalities (eg, altered concentrations of protein-C [PC], protein-S [PS], antithrombin [AT], factors II, V, VII, VIII, and X) in this patient population, which may have an important influence on thrombotic events during clinical course. The coagulation imbalance precedes Norwood stage III palliation. 8,10,11 Therefore, the alterations do not seem to be a direct consequence of the anatomic and physiologic changes originating from the Fontan circulation. Hepatic abnormalities resulting from chronic systemic venous hypertension 8,9,13,14,19 and protein losing enteropathy (PLE) 7,20 have been proposed as a plausible cause for abnormal liver protein synthesis. The role of physiologic derangements and endothelial abnormalities originating from chronic cyanosis, 12 low cardiac output, or perhaps even genetic predisposition 21,22 have also been hypothesized.
The relatively high prevalence of thrombotic and thromboembolic complications advocates for a better understanding of the specific impact of the hemodynamic status on the coagulation parameters as well as of the influence of an abnormal coagulation profile on postoperative course. Therefore, this analysis aims for a description of some coagulation parameters in a heterogenous group of SV patients throughout staged palliation. Moreover, we set the target of exploring possible relationships between coagulation parameters and hemodynamic variables, liver enzymes, and some clinical parameters (immediately after surgery and at 6 months of follow-up).
Methods
This is a retrospective, chart review study including patients at the University Children’s Hospital Zurich. Between 2016 and 2018, consecutive patients with univentricular cardiac anatomy undergoing staged Norwood/Fontan palliation (stage I, II or III), who underwent cardiac catheterization and received an advanced assessment of their coagulation profile, were included in this analysis.
At cardiac catheterization, mean pulmonary artery pressure (mPAP), mean right atrial pressure (mRAP), systemic ventricle end-diastolic pressure (EDP), pulmonary capillary wedge pressure (PCWP), arterial oxygen saturation (SaO2), mean transpulmonary pressure gradient (mTPG), pulmonary vascular resistance (Rp, in WU/m2), and ratio of pulmonary-to-systemic vascular resistance (Rp/Rs) were assessed. During introduction of anesthesia, a venous blood sample was taken, and an advanced evaluation of the coagulation profile was performed. Antithrombin, PC, free PS function, free PS antigen, activated PC resistance (APC resistance), prothrombin time (PT), activated partial thromboplastin time (aPTT), Quick test, and fibrinogen were measured. A screening for a heterozygous factor V Leiden mutation and heterozygous prothrombin G20210A mutation was performed. In addition, N-terminal pro-brain natriuretic peptide (NT-pro-BNP) level, liver function parameters and complete blood count were analyzed.
Antithrombin activity was evaluated using a factor Xa-based chromogenic assay, PC activity using a chromogenic assay, and free PS with a PT-based clotting assay and with the antigen concentration of the free form (free PS antigen). The presence of an altered coagulation screening was defined by an abnormal AT and/or PC and/or free PS and/or free PS antigen and/or APC resistance and/or the presence of factor V Leiden and/or heterozygous prothrombin G20210A mutation. The patients with an altered coagulation screening were defined as group 1 and those with a normal coagulation screening as group 2. The reference values for the coagulation parameters according to age were taken from Toulon et al, 23 and for the other chemical parameters, internationally validated references were used. As NT-pro-BNP was markedly skewed, a logarithmic transformation was performed.
The medical history of patients from birth to 6 months after sampling was screened to define cardiac anatomy, baseline characteristics and surgical history. The development of thromboembolic events or extensive bleeding during this time period was analyzed in detail. Other complications (eg, chylothorax, diaphragmatic paralysis, PLE, and plastic bronchitis) were classified as present or absent. To characterize the postsurgical outcome, the need for postoperative cardiac resuscitation (mechanical or pharmaceutical), need of inhaled nitric oxide (iNO), as well as the length of hospital stay, mechanical ventilation and catecholamine support were assessed. At 6-month follow-up survival, the presence of complications and echocardiography parameters were assessed.
Statistical analysis was performed using SPSS 25 (SPSS Inc, IBM Company, Chicago, Illinois). Normally distributed data were presented as mean and standard deviation and data of other distributions as median and interquartile range. Group comparison was performed using 2-sample t test or χ2 test. Levene test for equality of variance was used to test for homogeneity of variance. The ordinal, nominal and dichotomical variables were evaluated with contingency tables and compared with χ2 tests. The predictability of the continuous variables was evaluated by means of Pearson correlations. The significance is defined by values of p < .05. The study was conducted in accordance with the Declaration of Helsinki (revision 2013). The local ethical committee approved the study.
Results
Description of Study Participants
In total, 26 patients were included in the analysis. Baseline characteristics and clinical/surgical outcome of all patients are summarized in Table 1. Hemodynamic parameters obtained at cardiac catheterization are listed in Table 2.
Baseline Characteristics of Study Population: Patients With at Least 1 Abnormality in Their Coagulation Profile (Group 1) and Patients With a Normal Coagulation Profile (Group 2).a

Abbreviations: aPTT, activated partial thromboplastin time; iNO, inhaled nitric oxide; LV, left ventricle; n, sample number; NT-pro-BNP, N-terminal pro-brain natriuretic peptide; PLE, protein losing enteropathy; RV, right ventricle; Tc, Thrombocytes; y, yes.
a Data presented as mean ± SD/median (interquartile range)/n (%). Group comparison was performed using 2-sample t test or χ2 test (significance level P < .05).
b Of systemic-pulmonary artery shunts during stage I palliation, intestinal ischemia or stroke; Percentile of reference values according to age and sex.
Illustration of Hemodynamic Variables at the Time of Cardiac Catheterization of Study Population.a

Abbreviations: mPAP, mean pulmonary artery pressure; mRAP, mean right atrial pressure; mTPG, mean transpulmonary pressure gradient; PCWP, pulmonary capillary wedge pressure; Rp, pulmonary vascular resistance; Rp:Rs, ratio of pulmonary-to-systemic vascular resistance; SV-EDP, single ventricle end-diastolic pressure; SaO2, arterial oxygen saturation.
a Data presented as mean ± standard deviation.
Coagulation Profile, Distribution, and Effects of Coagulation Abnormalities
Complete results of the analysis of the coagulation profiles are shown in Table 3. A total of 16 (62%) patients showed at least 1 abnormality (group 1). Nine (34%) patients had an isolated reduction in PC; 2 (8%) patients reduced PC and AT; 2 (8%) patients a heterozygous prothrombin G20210A mutation; 1 (4%) patient a factor V Leiden heterozygous mutation; 1 (4%) patient an isolated reduction in free-PS; and 1 (4%) patient reduced PC, free-PS, and free-PS-antigen. These patients (group 1) compared to patients with a normal coagulation profile (group 2) showed a longer postoperative hospital stay (21.3 ± 9.5 days vs 14.8 ± 4.5 days; p = .04), longer postoperative catecholamine support (3.5 ± 2.5 days vs 1.3 ± 0.7 days; p = .01), a higher incidence of chylothoraxes (p = .007), and a higher incidence of thromboembolic events (p = .04; Figure 1A and B). Thromboembolic complications or excessive bleeding occurred in group 1 patients only. Thromboembolic complications were documented in 5 (19%) and excessive bleeding in 2 (8%) patients. Specifically, cerebral stroke (n = 1), intestinal ischemia (n = 2), thrombus formation in inferior caval vein (n = 1) and pulmonary vein (n = 1), thoracic and cerebral bleeding during surgery (n = 1), and massive bleeding from the endotracheal tube (n = 1) were described. Finally, aPTT was 36 ± 9.8 seconds in group 1 and 30 ± 3.6 seconds in group 2 (p = .04).
Results of Coagulation Screening in 26 Single Ventricle Patients and Individual Frequencies of Abnormal Coagulation Parameters in the Study Cohort.
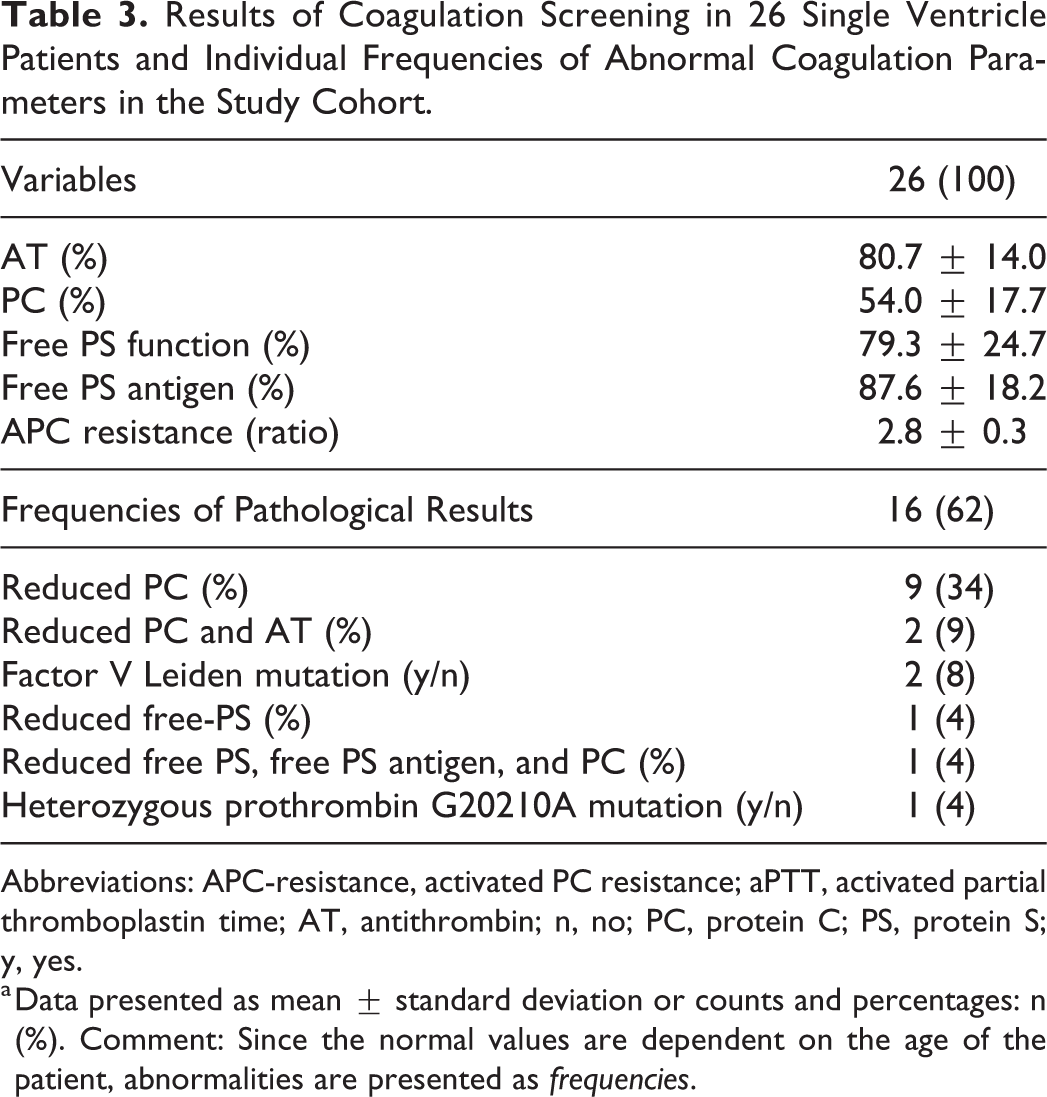
Abbreviations: APC-resistance, activated PC resistance; aPTT, activated partial thromboplastin time; AT, antithrombin; n, no; PC, protein C; PS, protein S; y, yes.
a Data presented as mean ± standard deviation or counts and percentages: n (%). Comment: Since the normal values are dependent on the age of the patient, abnormalities are presented as frequencies.

Box plot diagram to illustrate group comparison (normal coagulation profile = group 2 vs abnormal coagulation profile = group 1) of postoperative need for catecholamine support (A) and time of postoperative hospitalization (B) Results expressed as mean. d indicates days.
The 2 groups showed no statistically significant differences in baseline characteristics (sex, age, cardiac anatomy, and stage of palliation), other laboratory parameters (liver function, hemoglobin, platelet count, and NT-pro-BNP), cardiac catheterization parameters, postsurgical course (regarding length of mechanical ventilation and need of iNO), fenestration at stage III, development of other long-term complications or echocardiographic assessed cardiac function at follow-up (see Tables 1 and 2).
Coagulation Profile and Hemodynamic Parameters
Antithrombin correlated positively with SaO2 (p = .04; r = 0.4; 95% confidence interval [CI]: 0.11-0.78) (Figure 2A) and negatively with Rp (p = .01; r = 0.5; 95% CI: 0.9-0.1; Figure 2B); patients with a reduced AT (%) had lower SaO2 but higher Rp. Protein-C correlated negatively with mPAP (p = .02; r = 0.4; 95% CI: 0.8-0.1; Figure 2C) and PCWP (p = .03; r = 0.4; 95% CI: 0.8-0.3; Figure 2D): reduced PC (%) is associated with higher mPAP and PCWP. Free PS correlated negatively with mPAP (p = .01; r = 0.4; 95% CI: 0.8-0.1; Figure 2E) and free-PS-antigen correlated negatively with mPAP (p = .003; r = 0.6; 95% CI: 0.9-0.2; Figure 2F), meaning an increased mPAP is related to lower free-PS (%) and free-PS-antigen (%). No correlation was found between the coagulation parameters and mRAP, EDP, mTPG, and Rp:Rs.

Correlations between coagulation profile parameters and hemodynamic parameters (A-F). Also, see detailed description in the main manuscript, results section. Results expressed as mean. AT indicates antithrombin; mPAP, mean pulmonary artery pressure; PC, protein C; PS, protein S; PCWP, pulmonary capillary wedge pressure; Rp, pulmonary vascular resistance; SaO2, arterial oxygen saturation.
Discussion
In our single-center analysis, a high frequency of abnormalities in coagulation parameters in patients with UVH physiology through staged Norwood palliation was found. Moreover, we identified possible correlations between hemodynamic and coagulation parameters, while coagulation abnormalities in addition negatively affected the postoperative course.
According to the Virchow triad, thromboembolism could be provoked by altered hemodynamic factors (eg, stasis, nonpulsatile circulation, atrial arrhythmias or sluggish flow), the presence of abnormal surfaces (eg. prosthetic material, blind cul-de-sacs, or surgical scars) or clotting factor abnormalities. All these hemodynamic conditions are present through staged Norwood palliation, especially after stage III. 13,16,17,24 Since thromboembolic episodes occur both on the pulmonary venous and systemic arterial circulation, through all stages of palliation, the presence of a coagulation disorder seems a reasonable hypothesis.
The first report on coagulation abnormalities in Fontan patients was published in 1990 14 and highlighted an imbalance between procoagulant and anticoagulant factors leading to a high thrombotic risk. Later studies showed reduced concentrations of PS, AT and PC after stage II and stage III. 13,16 However, these analyses used adult reference values. 25 Odegard et al have published similar results in children with UVH physiology at all stages of palliation in comparison to age-matched controls. 8 –11 Immediately before stage II 10 and stage III 20 reduced concentrations of PC, PS, factors II, V, VII, IX, and X, plasminogen, fibrinogen, and AT were described. After stage III, 9 the changes in coagulation parameters were qualitatively and quantitatively similar, with the important exception of an increased factor VIII. These findings were confirmed in 2 prospective longitudinal studies. 11,19 In contrast to these results, Rask et al 18 showed a less prothrombotic state late after Fontan surgery and a normalization of PC has also been described before. 15,16 However, PS activity remained reduced and increased platelet activation, probably driven by endothelial damage, was observed. 15 In our analysis, we identified at least 1 highly probable abnormality in coagulation parameters in 62% of our patient cohort, most frequently reduced PC.
Deficiencies of AT, PC, or PS, both inherited and/or acquired, create a prothrombotic state. 26 The underlying cause, as to whether the unbalanced coagulation system abnormalities are linked to delayed maturation of the coagulation system as a result of physiological alterations (such as a subclinical form of PLE, cyanosis, or low cardiac output), remains a speculative and unlikely hypothesis. 8,27 Since PLE is a late complication of a Fontan circulation, it could be described only in 2 of our patients (one with an abnormal coagulation); therefore, not many conclusions could be drawn. Although PC has a short biological lifetime, a vitamin K deficiency remains an unlikely explanation of their reduced concentrations. In fact, normal vitamin K levels, suggesting preserved enteric absorption of lipid-soluble vitamins, have been described before in this patient population. 14 It could be hypothesized that their deficit could result from fluctuating and transiently lowered vitamin K levels or by temporal dysfunction of the vitamin-K-dependent carboxylase. An acquired deficiency of PC, PS and AT has been reported in severe liver disease, during disseminated intravascular coagulation and in the immediate postoperative period. 16 Consequentially, the role of an increased systemic venous pressure and hepatic congestion (or low perfusion due to low-cardiac output) in reducing protein synthesis in the liver has been indicated as a potential driving cause. Severe hepatic dysfunction was not found in our patients; however, the presence of elevated transaminases did not appear to be associated with coagulation abnormalities in our study nor in previous reports in literature. 8,9,13,14,19 This is also supported by the presence of coagulation abnormalities when inferior caval vein pressure is not increased. 16
These considerations together with the fact that the abnormalities in coagulation factors are present earlier in the course of staged SV palliation seem to suggest that these abnormalities do not result from the Fontan physiology only. In accordance with these considerations is the fact that we only had 3 participants in a Fontan circulation in our patients’ group. At stages I and II, chronic cyanosis and secondary polycythemia (with associated decreased absolute amounts of clotting factors) may induce a hypercoagulable state by shifting the endothelial phenotype toward a prothrombotic state. 12,28,29 In fact, hypoxia suppresses thrombomodulin in endothelial cells, resulting in a reduced activation of PC. 12 In our analysis, we did not investigate the complete profile of coagulation parameters; however, postoperative bleeding was not frequent, pointing to a misbalance toward a procoagulatory state. At stage III, the higher shear stress on the wall of the pulmonary vasculature seems to alter endothelial function, leading to an increased risk of thrombus formation as well as to vasoconstriction. 12,17 Finally, an elevated systemic venous pressure and abnormal flow pattern may also lead to thrombus formation. 17
The reduction of all 3 anticoagulants (PS, PC, and AT) suggests that the deficiency is acquired rather than hereditary. A higher prevalence for heterozygous factor V Leiden mutation or of single-nucleotide polymorphisms of genes encoding proteins involved in coagulation pathways in patients with congenital heart disease or directly after surgery has been reported before. 17,21,22 However, we did not find an increased prevalence in our pilot analysis. In fact, only 2 patients showed a factor V Leiden mutation and 1 a prothrombin G20210A heterozygous. Nevertheless, our preliminary results appear to support the use of these 2 genetic markers in a clinical setting to identify patients at an increased risk of thromboembolic complications since 2 out of these 3 patients experienced severe thromboembolic events direct postoperatively.
To our knowledge, our study is the first to suggest that an abnormal coagulation profile could be associated with impaired invasive hemodynamic parameters. Whether the pathological findings in coagulation parameters negatively influence hemodynamics or are a result of impaired hemodynamic parameters, remains unclear. The key question regarding which role the type of circulation plays in this association also remains unanswered, especially since we only have a punctual assessment and could enroll only 3 participants with a Fontan circulation. However, our results clearly point toward an early manifestation of coagulation abnormalities. One hypothesis might be that the altered coagulation relates to a procoagulatory state, which might be the fundamental for microthrombus formation in the pulmonary vasculature (and/or systemic–pulmonary shunt). Microthrombus formation might degenerate into altered (impaired) hemodynamics. This could be sustained by the positive correlation between AT and SaO2 (described once before after stage III 19 ), in the sense that lower AT levels are associated with lower oxygen saturation. The association between Rp and SaO2 is also in accordance with this theory. The increased Rp of the patients with a reduced SaO2 could potentially result from microthrombus formation in the peripheral pulmonary vascular bed, which then augments vascular resistance. Our finding of the relation between a diminished PC and an increased PCWP would point into the same direction because we measured the occlusion pressure of the lung capillaries that could be influenced by microthrombus formation. The correlations of reduced PC and PS with increased mPAP would potentially also support this hypothesis, because these microthrombus formations could impair the hemorheology and increase the pressure in the pulmonary arteries. However, these associations between hemodynamic data and coagulation factors remain controversial, especially since other studies were unable to demonstrate any significant correlation with hemodynamics. 8 –11,16 Nevertheless, a procoagulatory state appears to have a negative influence on the hemodynamic parameters.
The negative influence of altered coagulation parameters on the postoperative course seems to be confirmed by a longer postoperative hospital stay, a longer need of catecholamine support and a higher incidence of postoperative chylothoraxes in patients with abnormal coagulation profile in our patients. Theoretically, this could also be due to an association between impaired ventricular function and impaired hemodynamic parameters prior to surgery in patients with abnormal coagulation parameters. However, no association between the NT-pro-BNP values and the presence of clotting abnormalities could be described.
Finally, the higher prevalence of thromboembolic events and excessive bleeding that characterized only patients with an altered coagulation remark the clinical relevance of these results of our analysis. It is important to report, that (considering the retrospective design of our study) we could not rule out other causes (eg. postoperative impaired perfusion) for intestinal ischemia. However, we only included the 2 cases where the evaluation of the visceral surgeon considered a thromboembolic event as very likely due to the intraoperative findings.
Limitations
Our study assessed a heterogeneous patient population (different cardiac anatomies, different stages of palliation, etc) and we did not (yet) examine the full complement of coagulation factors, especially platelet function tests were not assessed. Furthermore, since no age-matched controls were enrolled, the definition of normal/abnormal coagulation profile relies on previously published norm values and this might constitute a relevant bias in the interpretation of the results.
Moreover, the family history for coagulation abnormalities was not taken into account and the analysis was retrospectively performed, with a small sample size and at a single center. Especially regarding a comparison of the postoperative course, although group 1 and group 2 are statistically comparable, the role of the different surgical interventions (stage II or III) could not be assessed, which implements limitation to the interpretation of our results. Finally, without lung biopsies and histological assessment, the hypothesis of the presence of microthrombus formation in the pulmonary circulation remains unprovable. Considering all these limitations, our results are very interesting hypotheses that support the introduction of a larger, prospective (potentially multicenter), longitudinal trial also assessing age-matched controls in the near future.
Conclusion
Abnormalities in coagulation parameters are common in SV patients. A correlation between hemodynamic and coagulation parameters can be hypothesized. Coagulation abnormalities seem to constitute a preoperative risk factor and seem to affect postoperative course.
Footnotes
Authors’ Note
Data presented at the 53rd AEPC Meeting, May 15-18, 2019, Seville, Spain.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.