
Abstract
The current systematic review and meta-analysis aimed to summarize the results of all available studies to compare the efficacies of rituximab and conventional treatment for acquired thrombotic thrombocytopenic purpura (TTP). Three investigators independently searched studies in the MEDLINE and EMBASE databases published before December 11, 2018. To be included in the meta-analysis, studies needed to be randomized-controlled or cohort studies comparing the efficacies of rituximab and conventional therapy for TTP treatment. The effect estimates and 95% confidence intervals (CIs) from each study were collected, and Mantel-Haenszel methods were used to pool the data. A total of 570 patients from 9 eligible studies were included in the meta-analysis (280 patients in the rituximab arm and 290 in the conventional treatment arm). Patients receiving rituximab in an acute phase to induce disease remission had a significantly lower relapse rate than those given conventional treatment (odds ratio [OR]: 0.40, 95% CI: 0.19-0.85, P = .02, I2 = 43%). Similarly, the relapse rate in the rituximab group for preemptive therapy to prevent clinical relapse was also significantly lower than in the control group (OR: 0.09, 95% CI: 0.04-0.24, P < .00001, I2 = 11%). Furthermore, the conventional treatment group had a significantly higher mortality rate than the rituximab group during the follow-up (OR: 0.41, 95% CI: 0.18-0.91, P = .03, I2 = 0%). Rituximab offered high efficacy for the prevention of relapses and lower mortality rate in cases of acquired TTP.
Introduction
Thrombotic thrombocytopenic purpura (TTP) is a serious condition that results in classic presentations, including thrombocytopenia, microangiopathic hemolytic anemia, fever, renal insufficiency, and neurological deficits.
1
The pathogenesis is caused by a decrease in the level of a metalloprotease named ADAMTS13 (
In the case of acquired TTP, the treatments available comprise total plasma exchange with plasma infusion, steroids, immunomodulator agents (vincristine and cyclosporin), and rituximab; these drugs are given due to the autoimmune nature of acquired TTP. 7 –9 Rituximab, the humanized anti-CD20 monoclonal antibody, is introduced to reduce the incidence of relapsed TTP. 10 Its actions are a decrease in the production of antibodies against ADAMTS13 and a resumption of ADAMTS13 activity. 11 However, whether rituximab should be a frontline treatment or only reserved for patients with a suboptimal response to initial treatments for autoimmune TTP is controversial. The current systematic review and meta-analysis were performed with the aim of including all available studies and summarizing their results to compare the efficacies of rituximab and conventional treatment for acquired TTP.
Methods
Data Sources and Searches
Three investigators (C.W., W.O., and N.O.) independently searched studies published in the MEDLINE and EMBASE databases before December 11, 2018 using a search strategy that included the terms for TTP and rituximab. Supplementary Data 1 displays the search strategy for our meta-analysis. We further examined the references of the eligible publications to identify additional articles for inclusion. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement was used as a guideline for performing the current study; it is provided as Supplementary Data 2. 12
Selection Criteria and Data Extraction
The studies included in this meta-analysis needed to be randomized-controlled studies or cohort studies (either prospective or retrospective) that compared the efficacies of rituximab and conventional therapy for TTP treatment. Furthermore, they had to report at least one of our primary outcomes of interest, which was either the relapse rate after remission of each treatment or the mortality rate. All 3 investigators independently assessed the eligible articles. In the case of disagreements on whether a particular publication should be included, all investigators jointly reviewed it before making the final decision.
Outcome Definitions
Complete remission was defined as the achievement of a platelet count of ≥150 × 109/L and a sustained response for ≥30 days after plasma exchange was stopped. Relapse was defined as the recurrence of an acute episode of TTP after remission. 13
Quality Assessment
The quality of each included randomized-controlled study was evaluated by using the Jadad quality assessment scale. 14 The quality of the included nonrandomized studies was evaluated with the Newcastle-Ottawa Scale. This 3-item scoring system assesses the selection of the participants, the comparability between the groups, and the ascertainment of exposure (for case-control studies) and the outcome of interest (for cohort studies). 15
Statistical Analysis
All statistical data were analyzed using Review Manager 5.3 software from the Cochrane Collaboration (London, United Kingdom). The effect estimates and 95% confidence intervals (CIs) from the individual articles were collected, and Mantel-Haenszel methods were used to pool the data. 16 Cochran Q test was then calculated and quantified using the I2 statistic to assess the statistical heterogeneity of the publications. They were classified as follows: 0% to 25% represented an insignificant heterogeneity; 26% to 50% low heterogeneity; 51% to 75% moderate heterogeneity; and >75% high heterogeneity. 17 Due to the high likelihood of between-study heterogeneity, we preferred the random-effects to the fixed-effects model. Publication bias was not evaluated because of the small number of included studies (less than 10). Values of P less than .05 were considered statistically significant.
Results
A total of 1877 potentially relevant articles were found in the 2 databases (348 from MEDLINE and 1529 from EMBASE). We excluded 336 duplicated reports, and the remaining 1541 were evaluated for relevance via a review of their titles and abstracts. Of those, 1513 were excluded according to the exclusion criteria, which were: (1) reviews, or meta-analyses, or commentaries; (2) reports irrelevant to TTP; (3) articles irrelevant to a comparison between rituximab and conventional treatments; and/or (4) publications with no primary end points. The full-lengths of the remaining 28 articles were manually reviewed, resulting in a further 19 being excluded because they met the exclusion criteria. Nine publications finally fulfilled the inclusion criteria for the meta-analysis; they comprised 5 prospective cohort studies and 4 retrospective cohort studies. 18 –26 The literature review process is summarized in Figure 1.
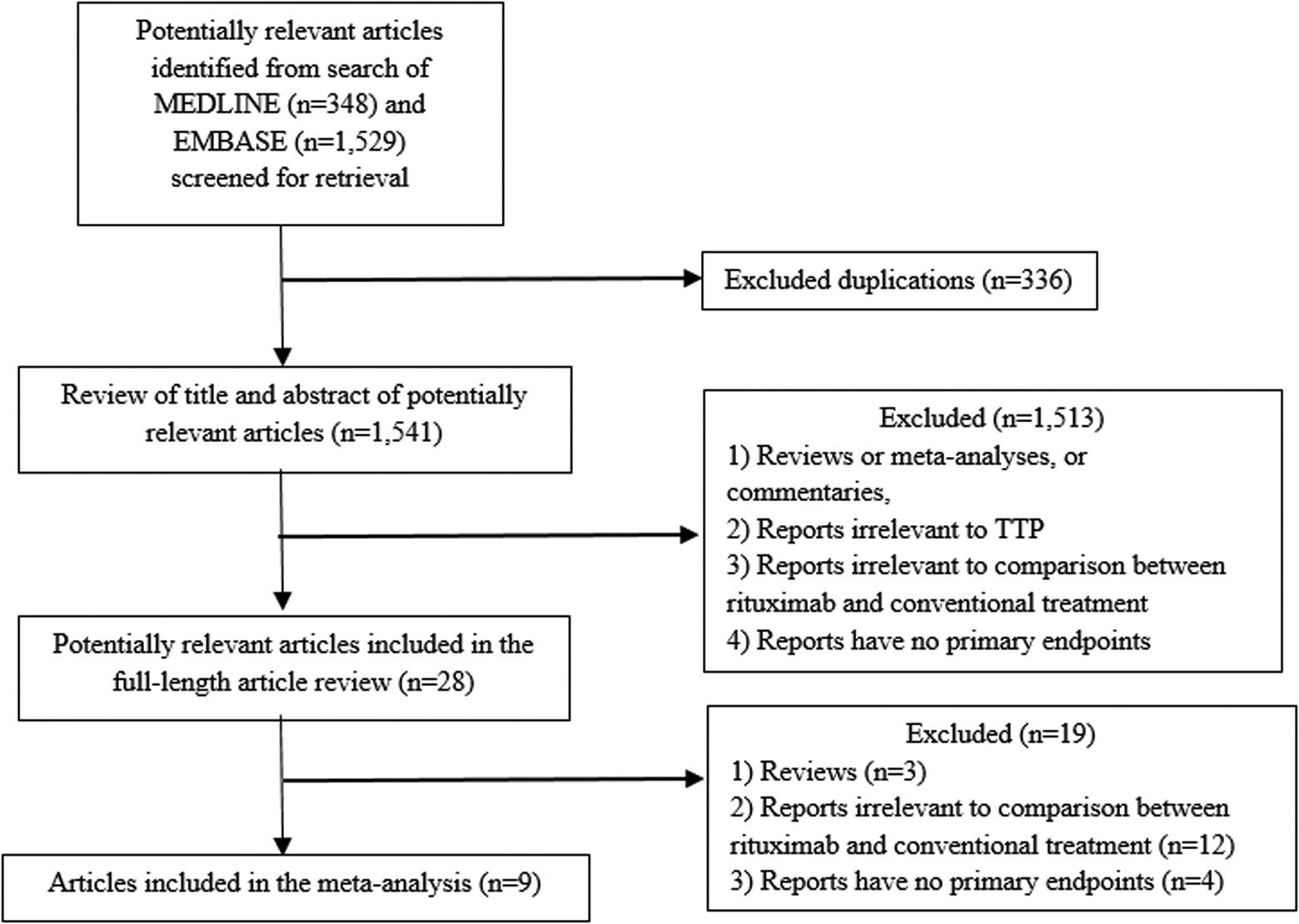
The literature review process.
Baseline Patient Characteristics
A total of 570 patients were included in this meta-analysis (280 in the rituximab arm and 290 in the conventional treatment arm). The age range for the rituximab arm was 18 to 79 years, whereas it was 16 to 88 years for the conventional treatment arm. Approximately 3-quarters of the patients in each group were female. More than 30% of the rituximab group participants were either relapsed or refractory patients with TTP, whereas the corresponding figure for the conventional treatment group was noticeably lower at 22.8%. In most of the studies, the proportion of enrolled patients with TTP who had ADAMTS13 activity represented less than 10% of the participants in each group. Almost all cases in both groups received plasma exchange and corticosteroids as their TTP treatment. The rituximab protocols were divided into 2 purposes for TTP treatment in the included studies. Most included studies used rituximab in acute phase to induce TTP remission, whereas other 2 studies used preemptive rituximab treatment during remission (in case of persistently low ADAMTS13 levels) to prevent clinical relapse. The baseline patient features, treatments, median follow-up periods, study types, and quality assessment scores for the 9 included studies are detailed in Table 1.
Baseline Patient Characteristics of Each Included Article.

Abbreviations: ADAMTS13, a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13; CSA, cyclosporin A; Cyclo, cyclophosphamide; F, Female; iv, intravenously; M, male; MMF, mycophenolate mofetil; NR, not reported; P, prospectively; PEX, plasma exchange; R, retrospectively; RTX, rituximab.
Long
-
Term Remission and Mortality Outcomes
The relapse rate was reported in 8 studies (a 1-year follow-up relapse rate in 1 study, 18 a 2-year rate in 3 studies, 19,23,24 a 3-year rate in 3 studies, 20,22,26 and a 4-year rate in 1 study 25 ). Six out of 8 studies demonstrated rituximab role in an acute phase to induce disease remission. The pooled relapse rate found that patients who received rituximab had a significantly lower relapse rate than those given conventional treatment (odds ratio [OR]: 0.40, 95% CI: 0.19-0.85, P = .02, I2 = 43%; Figure 2A). 18 –20,23 –25 Likewise, the relapse rate in the rituximab group was also significantly lower than the control group by pooling the data of other 2 studies using rituximab for preemptive therapy to prevent clinical relapse (OR: 0.09, 95% CI: 0.04-0.24, P < .00001, I2 = 11%; Figure 2B). 22,26 Furthermore, the conventional treatment group had a significantly higher mortality rate than the rituximab group during the follow-up (OR: 0.41, 95% CI: 0.18-0.91, P = .03, I2 = 0%; Figure 3). 18 –24,26

Forest plots of the odds ratio of the relapse rates after complete remission of the rituximab and conservative treatment arms dividing on roles of rituximab therapy: (A) acute treatment; (B) preemptive treatment.
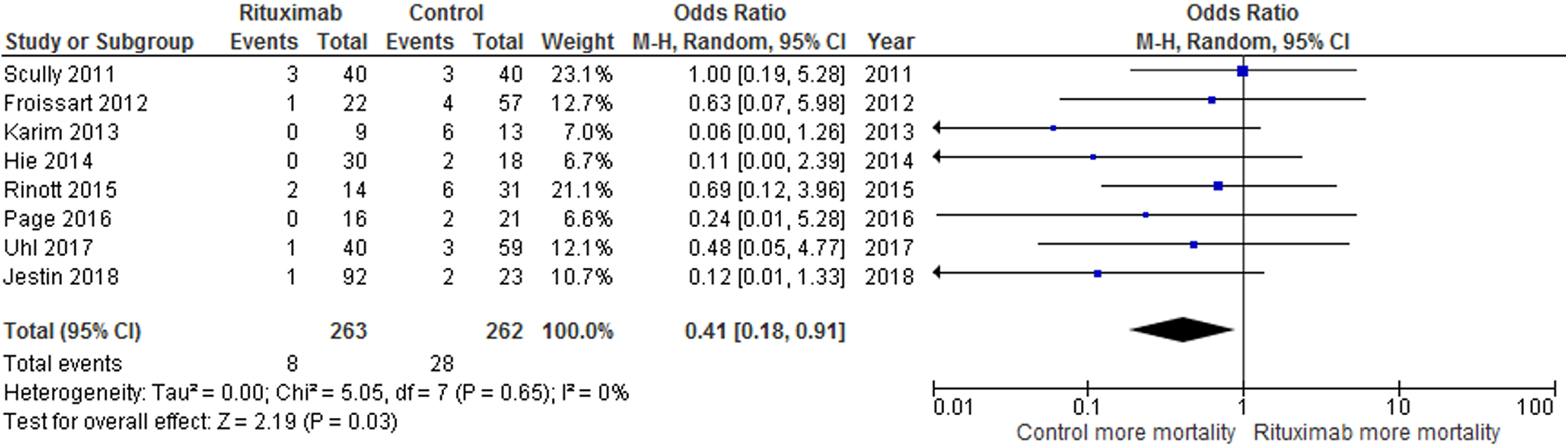
Forest plots of the odds ratios of the mortality rates of the rituximab and conservative treatment arms.
Discussion
This is the first meta-analysis to compare the efficacies of rituximab and conventional treatment for patients with TTP. There were no significant differences in the baseline patient characteristics of the 2 groups (including age, gender, and the proportion of patients who had ADAMTS13 activity). However, the proportion of relapsed/refractory TTP cases in the rituximab group was higher than that in the conventional treatment group.
Although plasma exchange, significantly reducing the early mortality rate, yielded an advantage in emergency management for acquired TTP, long-term relapse rate was quite high if novel medications or immunosuppressive drugs were not integrated for the treatment. 27 Corticosteroid is commonly an adjuvant therapy combined with plasma exchange, which could decrease ADAMTS13 autoantibodies and improve ADAMTS13 activity. 28 Nevertheless, the exacerbate rate remained not low from a recent study, with the figure nearly of 10% at the first month follow-up. 28 Rituximab affects to reduce B-cell lymphocytes, and subsequently decrease the production of ADAMTS13 autoantibodies. 29 It was also approved to render high sustained response in immune thrombocytopenia patients from a previous meta-analysis. 30 The pooled forest plot of the relapse rate in TTP from this meta-analysis showed a significantly lower rate for the rituximab group in both acute and preemptive treatment purposes than the conventional treatment group during the 1- to 4-year follow-up period. The patient who received rituximab also had lower mortality rate when compared to conventional treatment. Our results indicated that rituximab combined with corticosteroid showed higher efficacy to prevent relapse rate and lower mortality rate in newly diagnosed acquired patients with TTP. Furthermore, we noticed that the proportion of relapsed/refractory patients with TTP in the rituximab group represented nearly one-third of the total cases. We therefore support the use of rituximab as an adjuvant treatment in combination with plasma exchange in newly-diagnosed TTP and as a second-line treatment for patients with acquired TTP.
There are some limitations to this study. Firstly, none of the included studies is randomized trial; therefore, these studies are subjected to have selection biases especially the differences in baseline characteristics between 2 groups such as a proportion of age-group, a proportion of refractory disease patients, and other additional immunosuppressive therapies. There may be more immunosuppressive therapies in rituximab group because the disease is generally more resistant. For instance, more steroid uses in Scully et al study and some of more other additional immunosuppressive therapies use in Page et al and Jestin et al studies. Immunosuppression may suppress ADAMTS13 antibody, resulting in lower relapse rate. Moreover, the studies that used historical controls have longer follow-up time in the control groups, and leads to falsely high relapse rate and mortality rate in Hie et al, Rinott et al, and Jestin et al studies. In addition, due to limited number of studies included in the meta-analysis, a publication bias assessment could not be performed.
Conclusions
Rituximab provided a high efficacy to prevent relapses in cases of newly diagnosed acquired TTP. Additionally, its effectiveness with the subgroup of patients with relapsed/refractory TTP was demonstrated through the provision of good outcomes.
Supplemental Material
Supplementary_Data_1_and_2 - Comparison of the Long-Term Remission of Rituximab and Conventional Treatment for Acquired Thrombotic Thrombocytopenic Purpura: A Systematic Review and Meta-Analysis
Supplementary_Data_1_and_2 for Comparison of the Long-Term Remission of Rituximab and Conventional Treatment for Acquired Thrombotic Thrombocytopenic Purpura: A Systematic Review and Meta-Analysis by Weerapat Owattanapanich, Chompunut Wongprasert, Wannaphorn Rotchanapanya, Natthida Owattanapanich, and Theera Ruchutrakool in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Author’s Note
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request. Our institution does not require ethical approval for performing a meta-analysis as this study did not directly involve human subjects. Informed consent for patient information to be published in this article was not obtained because this study did not directly involve human subjects.
Author’s Contributions
All authors designed the study. WO, CW, and NO collected the data. WO performed the statistical analyses. WO, CW, and WR drafted the manuscript and revised the final manuscript. TR made critical revisions to the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.