
Abstract
The aim of our study was to quantify risk factors for venous thromboembolism (VTE) during the puerperal period. The case–control study was conducted in Women’s Hospital, Zhejiang University, China, from January 2006 to December 2016; cases of hospitalized VTE within 1 week after delivery were identified according to International Classification of Diseases, Ninth Revision, Clinical Modification codes. Control postpartum women without VTE were randomly selected, matched on birth day, age, delivery mode, and number of fetus with 4:1 ratio. Clinical risk factors for postpartum VTE and coagulation parameters were analyzed. We found independent variables that were significantly related to postpartum VTE (all P < .05) in a binary logistic regression analysis included preeclampsia/eclampsia (odds ratio [OR], 2.89; 95% confidence interval [CI], 1.56-5.37) and postpartum hemorrhage (OR, 4.6; 95% CI, 1.71-12.40). D-dimer was the only biomarker that statistically significant associated with postpartum VTE in 3 days after delivery (all P < .05). These findings showed preeclampsia/eclampsia and postpartum hemorrhage were important risk factors for early VTE during puerperal period. A higher level of D-dimer was more meaningful than other coagulation parameters to suspect early thrombotic disease after delivery.
Introduction
Venous thromboembolism (VTE) is a rare but serious maternal complication around delivery. It is one of the leading causes of maternal death and mortality in developed countries. 1 Previous studies have documented more than 20-fold greater VTE in pregnant women compared to nonpregnant women. 2 –4 Since several important physiologic changes during pregnancy increase the risk of development of VTE, such as an increase in the coagulation factor II, V, VII, VIII, IX, X a decrease in endogenous phospholipid-binding anticoagulation protein S, hypercoagulability caused by hemostatic system, changes in venous outflow induced by hormones, mechanical obstruction by the uterus, and vascular injury. 5,6 Since universal thromboprophylaxis may not be cost effective or safe because of the risk of allergy and bleeding, different studies have identified different risk factors for pregnancy-related VTE, such as advanced age, greater body mass index (BMI), black race, cesarean delivery, preterm delivery, preeclampsia, postpartum hemorrhage, or infection. Most of these studies come from Western countries, and it is not well known which of these risk factors are high enough risks to warrant prolonged postpartum thromboprophylaxis and how combinations of independent risk factors affect overall VTE risk, especially in Asian countries. 7
Most of the studies have examined the risk factors of VTE which happened up to 12 weeks during postnatal. Few studies have evaluated the early VTE risk factors that occur 1 week after delivery, 8 so it is still unclear about the risk factors which happened during early period postpartum. More information about VTE risk factors during early postpartum period could benefit clinicians with the decisions of postpartum low-molecular-weight heparin prophylaxis in specific risk groups.
The purpose of this study was to identify various risk factors for VTE during early postpartum period and tried to discover hematologic index that would help to predict VTE risks.
Methods
Data Sources and Study Population
This retrospective case–control study included all postpartum patients with deep venous thrombosis (DVT) or pulmonary embolism (PE) in Women’s Hospital, Zhejiang, China, from January 2006 to December 2016. The study was approved by the Medical Research Ethics Review Board of the hospital. All patients were of Chinese Han ethnicity. We identified all VTEs including DVT or PE experienced by women (excluding superficial VTE) in our cohort. All Chinese women provided that they had no history of previous VTE, other cardiovascular diseases, or cancer; thus, we assessed only pregnancy-related VTEs. Venous thromboembolism was based on a recorded medical code assigned by a physician and supplemented by evidence of vascular ultrasound or computed tomography angiography.
Cases were defined as women who had experienced an incident hospitalized DVT or PE within 1 week following delivery. We identified 102 cases who had DVT or PE during the postpartum period and without a previous VTE history.
Controls were defined as women without VTE within 1 week following delivery. We randomly sampled 408 women who had delivered in Women’s Hospital, Zhejiang, China, from January 2006 to December 2016, frequency-matched to cases on birth day, age, delivery mode, and number of fetuses with 4:1 ratio. Exclusions were applied to women with a history of tumor, chronic obstructive pulmonary disease (COPD), anticardiolipid antibody syndrome (ACLAS), and coagulation disorders.
Risk Factors
For each pregnancy, information on maternal factors before or after pregnancy was extracted from the patient’s medical record which included maternal age, BMI, and weight gain during pregnancy. Pregnancy-related factors considered were gravidity, parity, mode of delivery, birth outcome (live or stillborn child), length of gestation, and multiple gestation. Pregnancy complications (including gestational diabetes mellitus, eclampsia/preeclampsia, placental abruption, and postpartum hemorrhage) were extracted if they occurred during the pregnancy/postpartum period. Women were defined as having gestational diabetes if they had a first record of diabetes during pregnancy and no prior prescriptions for oral hypoglycemics or insulin. Preeclampsia is defined as a medical code indicating the condition during pregnancy or at least 3 readings of high blood pressure after 20 weeks’ gestation (systolic ≥ 140 mm Hg and/or diastolic ≥ 90 mm Hg), with no antihypertensive treatment before pregnancy and with proteinuria ≥ 300 mg/24 h or ≥1 + dipstick in random urine samples or new signs of end-organ dysfunction. The onset of convulsions in a woman with preeclampsia that cannot be attributed to other causes is termed eclampsia. Gestational hypertension is characterized most often by new-onset elevation of BP after 20 weeks of gestation, often near term, in the absence of accompanying proteinuria. Placental abruption is suspected when a pregnant mother has sudden localized abdominal pain with or without bleeding, excluding other possible sources of vaginal bleeding or abdominal pain. Physical examination of uterine tension and ultrasound may be used to help diagnosis. Postpartum hemorrhages defined as blood loss more than 500 mL following vaginal delivery or 1000 mL following caesarean section in the first 24 hours following delivery. Characteristics of newborn include birth weight (categorized into low <2500 g, normal 2500-4000 g, and large >4000 g following the Centers for Disease Control and Prevention categories 14), neonate gender, and Apgar score (1 minute, 5 minutes).
Information on important comorbidities was extracted based on previous literature and the current RCOG guideline on thromboprophylaxis. 7 Women who had ever been diagnosed with cancer, COPD, systemic lupus erythematosus, nephrotic syndrome, or cardiac disease (including congestive cardiac disease, coronary artery disease, congenital heart disease, cardiomyopathy, angina, or myocardial infarction) during or before pregnancy were excluded. We also excluded women having preexisting diabetes or preexisting hypertension.
Statistical Analysis
Univariable analysis was used to examine the significance of the predictor independent variables in relation to PE or DVT. Quantitative data were expressed as mean (SD), and categorical data were expressed as percentages. At univariable analysis, quantitative variables were analyzed using the t test when the data met homogeneity of variance or the Mann-Whitney U test when the data did not meet homogeneity of variance, and constituent ratio data were analyzed using the χ2 test. Binary logistic regression analysis was performed for the variables that at univariable analysis were associated with PE or DVT. The value P < .05 was considered statistically significant. For multivariable analysis, a binary forward stepwise logistic regression analysis was used, with P < .10 as the criterion for entry into the model. The variable with the highest P value was then successively deleted until only a variable with P < .10 remained. All statistical tests were 2-sided, and statistical significance was accepted at P < .05. Statistical analyses were performed using commercially available software (SPSS for Windows, version 13.0; SPSS, Inc., Chicago, Illinois).
Results
Basic Characteristics
We identified 102 women who experienced a VTE event in 1 week following delivery (95 DVT and 7 PE with or without DVT) and 408 women who did not experience a VTE event between January 2006 and December 2016. The basic characteristics for each pregnancy are summarized in Table 1. There were no significant differences in matched characteristics.
Basic Characteristics of Case and Control Patients.

Abbreviation: IQR, interquartile range.
Risk Factors for DVT During the Postpartum Period
The prevalence of related risk factors for postpartum VTE are shown in Table 2. In particular, cases had a higher rate of VTE with preterm delivery, preeclampsia or eclampsia, postpartum hemorrhage, and low birth weight. The distribution of related risk factors was analyzed with univariable statistics in the case and control group (Table 2). Deliveries ≥2, preeclampsia/eclampsia, postpartum hemorrhage, and birth weight especially <2500 g (low birth weight) were statistically significant characteristics that were associated with postpartum DVT (all P < .05). However, BMI, weight gain in pregnancy, and rates of gestational diabetes mellitus, preterm delivery(<37 weeks), and birth sex ratio did not demonstrate a statistically significant effect in prediction of postpartum DVT.
Single-Variable Statistical Analysis of Clinical Risk Factors for Postpartum DVT Between 2 Groups.a,b

Abbreviations: BMI, body mass index, calculated as weight in kilograms divided by height in meters squared; CI, confidence interval; DVT, deep venous thrombosis; OR, odds ratio.
a Unless otherwise indicated, values are given as either mean (SD) and range or No. (%).
b The t test was applied to quantitative data; χ2 test was applied to qualitative data.
A binary multivariable logistic regression analysis in relation to postpartum DVT is given in Table 3. Independent variables that were significantly related to postpartum DVT in the binary multivariable logistic regression analysis included preeclampsia/eclampsia and postpartum hemorrhage. Postpartum DVT was, thus, evident in patients with preeclampsia/eclampsia and postpartum hemorrhage.
Binary Multivariable Statistical Analysis of Clinical Risk Factors for Postpartum DVT.

Abbreviations: CI, confidence interval; DVT, deep venous thrombosis; OR, odds ratio; SE, standard error.
Coagulation Function for DVT During the Postpartum Period
Coagulation parameters including prothrombin time, activated partial thromboplastin time, thrombin time, plasma fibrinogen, platelets, international normalized ratio, and
Hematologic Indices Compared Between the Case and Control Group by t Test.

Abbreviations: INR, international normalized ratio; APTT, activated partial thromboplastin time, Fbg, plasma fibrinogen; PT, prothrombin time.
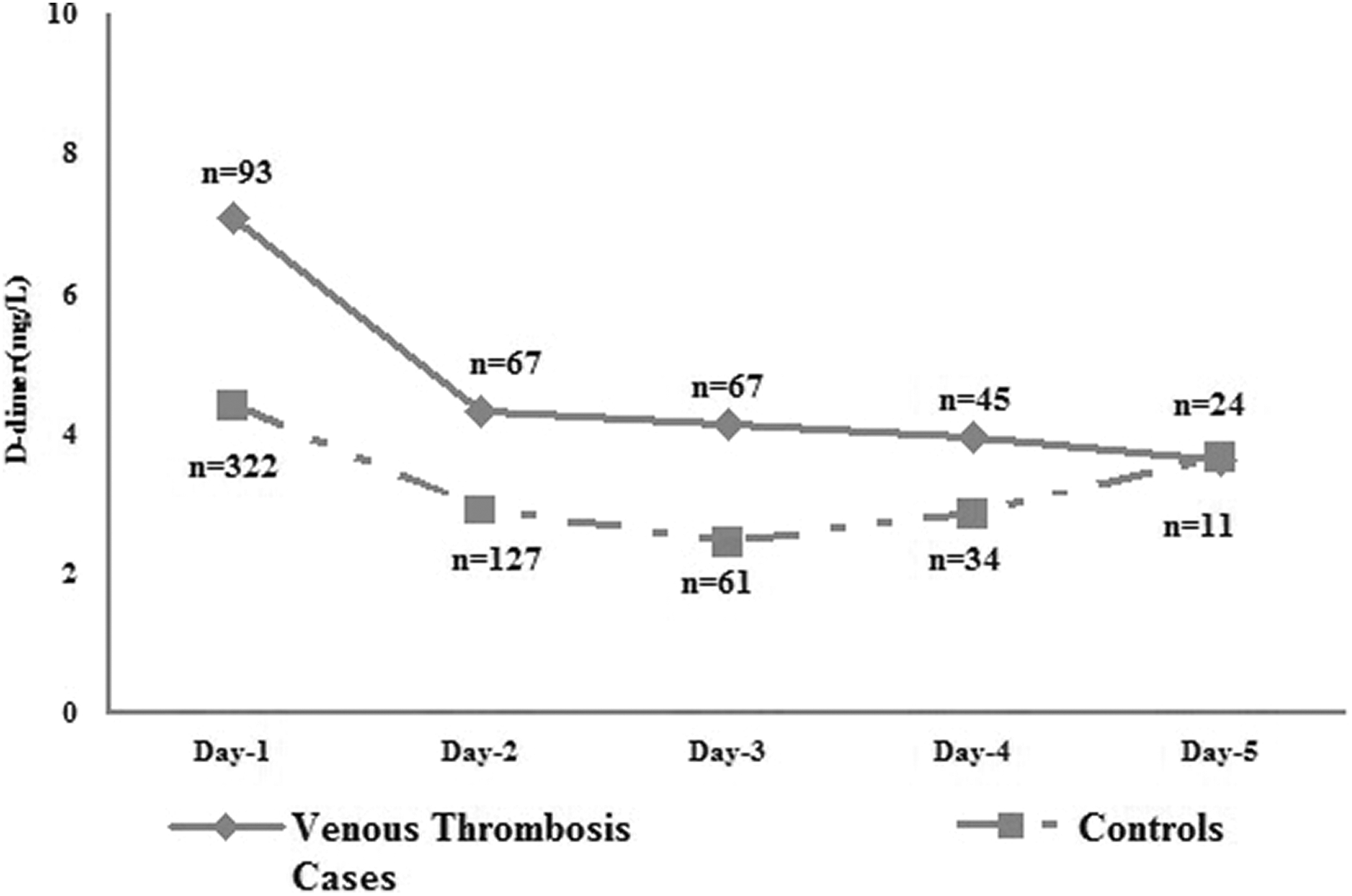
The average of D-dimer in cases and controls during postpartum. Dash line indicated control groups and solid line indicated venous thrombosis groups. Since normal D-dimer was not tracked, not all pregnancies had complete data during 5 days after delivery. The numbers of maternal who had a D-dimer monitoring were signed.
Discussion
This analysis examined the risk factors of early postpartum VTE in Asian population. Most of the studies have examined the risk factors for VTE that happened in 6 weeks to 3 months during postpartum. We were more interested in early postpartum VTE, since some studies that found the highest rates during the first few weeks postpartum. 9 –12 Our results agree with several other studies that have identified women with pregnancy complications to be at higher risk for postpartum VTE. 9,10,13, 14 The contribution of pregnancy-related risk factors to VTE formation is likely mediated through their effects on coagulability and acute perturbations such as hemorrhage may compound the changes associated with the postpartum hemostatic system to further increase VTE formation.
Our results showed a strong association between preeclampsia/eclampsia and risk of VTE which was agreed with previous studies. 10,15 Anne et al reported that patients with preeclampsia had higher VTE rates in 2 weeks after delivery, especially in second postnatal week. Our findings showed that the occurrence of preeclampsia/eclampsia was 19.6% compared to 9.1% of the controls within the first 1 week following delivery. In patients with preeclampsia, a reactive thrombocytosis during 6 to 14 days after initial thrombocytemia 16 might be a potential cause of the disease. Therefore, routine medical thromboprophylaxis administered 2 to 7 days after cesarean section probably prevents some events of VTE during the first postnatal week.
Postpartum bleeding increased the risk of puerperal VTE substantially in accord with previous studies. 17 –19 In the present study, we observed that the postpartum hemorrhage was an independent variable significantly related to VTE. Severe bleeding remained a strong risk factor regardless of mode of delivery. For one reason, tissue trauma during delivery and the loss of a large volume of full blood may lead to coagulopathy and trigger coagulation; for another, transfusion and the use of coagulation products could lead to thrombosis. 18
A previous study found that weight gain during pregnancy was a more important predictor of VTE risk 19 but not in our results. Jacobsen et al found weight gain during pregnancy of more than 21 kg to increase the risk of VTE in the puerperal period. 10 Our findings showed that the average weight gain was 13.9 kg in cases group and 14.5 kg in control group; the relatively small weight gain may explain our different results. Several studies have found an association between BMI in early pregnancy and VTE during pregnancy and the puerperal period. 18 –23 High risks for VTE were observed in women with BMI between 30 and 40 kg/m2 in Sultan et al study. 13 Our findings showed little association between obesity and VTE during pregnancy, it might have contributed to relatively smaller population of obesity in our group (16.3% in case group and 16% in control group).
The association between multiple pregnancies and VTE in pregnancy is a controversial issue. Some studies stated strong relation between multiple pregnancies and VTE but not in the puerperal period. 4,14,24 Virkus et al stated that multiple pregnancy was an important risk factor 25 ; however Sultan et al found that multiple pregnancy was not a predictor of VTE risk. 13 We arrived at the outcome that multiple pregnancies might be a potential risk for VTE but not an independent variable. The arguments need more researches to assess.
Previous research reported that birth weight of <2500 g at term is a strong and independent risk factor for postpartum VTE. 26 Our findings suggested that birth weight of <2500 g was a risk factor for postpartum VTE but not an independent variable. Biological explanations for this observed association exist, of which placental insufficiency is most plausible. Previous knowledge indicates that ischemic placental disease may be linked to both low birth weight and an increased venous thrombotic risk. 10,26 Other conditions of ischemic placental disease, preeclampsia, and placental abruption are also consistently documented risk factors for maternal postpartum VTE. 10,13 Furthermore, histological placental examinations of women with growth restriction provide evidence of both maternal and fetal vascular obstruction. 27,28 Therefore, we could postulate the presence of thrombophilic traits leading to both ischemic placental disease and an increased venous thrombotic risk.
A few alternative biomarkers to replace
These results underscore the needs for clinicians to have heightened awareness of the elevated and prolonged risk of early postpartum VTE, particularly among women with preeclampsia/eclampsia or postpartum hemorrhage complications, especially who had a high
Footnotes
Authors’ Notes
Zhi-Hua Zhou and Yuan Chen contributed equally to this study. Z.H.Z. and Y.C. contributed to collection, analysis, and interpretation of data as well as article preparation. B.H.Z. and Y.J. contributed to interpretation of data. Q.L. contributed to study design and data interpretation and the article preparation, she is the guarantor of this work and, as such, has full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Ethical approval to report this case series was obtained from Medical Research Ethics Review Board of Women’s Hospital, Hangzhou, China. Informed consent was not obtained because no patient information was published herein.
Acknowledgments
The authors thank the Staff at women’s hospital, Zhejiang University for technical assistances and facility supports.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Key Subjects Group of Reproductive Medicine, School of Medicine, Zhejiang University, funded by National Nature Science Foundation of China grant 81571447, 81501339.