
Abstract
The purpose of this study was to compare the efficacy and safety associated with catheter-directed thrombolysis (CDT) using either recombinant tissue plasminogen activator (rt-PA) or urokinase (UK) for subacute deep venous thrombosis (DVT). From January 2014 to December 2016, we conducted a retrospective analysis on a total of 49 patients who underwent consistent CDT with either rt-PA (rt-PA-CDT group) or UK (UK-CDT group) treatment. The thrombolytic rate of the rt-PA-CDT group was significantly higher than that of the UK-CDT group (87.5% vs 60%, respectively; χ2 = 4.751; P = .029). The rt-PA-CDT group exhibited an improved grade III thrombolytic rate (9 patients vs 3 patients; χ2 = 5.144; P = .023). The time for the rt-PA-CDT group to achieve a grade III thrombolytic rate was shorter than that of the UK-CDT group (5.01 ± 1.09 days vs 6.43 ± 1.69 days, respectively; t = −2.187; P = .044). No severe complications were seen in either group and mild complications rates were 16.7% and 20.0% (χ2 = .091; P = .763). The clinical efficacy rates at discharge were 91.7% and 76.0%, respectively (χ2 = 2.200; P = .138). In conclusion, CDT with a continuous infusion of low-dose rt-PA resulted in safe and effective thrombolysis in the great majority of patients with proximal DVT in the subacute phase. Furthermore, rt-PA was significantly better than UK in terms of the thrombolytic rate. In our study, rt-PA-CDT improved the thrombolytic rate of grade III thrombus and achieved a grade III thrombolytic rate in a shorter time than UK-CDT.
Introduction
Deep vein thrombosis (DVT) of the inferior limbs, considered one of the most common vein diseases, results in pulmonary embolism (PE) associated with increased mortality and substantial morbidity and occurs when a blood clot forms in a leg vein. 1 Current guidelines recommend anticoagulant therapy as the standard treatment for DVT because of the lack of high-quality evidence for other treatments. 2 Although adequate anticoagulation can thin the blood to reduce further clots from forming and prevent PE, postthrombotic syndrome (PTS) can still develop, secondary to chronic insufficiency of the ipsilateral limb venous system. 3–4 Recent clinical studies have demonstrated that the use of thrombolysis for DVT can breakdown blood clots and has some advantages, such as earlier achievement of thrombus removal, resulting in lower rates of PTS compared to the use of oral anticoagulation alone. 4 –6 Therefore, thrombolysis has widely gained favor and has been rapidly applied in the endovascular treatment. 6
According to reports in the literature, 4,7 –9 the treatment of acute DVT by catheter-directed thrombolysis (CDT) with urokinase (UK) or alteplase (recombinant tissue plasminogen activator [rt-PA]) in combination with anticoagulation significantly improves the clearance and patency rates of acute DVT and reduces the incidence of postthrombosis syndrome. Clinically, according to the parameter of the start date of DVT symptoms, DVT can be categorized as acute phase (less than 14 days), subacute phase (15-28 days), and chronic phase (more than 28 days) by the reporting standards of the Society of Interventional Radiology (SIR). 10 Some patients who do not seek timely treatment or whose treatment is limited by their condition are already in the clinical subacute phase at the time they are admitted to the hospital.
To date, there is still no convincing clinical evidence in the current guidelines that any fibrinolytic agent is superior to others when CDT is used to treat the subacute phase of proximal DVT. Furthermore, the optimal fibrinolytic agent remains a matter of debate and is still a hot research topic in the treatment of venous thrombosis diseases. 11 Using a retrospective clinical data analysis, we compared the clinical efficacy of 2 fibrinolytic agents in CDT for patients in the subacute phase of proximal DVT to provide a reference for the clinical treatment of these patients.
Patients
This was a case series study, and the protocol was approved by the local institutional review board. All treated patients’ medical records were kept in the information system database for our referral. The information system database was searched for patients who conformed to the inclusion/exclusion criteria for case selection between January 2014 and December 2016. We retrospectively collected data on 24 patients in the subacute phase of DVT who underwent rt-PA thrombolysis treatment (rt-PA-CDT group) in our department from June 2015. For comparison with the efficacy of UK thrombolysis treatment, we collected data on 25 patients in the subacute phase of DVT who underwent UK thrombolysis treatment (UK-CDT group) between January 2014 and May 2015. The inclusion criteria for case selection were applied as follows: (1) patients with DVT who underwent continuous CDT treatment with UK or rt-PA in our department between January 2014 and December 2016; (2) patients who were clearly diagnosed with unilateral iliofemoral venous DVT and/or femoral–popliteal venous DVT involved by color Doppler ultrasonography and/or lower limb venography; (3) range of 15 to 28 days for the time between the onset of symptoms of the affected limb and(or) body signs and the treatment; and (4) a lack of symptoms and imaging evidence of PE. The exclusion criteria were as follows: (1) patients in the acute or chronic phase of DVT, (2) patients with bilateral lower limb DVT, (3) patients for whom the thrombolytic catheter could not be inserted into the thrombosis during CDT, and (4) patients who received auxiliary mechanical thrombectomy.
Procedures
A temporary filter was placed into the inferior vena cava (IVC) for patients with a massive thrombus in the proximal vein that was judged to be potentially life threatening at the discretion of the operator via the femoral vein of the nonaffected leg prior to the next step of treatment. 12 Depending on whether the popliteal vein of the affected limb was imaged and whether the patient could assume the prone position, either a retrograde puncture from the contralateral femoral vein or an anterograde puncture from the ipsilateral popliteal vein was made to perform the CDT. 13 A low-dose continuous thrombolytic mode with an intravenous infusion pump (ZNB-XD intelligent infusion pump; KellyMed Co, Ltd, Beijing, China) was used for the thrombolysis. 14 The details are as follows: rt-PA-CDT group: 500 mL of saline + 20 mg of alteplase (20mg/each; Boehringer Ingelheim, Ingelheim am Rhein, Germany), which was continuously pumped in through a thrombolytic catheter at a flow rate of 0.01 mg·kg−1.h−1; UK-CDT group: 500 mL of saline + 500 000 to 750 000 U of UK (250 000 U/each; Livzon Pharmaceutical Co, Ltd, Zhujiang, China), which was continuously pumped in through a thrombolytic catheter at a flow rate of 20 000 to 30 000 U/h. During CDT, a therapeutic low-molecular-weight heparin (LMWH) injection (4100 IU/each; Changshan Biochemical Pharmaceutical Co, Ltd, Shijiazhuang, China) was used for anticoagulation with a subcutaneous injection of 4100 IU/12 hours.
During CDT, routine monitoring of prothrombin time, international normalized ratio (INR), plasma fibrinogen (FIB) concentration, activated partial thromboplastin time, platelet count, and other indicators was performed everyday. When the FIB level was 1.0 to 1.5 g/L, the rate of drug administration was slowed down; when the FIB was <1.0 g/L, thrombolysis was temporarily paused. Every 36 to 48 hours or more often if necessary, lower limb venography was performed as a reexamination to evaluate the thrombolysis efficacy and to adjust and ensure that the effective segment of the thrombolytic catheter was continuously buried deeply in the thrombosis. When the following indications appeared, the thrombolysis was stopped 14 : (1) the swelling of the affected limb disappeared or significantly subsided, and the angiography confirmed that the thrombosis had disappeared, (2) the range of thrombolysis of 2 consecutive reexaminations did not show a change, (3) FIB < 0.1 g/L, or (4) complications occurred during the CDT process. For example, when minor bleeding events occurred, the drug administration was temporarily stopped, or the drug administration rate was slowed, and 24 hours later, according to the severity of the disease, the thrombolysis treatment was either stopped or continued; when major bleeding events occurred, thrombolysis was terminated. If the angiography reexamination showed that the residual stenosis rate was >50% after iliac vein thrombolysis, balloon (Muatang 8-12mm; Boston Scientific Co, Ltd, Marlborogugh, USA) expansion was performed. 15 If the residual stenosis rate was still >50% after expansion, then stent (Luminexx 12-14mm; C. R. Bard, Murray Hill, New Jersey) implantation was performed in the lesion segment. After stent implantation, if the angiography reexamination showed that the vascular wall was rough and the blood flow was relatively slow, then the thrombolytic catheter was left in, and the thrombolysis was continued for another 24 hours.
During hospitalization, LMWH was subcutaneously injected for 5 to 7 days and was then changed to oral administration of the anticoagulant. Oral administration of warfarin (2.5 mg/tablet; Sine Pharmaceutical Laboratories Co, Ltd, Shanghai, China) was overlapped with that of LMWH for 3 to 5 days, and the INR was controlled to values of 2.0 to 3.0 for 3 to 6 months. 16 Before discharge, both groups of patients underwent a reexamination via intravenous antegrade angiography of the affected limb and a discharge efficacy evaluation. After being discharged, the patients were advised to wear therapeutic pressure gradient elastic stockings 17 (ankle pressure was approximately 30-40 mm Hg; 1 mm Hg = 0.133 kPa) for at least 2 years.
Outcomes and Safety
The main indicator was the thrombolytic rate, and the secondary indicator was improvement in the patient’s clinical symptoms. Three senior interventionists blindly assessed the thrombolysis degree of the affected limb based on the preoperative and postoperative venography images of the 2 groups: complete thrombolysis (grade III), revealing 100% thrombolysis with no residual clots; large degree of thrombolysis (grade II), revealing 50% to 99% thrombolysis; and small degree of thrombolysis (grade I), revealing <50% thrombolysis. Lysis grades II and III (ie, ≥50%) were considered successful lysis outcomes. 4,7 Clinical efficacy was assessed by considering the clinical symptoms, signs of the affected limb, and angiography images 13 as follows. Excellent indicates complete disappearance of swelling and pain of the affected limb; when the ipsilateral side was compared to the contralateral side, the difference in the circumference was ≤1.0 cm, and angiography showed that the blood flow was completely or essentially recovered with no visible retention of the contrast agent. Good indicates complete disappearance of swelling and pain of the affected limb; when the ipsilateral side was compared to the contralateral side, the difference in the circumference was >1.0 to ≤1.5 cm, and angiography showed that most of the blood flow was recovered with no obvious retention of the contrast agent and a small number of collateral vessels. Fair indicates there was a significant improvement in swelling and pain of the affected limb; when the ipsilateral side was compared to the contralateral side, the difference in the circumference was >1.5 to ≤2.0 cm, and angiography showed that the blood flow was partially recovered with slight retention of the contrast agent and more collateral vessels. Poor indicates there was no significant improvement in the swelling and pain of the affected limb; when the ipsilateral side was compared to the contralateral side, the difference in the circumference was >2.0 cm, and the angiography showed that there was significant retention in contrast agent and a large number of collateral vessels for compensation. The effective rate of clinical efficacy = (the number of [excellent + good + fair] cases/total number of cases) × 100%.
At follow-up, PTS was diagnosed after 12 months based on the Villalta scale, with assessment of 5 patient-rated venous symptoms and 6 clinician-rated physical signs. A score of 5 or higher represented PTS, and a score of 15 or greater or the presence of venous ulcer represented severe PTS. 3,4
The related complications that occurred during CDT included major complications, such as a decrease in hemoglobin 2 g/dL, which required transfusion of at least 2 U of packed red blood cells, an intracranial hemorrhage or massive hemorrhage of other important organs, PE or death, and minor complications, such as oozing of blood and hematoma at the puncture site, hematuria visible to the naked eye or under a microscope, mucosal bleeding, and other small bleeding events and infections, which could be controlled by simple suppression or stopping the thrombolysis. 4
Statistical Analysis
The SPSS statistical package (version 23.0, SPSS, Chicago, Illinois) was used for all statistical analyses in this study. The measurement data with normal distribution are represented by the means ± standard deviation (SD). Comparison of the measurement data of the 2 groups of patients was performed with a t test. Comparison of the count data of the 2 groups was performed with Fisher exact test/χ2 test. A t test was used for the comparison of the average thrombolysis time between the rt-PA-CDT group and the UK-CDT group. P < .05 was considered statistically significant.
Results
Baseline Demographics and Clinical Characteristics
The general clinical characteristics of patients in the 2 groups are detailed in Table 1. None of the differences were statistically significant (all P > .05), and they were comparable.
Baseline Demographics of the Patients.a
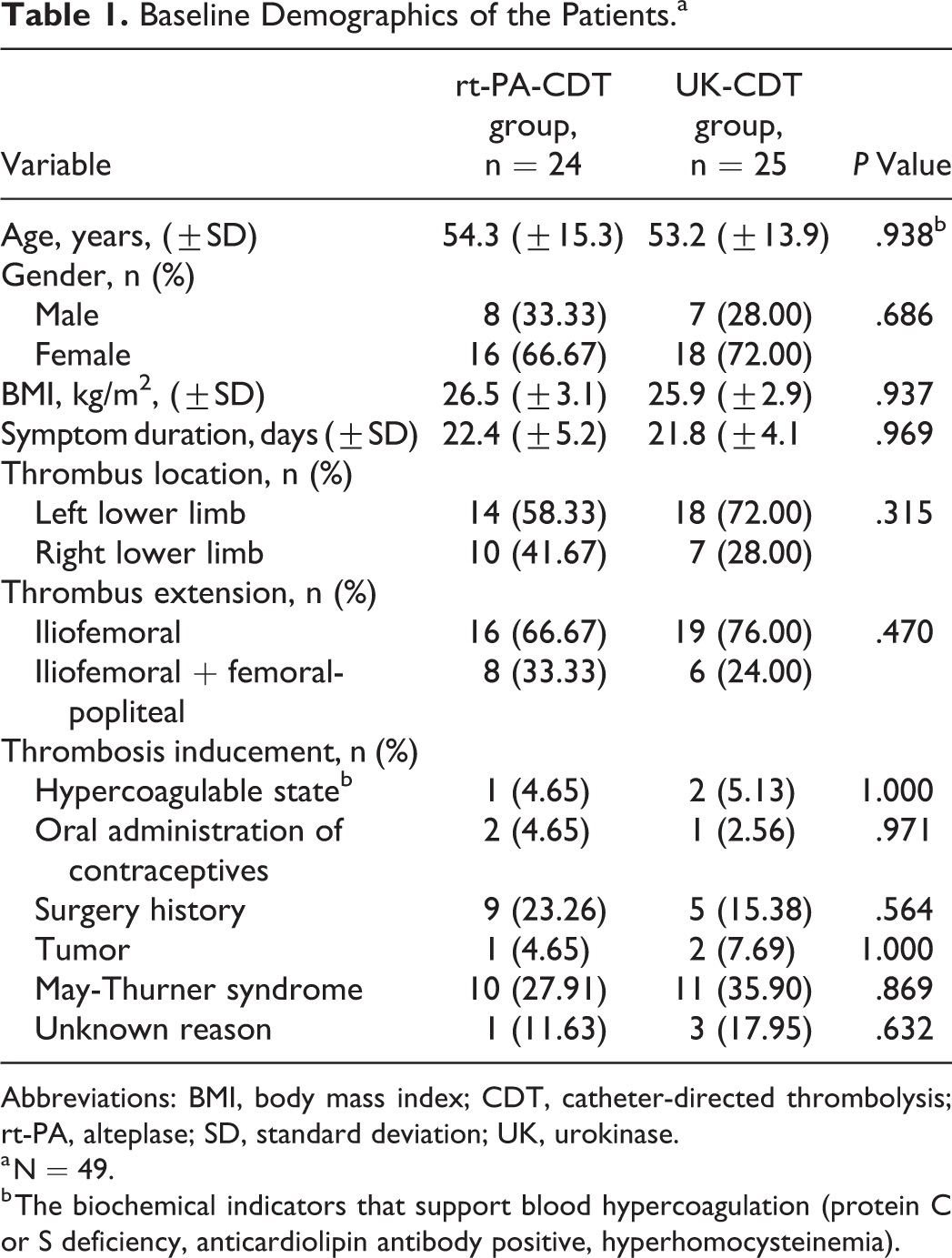
Abbreviations: BMI, body mass index; CDT, catheter-directed thrombolysis; rt-PA, alteplase; SD, standard deviation; UK, urokinase.
a N = 49.
b The biochemical indicators that support blood hypercoagulation (protein C or S deficiency, anticardiolipin antibody positive, hyperhomocysteinemia).
Endovascular Therapeutic Strategies, Thrombolytic Rate, and Clinical Efficacy
A total of 17 patients (10 in the rt-PA-CDT group and 7 in the UK-CDT group; χ2 = 1.009; P = .315) who were evaluated as potentially life-threatening received recoverable IVC filters prior to interventional treatment. All filters were removed after CDT treatment.
The thrombolysis degree, average CDT time, and dose of thrombolytic agents of the rt-PA-CDT and UK-CDT groups are shown in Table 2. The thrombolytic rate of the rt-PA-CDT group (≥50%) was significantly higher than that of the UK-CDT group, and the difference was statistically significant (χ2 = 4.751; P = .029). The rt-PA-CDT group exhibited an improved grade III thrombolytic rate (χ2 = 5.144; P = .023). The total average CDT time was 5.6 ± 1.0 days for the rt-PA-CDT group and 6.3 ± 1.5 days for the UK-CDT group, and the difference was not statistically significant (t = −1.868, P = .194). The time for the rt-PA-CDT group to achieve a grade III thrombolytic rate was significantly shorter than that for the UK-CDT group, and the difference was statistically significant (t = −2.187; P = .044). The difference in time to achieve a grade I or II thrombolytic rate between the 2 groups was not statistically significant (t = 0.304 and −0.627, respectively; P > .05). When the thrombolytic rate was >50%, the total dose of thrombolytic agent in the rt-PA-CDT group was 20.0 to 100.0 mg, with an average of 41.3 ± 9.8 mg, and the dose of the thrombolytic agent in the UK-CDT group was 3 000 000 to 6 000 000 U, with an average of 4 280 000 ± 839 000 U.
Comparison of the CDT Time, Dose of Thrombolytic Agent, and Degree of Thrombolysis Between the rt-PA-CDT and the UK-CDT Groups.a,b,c
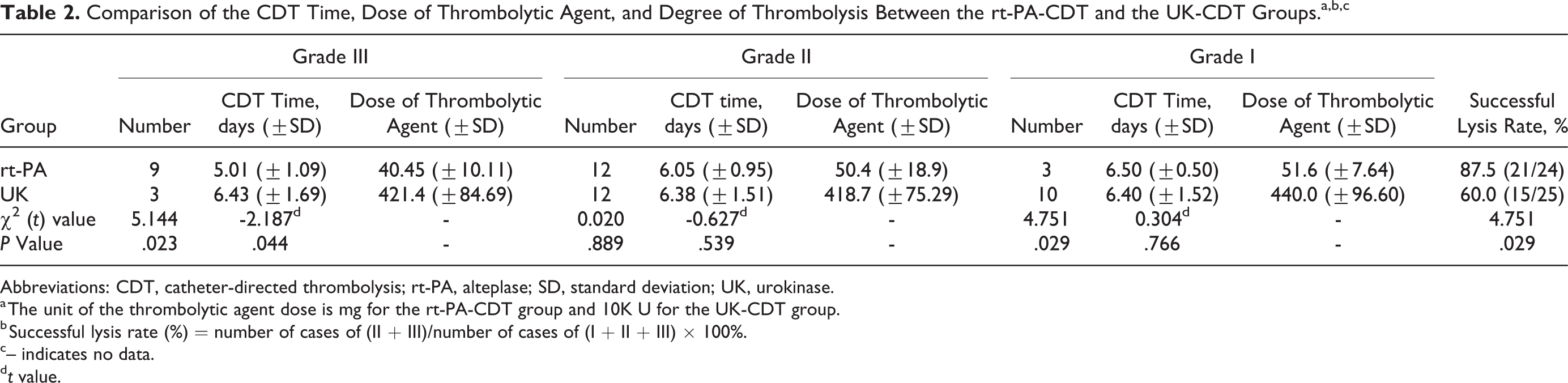
Abbreviations: CDT, catheter-directed thrombolysis; rt-PA, alteplase; SD, standard deviation; UK, urokinase.
a The unit of the thrombolytic agent dose is mg for the rt-PA-CDT group and 10K U for the UK-CDT group.
b Successful lysis rate (%) = number of cases of (II + III)/number of cases of (I + II + III) × 100%.
c– indicates no data.
dt value.
At the time of discharge, the clinical efficacy rates were high in both the groups, and the difference in the clinical efficacy rate between the rt-PA-CDT and the UK-CDT groups was not statistically significant (χ2 = 2.200; P = .138; Table 3). However, the blood flow in the iliofemoral main trunk of the rt-PA-CDT group was good, and the blood flow of the iliofemoral main trunk of the UK-CDT group was worse than that of the rt-PA-CDT group, although the blood flow of adjacent collateral vessels was increased. The rt-PA-CDT and UK-CDT groups had 16 (66.7%) patients and 13 (52.0%) patients, respectively, whose residual stenosis was >50% after venous thrombolysis; these patients underwent PTA treatment (χ2 = 1.090; P = .296). There were 14 (58.3%) patients and 12 (48.0%) patients in the rt-PA-CDT and UK-CDT groups, respectively, who underwent adjunctive treatment with stent placement (χ2 = .525; P = .469).
Comparison of the Clinical Efficacy and Complications in the 2 Groups.a
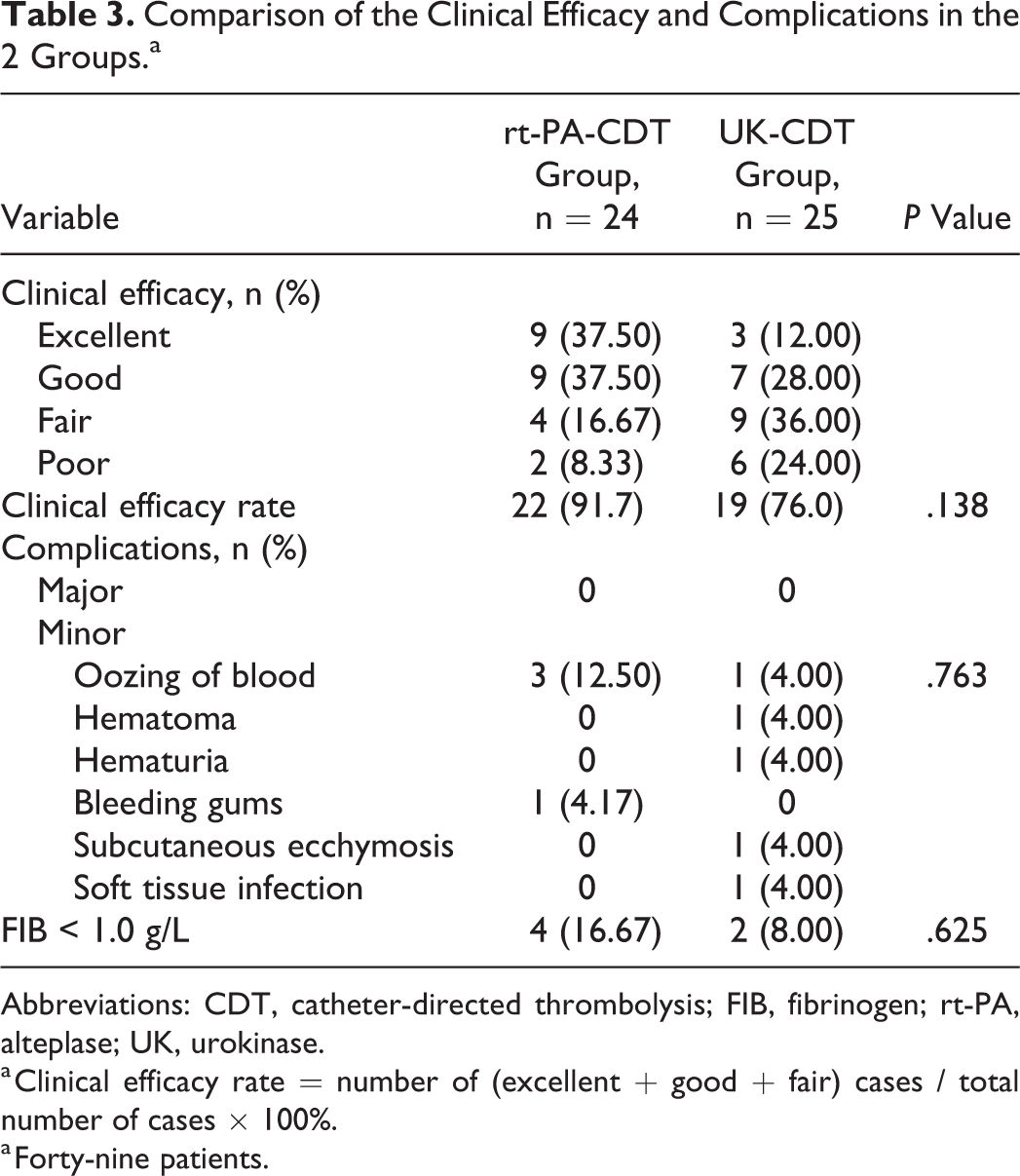
Abbreviations: CDT, catheter-directed thrombolysis; FIB, fibrinogen; rt-PA, alteplase; UK, urokinase.
a Clinical efficacy rate = number of (excellent + good + fair) cases / total number of cases × 100%.
a Forty-nine patients.
Safety Comparison
There were no serious complications in the rt-PA-CDT and UK-CDT groups. The incidence rates of minor bleeding complications were 16.7% and 20.0%, respectively, and the difference was not statistically significant (χ2 = 0.091, P = .763). In the UK-CDT group, 1 patient had an inflammatory manifestation in the soft tissue around the puncture site after undergoing CDT for 10 days (Table 3). In the rt-PA-CDT group, during CDT, the FIB of 4 patients was lower than 1.0 g/L. For 3 of these cases, 24 hours after the thrombolysis was stopped, the FIB was increased to 1.0 g/L during the reexamination, and 1 patient required transfusion with cryoprecipitated antihemophilic factors. Among the patients in the UK-CDT group, during CDT, the FIB of 2 patients was lower than 1.0 g/L. A total of 24 hours after the thrombolysis was stopped, the FIB of 1 patient increased to above 1.0 g/L during the reexamination, and 1 patient underwent transfusion of cryoprecipitated antihemophilic factors. The difference between the 2 groups was not statistically significant (χ2 = 0.239, P = .625).
Discussion
At present, there are differences in the clinical staging of DVT in various research institutions and guidelines. 6 –10 The staging is largely determined based on the onset time of the patient’s clinical symptoms and the examination results of ultrasonography and/or digital subtraction angiography (DSA), 10 which may cause inaccuracy in the staging of DVT and in the evaluations of efficacy and prognosis. Although it is more scientifically sound and instructive to determine the stage of DVT according to the age of thrombus, at present, the determination of the age of thrombus is still in the exploratory stage. Therefore, in this study, when determining the subacute stage, we still adopted the SIR reporting standard. 10 For acute-stage proximal DVT, the use of CDT treatment has been recognized by scholars both in China and abroad, and its efficacy has been confirmed to be significantly superior to that of simple anticoagulation treatment. 5,6 Compared to simple anticoagulation, thrombolysis treatment for patients with subacute proximal DVT may be a positive and effective strategic choice. 18 However, the selection of the thrombolytic agent is mainly empirical, and it has rarely been reported whether there is any difference in clinical efficacy between agents in the treatment of subacute proximal DVT.
The clinical control studies by Sugimoto et al 8 and Grunwald et al 9 directly compared the safety and clinical efficacy of UK and rt-PA in the treatment of DVT. The time between the onset and treatment of the included participants was less than 3 months. The efficacy of thrombolysis is related not only to the type of fibrinolytic agent but also to the dosage of the drug, perfusion duration, and other factors. In the studies by Sugimoto et al 8 and Grunwald et al, 9 the drug administration rate, drug administration time, and dose of thrombolytic agent were 113 000 to 150 000 U/h, 33.4 to 40.6 hours, and 440 to 480 million U in the UK-CDT group, respectively, and 0.57 to 0.96 mg/h, 24.1 to 30.8 hours, and 21.6 to 23.2 mg in the rt-PA-CDT group, respectively. Upon the completion of thrombolysis, the thrombolytic rates (≥50%) were 83.4% to 97.4% in the UK-CDT group and 87.5% to 96.9% in the rt-PA-CDT group, respectively, and both groups could achieve the goal of a better unobstructed vascular vessel, with rt-PA significantly reducing the thrombolysis time. Therefore, the authors suggested that the thrombolytic rates of both thrombolytic agents were comparable. However, in these 2 studies, the time ranges between the appearance of clinical symptoms and the treatment were wide, and patients with nonacute-phase DVT only accounted for 33% of the total number, making it very difficult to objectively reflect the efficacy of the rt-PA and UK thrombolysis treatments of nonacute phase thrombus. In this study, patients in the clinical subacute phase were included. For cases in which the duration of continuous infusion of the thrombolytic agent in the rt-PA-CDT group and UK-CDT group was comparable, the 87.5% thrombolytic rate (≥50%) of the rt-PA-CDT group was significantly higher than the 60.0% rate of the UK-CDT group (P = .029), and rt-PA could achieve grade III thrombolysis in a shorter time compared to UK. This finding suggests that rt-PA is superior to UK for thrombolysis in subacute proximal DVT. This result is related to the retention of the 2 circular structures (K region: ligand binding site) in its molecular structure, allowing rt-PA to selectively bind in a targeted manner to a specific site on a surface lysine and thus specifically activate FIB in a local area of the thrombus, thereby providing the pharmacological property of selective infiltration thrombolysis that occurs from the outside to the inside and layer by layer. 19
At present, the methods used by different research institutions for the treatment of nonacute DVT are different. 20 In this study, CDT with rt-PA and UK both had significant clinical efficiency, and at discharge, there was no significant difference in the clinical efficacy rate between the 2 groups (P = .138). This finding was attributed to the positive correlation between the improvement in clinical symptoms and thrombolytic rate and the correlation with the timely opening of collateral vessels and other factors. However, at the 12-month follow-up, there was no difference in PTS (P = .610). The studies by Haig et al 4 and Mewissen et al 7 showed that the grades II and III thrombolytic rates were significantly better than that of grade I in improving the vascular patency rate and reducing the recurrence rate of thrombus and the incidence of PTS. Thus, the degree of thrombolysis is positively proportional to the improvement in the long-term quality of life of the patient. 21 In this study, the thrombolytic rate (≥50%) of the rt-PA-CDT group was 87.5%, which is significantly better than the 60.0% rate of the UK-CDT group. Thus, we predict that the rt-PA-CDT group may have a lower incidence of PTS and better prognosis than the UK-CDT group in the long-term efficacy, but this still requires further follow-up and observation. At present, in Asian countries, relevant physicians are already familiar with the dosage, time, safety, and efficacy of UK for the treatment of DVT, but the application of rt-PA is relatively lacking. In this study, we determined the grades II and III thrombolytic rates and the dose of the thrombolytic agent and suggest that the thrombolytic effect (thrombolytic rate) of 1 mg of rt-PA is equivalent to the thrombolytic effect of 100 000 to 150 000 U of UK. We hope that this information can be a reference when rt-PA is used for the first time in CDT to treat DVT, and the dose of rt-PA can be controlled to prevent large dose-dependent bleeding complications from occurring.
In the study by Haig et al, 4 the administration rate of rt-PA was 0.01 mg·kg−1.h−1, and the incidence of major complications (massive bleeding) was 11%. In the study by Mewissen et al, 7 the average UK administration rate was 146 000 U/h, and the incidence of major complications was 3.3%. Thus, when rt-PA thrombolysis is highly beneficial, the risk of major complications may be higher than that for UK. In this study, we used a low dose and continuous thrombolysis, and no major bleeding, symptomatic PE, or other severe complications were observed during thrombolysis, which is different from the results of Haig et al 4 and Mewissen et al. 7 This finding may be related to the selection of patients, individual differences, the prescription plan, the infusion duration, and many other factors. 7,13 In this study, the incidence of minor bleeding complications was not significantly different between the 2 groups (P = .763) and was similar to the minor bleeding incidence rates of 21.7% and 16% reported by Haig et al 4 and Mewissen et al. 7 Thus, we consider the treatment of subacute DVT by low-dose, continuous rt-PA and UK through CDT to be safe, as neither agents increased the risk of bleeding. In this study, rt-PA rapidly reduced FIB but did not increase the risk of bleeding compared to UK. This result is related to the pharmacological property that rt-PA has a relatively small impact on systemic fibrinolysis and coagulation systems when it generates a thrombolytic effect. 19
This study still has some limitations. (1) The DVT staging was mainly based on the onset time of clinical symptoms and the imaging data of ultrasonography and (or) DSA, and there may be chronic patients whose clinical symptoms were delayed. Staging determined strictly according to the age of thrombus may be more scientifically sound and rigorous. (2) The grouping was not random and was mainly based on the order of the use of thrombolytic agents in our department, which may cause errors in evaluating the efficacy of DVT. (3) This was a single-center, retrospective, nonrandomized controlled study; the conclusions of the present study are limited as a result of the small, retrospective nature of the analysis. In the future, a prospective, randomized controlled study will be needed to further confirm the conclusions.
In summary, CDT with a continuous infusion of low-dose rt-PA resulted in safe and effective thrombolysis in the great majority of patients with proximal DVT in the subacute phase. The rt-PA agent is significantly better than UK in terms of the thrombolytic rate (≥50%), rt-PA-CDT improves the thrombolytic rate of grade III thrombus, and rt-PA-CDT can achieve a grade III thrombolytic rate in a shorter time. This finding may support the selection of rt-PA-CDT thrombolysis treatment as a positive and effective strategy for well-selected patients with subacute proximal DVT who have no contraindications to thrombolysis and a lower bleeding risk.
Footnotes
Compliance With Ethical Standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Authors’ Note
The scientific guarantor of this publication is Prof. JianPing Gu. The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article. The content of the manuscript is original, and it has not been published or accepted for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Clinical Medicine Science and Technology Projects of Jiangsu Province, China (BL2014013) and the Nanjing Medical Science Fund, China (YKK14087).