
Abstract
Race is touted as an independent risk factor for venous thromboembolism (VTE), although the basis for this is varied and contentious. Comparison of plasma thrombin generation (TG) using calibrated automated thrombogram (CAT) across races offers a modality that objectively measures global hemostatic function to evaluate this influence. Direct comparative data across races are currently not available. Aim is to establish the influence of race on plasma TG. Sixty normal participants, matched for age and gender, equally representing 4 races—Caucasian, Chinese, Indian, and Malay—were recruited. Thrombin generation parameters (lag time, time to peak, peak, and endogenous thrombin potential [ETP]) in platelet-poor plasma were measured using CAT. The mean ETP (standard deviation) for the different races were Caucasians: 1338.18 (194.19) nM·min; Chinese, 1318.91 (108.90) nM·min; Indians, 1389.81 (182.61) nM·min; and Malays, 1436.21 (184.24) nM·min. Caucasians had the longest mean lag time of 2.59 ± 0.37 seconds; Indians had the highest mean peak of 284.22 ± 30.74 nM, and Malays had the longest mean time to peak of 5.47 ± 0.59 seconds. Analysis based on race did not demonstrate any significant difference for all TG parameters. The greatest mean difference of ETP between any 2 races (Malays and Chinese) was 117.30 nM·min (95% confidence interval: −45.86 to 280.46 nM·min) which was within the predefined limit of equivalence. In a cohort of healthy participants, TG mediated by plasma factors is not influenced by race and does not explain the reported racial differences in VTE incidence. For the 4 racial groups studied, the use of separate normal ranges for plasma TG might not be essential.
Introduction
Thrombin generation (TG) assay measures the potential hemostatic function of blood, which is determined by the overall balance of prothrombin activation and thrombin inactivation. The calibrated automated thrombogram (CAT) is a technique developed to measure the capacity of an individual to generate thrombin by analyzing several variables including the lag time, the peak amount of thrombin generated, and its corresponding time, as well as the endogenous thrombin potential (ETP) given by the area under the curve. This information may then be used to give an indication of the potential risks of bleeding or thrombosis. 1 It is therefore an assessment of global hemostatic function that is not usually assessed by routine conventional coagulation tests.
The relative ease and increasingly widespread availability of the CAT platform has opened up a new dimension in the assessment of coagulation disorders. Data generated using CAT on normal participants and those with various hemostatic disorders are now widely available but are usually confined to specific racial groups prevalent to the location of the study. Race is, however, a contentious contributor to differences in hemostatic capacity. Population studies have mostly supported higher rates of venous thrombosis among Caucasians and blacks compared to Asians. 2 –4 In a previous study conducted in Singapore, incidence of venous thromboembolism (VTE) varied among the Chinese, Indian, Malay, and Caucasian patients. 4 Similarly, laboratory measures of various plasma hemostatic factors, including factor VII, VIII, protein C, and protein S have also touted racial differences in plasma levels. 2,3,5 –7 Comparison of plasma TG using CAT across different racial groups, therefore, offers an attractive modality that objectively measures global hemostatic function to weigh in on the subject of the influence of race on thrombotic events.
Although CAT data on normal participants from a few racial groups are now available, standardization of preanalytical variables is currently lacking. The resultant wide interlaboratory variability of TG data renders direct interlaboratory comparison of TG parameters invalid. 8,9 Therefore, the question of whether there are racial differences in TG potential mediated by plasma factors in a normal healthy population is currently not answered. We hypothesized that ETP, as a measurement of the total amount of thrombin generated and hence a function for hyper- or hypocoagulability, would show a clinically significant difference (predefined as at least 300 nM·min difference in ETP) between any 2 major races in Singapore. To address this, we conducted a study to measure plasma TG in our local diverse population with a cohort of volunteers from different racial groups, controlling for age and gender. This article reports our findings.
Methods
Normal healthy participants were recruited between March 2014 and May 2016. This study is approved by our institutional research review board. Fifteen participants from 4 racial groups (Caucasian, Chinese, Indian, and Malay) were recruited and matched for age and gender. Participants who were pregnant, had a history of thrombotic or bleeding disorders, and on antiplatelet, anticoagulants, oral contraceptives, or hormonal therapy were excluded.
Blood sampling and plasma preparation were performed according to the manufacturer’s recommendations. In brief, blood samples from the healthy participants were collected into vacuum tubes (Becton Dickinson, Franklin Lakes, New Jersey) containing 0.109 M sodium citrate as an anticoagulant at a proportion of 9:1 (blood:anticoagulant) using 21G needle without tubing after obtaining informed consent. The first blood sample collected from each patient was not used for TG. Whole blood samples were centrifuged at 1500g for 15 minutes (Hettich, Tuttlingen, Germany), followed by 10 minutes at 10 000g to obtain the platelet-free plasma. The plasma was quick-frozen and stored at −80°C until tested, not later than 6 months in batches after blood collection. Samples were analyzed immediately after thawing for 10 minutes at 37°C. Thrombin generation was analyzed using the Calibrated Automated Thrombogram (Diagnostica Stago, S.A.S, Paris, France) system. The CAT assay is measured using a prewarmed fluorometer (Fluoroskan Ascent; Thermo Scientific, Waltham, Massachusetts). In a 96-well round bottom plate, 20 μL of prewarmed trigger solution (a mixture of 5 pM phospholipid and 4 μM tissue factor) calibrated for platelet-poor plasma (PPP) was added to 1 well and 20 μL of prewarmed calibrator containing 600 nM α2M thrombin complex to another well. A 80-μL plasma was then added to each of the wells. Twenty microliters of a solution containing calcium and a fluorogenic substrate (FluCa solution; Diagnostica Stago, S.A.S) were added automatically by a dispenser at 0 time to each well, and readings were recorded at 30-second intervals for at least 40 minutes. Each sample was run in triplicate. Calibrated automated thrombogram parameters generated were (1) lag time (minutes): the initiation phase of clotting which equals to the clotting time; (2) peak height (nM): the maximal amount of thrombin formed; (3) ETP (nM·min): the area under the curve representing TG and decay over time; and (4) time to peak (minutes): the time needed to achieve the peak height.
Epidemiological data including gender, age, and race of the participants were recorded. Based on our previous data from 145 unselected normal participants, the mean ETP was 1329.2 (164.9) nM·min. With this knowledge, a clinically significant difference in ETP between any 2 racial groups was predefined as within 300 nM·min (approximately twice that of the standard deviation of normal controls). With a sample size of 15 for each racial group, this study would have an 80% power and 2-sided α of 5% to show equivalence. Basic descriptive statistics were computed to report the demographics of the study population. Mixed model with group matched as a random effect to account for age and gender was performed to analyze the effect of race on the TG parameters. Pairwise comparisons of the various racial groups were performed with Bonferroni correction. All statistical analyses were performed using SPSS version 23 (IBM Corporation, New York).
Results
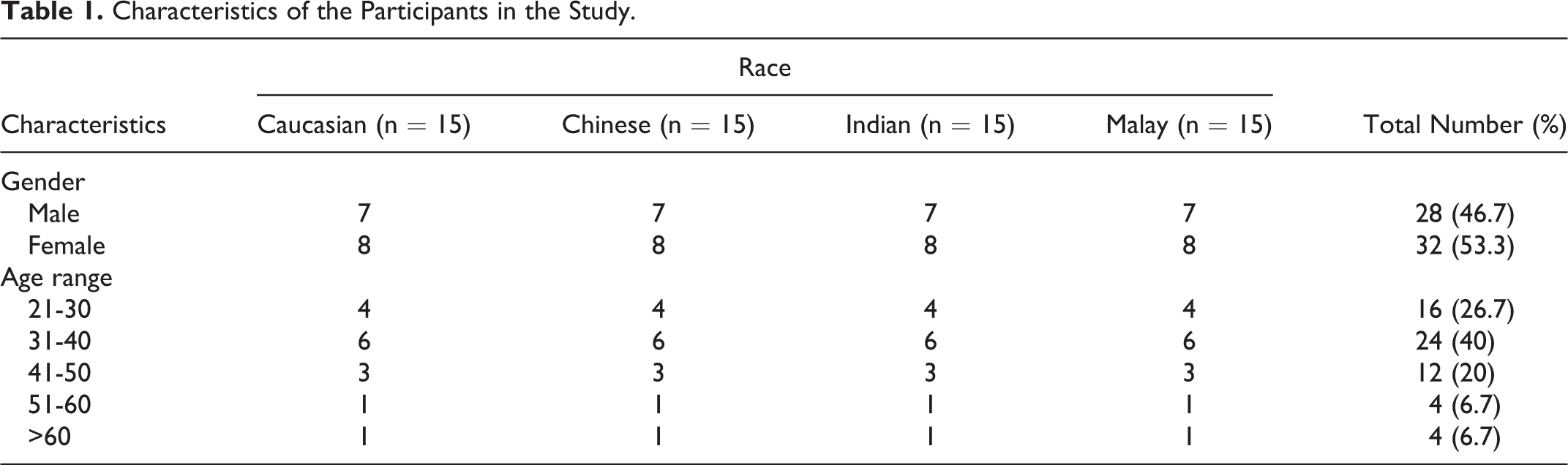
Sixty participants were recruited in our study and equally distributed across the 4 racial groups in our population (Caucasian, Chinese, Indian, and Malay), with ages ranging from 22 to 72 (Table 1). Participants from each racial group were matched for age and gender. Majority of the participants were younger than 50 years (86.7%). There were 28 (46.7%) male participants in the cohort. Plasma TG assay was performed in our laboratory with average interassay coefficient of variation (CV) of 12.4% and intra-assay CV of 1.45% for all parameters. The overall and race-specific TG parameters obtained from our study are shown in Table 2.
Characteristics of the Participants in the Study.
Thrombin Generation Parameters of the Participants.
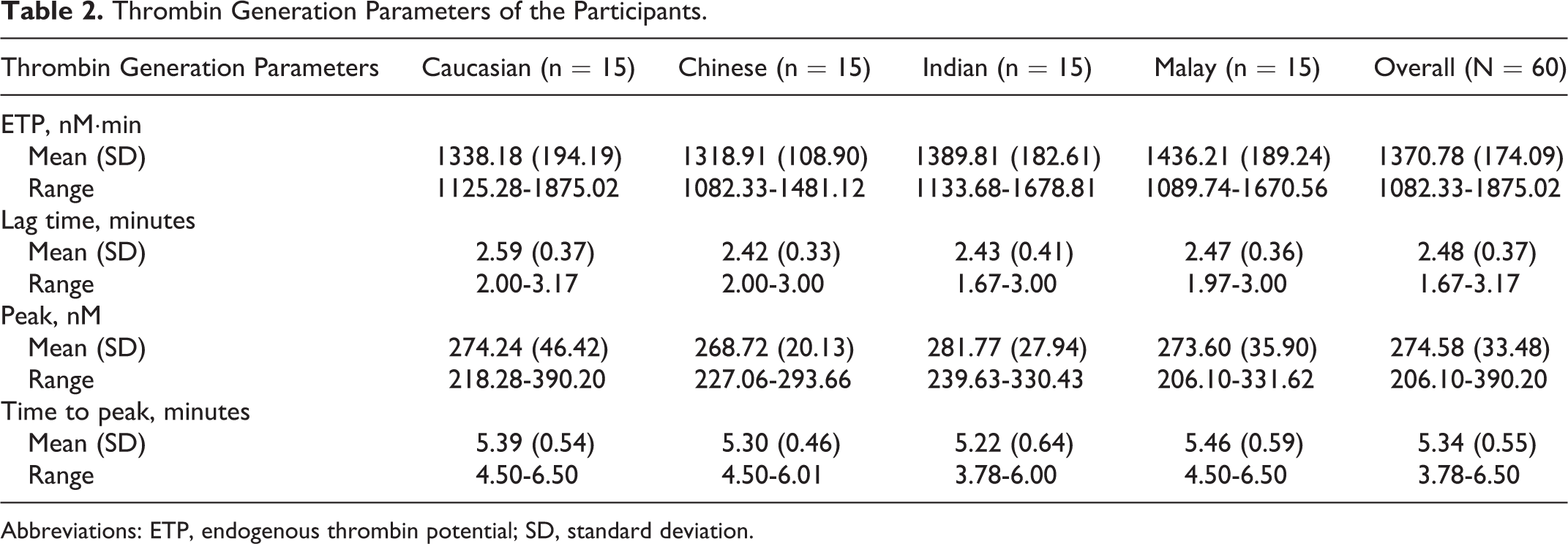
Abbreviations: ETP, endogenous thrombin potential; SD, standard deviation.
As age and gender may affect TG, 10,11 these variables were controlled by using age- and gender-matched participants of different races to eliminate these potential confounders. Pairwise comparisons between racial groups with Bonferroni correction revealed no significant differences in all 4 plasma TG parameters (P value > .05).
The Malay participants had the highest mean ETP, followed by the Indian, Caucasian, and Chinese participants. Nonetheless, the mean difference of ETP between the Malay and Chinese participants was only 117.30 nM·min, with the lower and upper bounds of the 95% confidence interval for difference between the 2 groups falling (Table 3) within the predefined limit of clinically relevant difference that the study intended to evaluate.
Pairwise Comparisons of the Participants’ ETP.
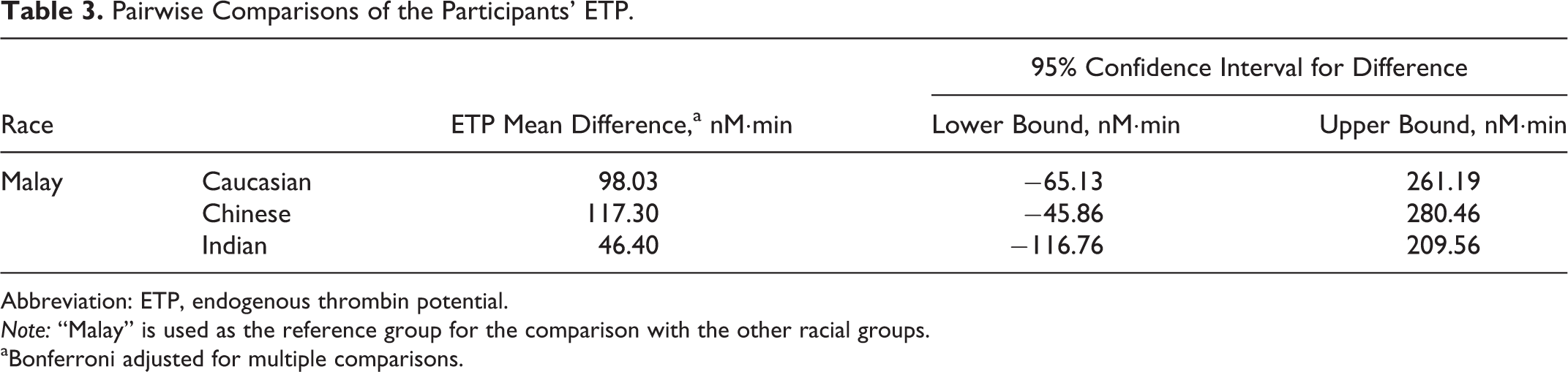
Abbreviation: ETP, endogenous thrombin potential. Note: “Malay” is used as the reference group for the comparison with the other racial groups.
aBonferroni adjusted for multiple comparisons.
There was no consistent trend in the various plasma TG parameters measured across the different racial groups. The Caucasian participants have the longest mean lag time, Indian participants had the highest mean peak, and Malay participants had the longest mean time to peak apart from the highest mean ETP. On the other hand, Chinese participants had the shortest mean lag time and the lowest mean peak, whereas the Indian participants had the shortest mean time to peak. Interestingly, the Caucasian participant who generated the highest ETP also had the highest peak, which is not unexpected; this was, however, an isolated finding and did not extend to the rest of the cohort.
Discussion
While data generated using CAT on normal participants and those with various hemostatic disorders are now widely available, information on the influence of race on the TG parameters remains lacking. This study reports our attempt at defining this connection.
Measurement of plasma TG, being the penultimate step before clot formation, is thought to be able to amalgamate the effects of various coagulation and platelet parameters responsible for the delicate balance in normal hemostatic homeostasis. Thrombin generation performed on platelet-free plasma provides focus on the plasma factors responsible for TG. Known and measurable factors such as clotting factors and the natural anticoagulants have reported differences in normal plasma levels defined across races as well as prevalence of pathologically abnormal levels. 2,5 –7,12,13 This has been cited as potential reasons for racial differences in incidence of venous and perhaps arterial thrombotic events. Our findings, however, suggest that, in healthy Caucasian, Chinese, Indian, and Malay participants, TG parameters contributed by plasma factors are not predetermined by race.
We also compared the plasma TG values obtained from our Chinese group with those from studies originating from China, which used the same CAT system and trigger concentrations of tissue factor and phospholipids. 14,15 The centrifugation conditions and the concentration of sodium citrate used in the blood collection tubes, however, differed from that used in our laboratory. Their plasma TG parameters were vastly different from ours, and this is likely due to differences in test methodology rather than the effects of potential confounders. This reaffirms the earlier contention that TG parameters performed at different laboratories cannot be used for indirect comparison. In contrast, our current study provides direct standardized comparison of plasma TG parameters across a number of racial groups.
One limitation in our study is the relatively small number of normal participants in each arm and the limited number of racial groups studied. Other acquired factors including diet, weight, and smoking that could potentially confound the influences of race were not controlled in this study. However, the direct effects of these factors on TG remain uncertain. Even though all the participants were not on antiplatelet, anticoagulants, oral contraceptives, and hormonal therapy, the use of other nonsteroidal anti-inflammatory drugs and traditional medications that could potentially interact with the coagulation system was not controlled and might be a potential source of confounder. Nonetheless, the standardized method of testing as well as our attempts to control for known confounders, specifically age and gender, should improve the validity of our findings and its conclusion.
Our results are important firstly for the establishment of normal values for all the TG parameters in multiracial populations. Based on our data, it might not be essential to use separate normal ranges for the different racial groups in populations sharing similar racial composition as in Singapore. Secondly, in a population of healthy participants, TG mediated by plasma factors might not be influenced by race and does not account for the reported racial differences in VTE incidence. If indeed race is an independent risk factor for thrombosis, plasma TG measurements is not a sensitive test for identifying this risk in healthy participants.
Footnotes
Acknowledgment
The authors thank all study participants for their participation in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is internally funded by the thrombosis and hemostasis research unit of Department of Hematology, Singapore General Hospital.