
Abstract
Monocyte to high-density lipoprotein cholesterol ratio (MHR) is a systemic inflammatory marker, and recently, it has been used quite commonly for the assessment of inflammation in cardiovascular disorders. The aim of the present study is to investigate the relevance of MHR as a marker to assess metabolic syndrome (MetS) and MetS severity in clinical practice. A total of 147 patients with MetS who were diagnosed according to National Cholesterol Education Program Adult Treatment Panel III criteria and 134 healthy controls, matched for age and gender, were included in our retrospective study. MHR values were 13.15 ± 6.07 for patients with MetS and 9.74 ± 5.24 for the control group. MHR values of the patients were found to be statistically significantly higher than the control group (P < .0001). MHR showed a significantly positive correlation with the severity of MetS (r = .429; P < .0001). When patients with MetS were assessed with MHR in the study population, receiver–operating characteristic curve analysis yielded a cutoff value of 9.36 with a sensitivity of 72%, a specificity of 61%, and a P value <.0001. In logistic regression analyses of MetS with several variables, MHR remained as an independent predictor of MetS (95% CI: 0.721-0.945, P = .005). MHR might be an available and useful inflammatory marker to evaluate patients with MetS and disease severity.
Introduction
Metabolic syndrome (MetS) is a disorder characterized with obesity, elevated blood pressure, impaired glucose metabolism, and atherogenic shifts in lipid metabolism that harbors genetic and environmental pathogenic factors. 1,2 In patients with MetS, increased incidence of nonalcoholic fatty liver disease and insulin resistance as well as physical inactivity have negative influence on the clinical course. 2 Although its etiopathogenesis is not fully defined, alterations and interactions of all those metabolic parameters lead to oxidative stress, endothelial dysfunction, and chronic low-grade inflammation, which consequently result in atherosclerosis and an increase in cardiovascular disorders due to atherosclerosis. 2,3
In patients with MetS, systemic inflammation has a significant role in the onset and progression of atherosclerotic process. In this inflammatory process, along with various other immune system elements, activation of monocytes and macrophages is predominant. 4,5 Monocytes, which account for 3% to 8% of leucocytes in peripheral blood, possess a key effect in control of inflammatory processes. Monocyte activation and its differentiation to lipid-loaded macrophages have important role in the formation of atherosclerotic lesions. 5 –8 High-density lipoprotein cholesterol (HDL-C) has a protective role in cardiovascular diseases due to its anti-inflammatory, antioxidant, and antithrombotic properties. 9 Besides, a relationship between high number of monocytes and low HDL-C levels has been reported in inflammatory disorders. Recently, monocyte to HDL-C ratio (MHR) has become a convenient marker in various cardiovascular disorders. 5,10 There are some advantages and disadvantages of MHR as a marker. It is cheaper than markers such as cytokines (interleukin [IL]-1, IL-6, tumor necrosis factor-α [TNF-α]), monocyte chemoattractant protein-1 (MCP-1), and serum amyloid A (SAA); it is an easily accessible marker that can be calculated by the ratio of monocyte and HDL-C, which is readily available in the lipid profile and the total blood count that we use in our daily clinical practice. However, it can be affected by anti-inflammatory and antilipidemic treatments that can be used in many systemic inflammatory or infection diseases. 5,11 –13 Our aim is to investigate the relevance of MHR as a marker to assess MetS and MetS severity in clinical practice.
Materials and Methods
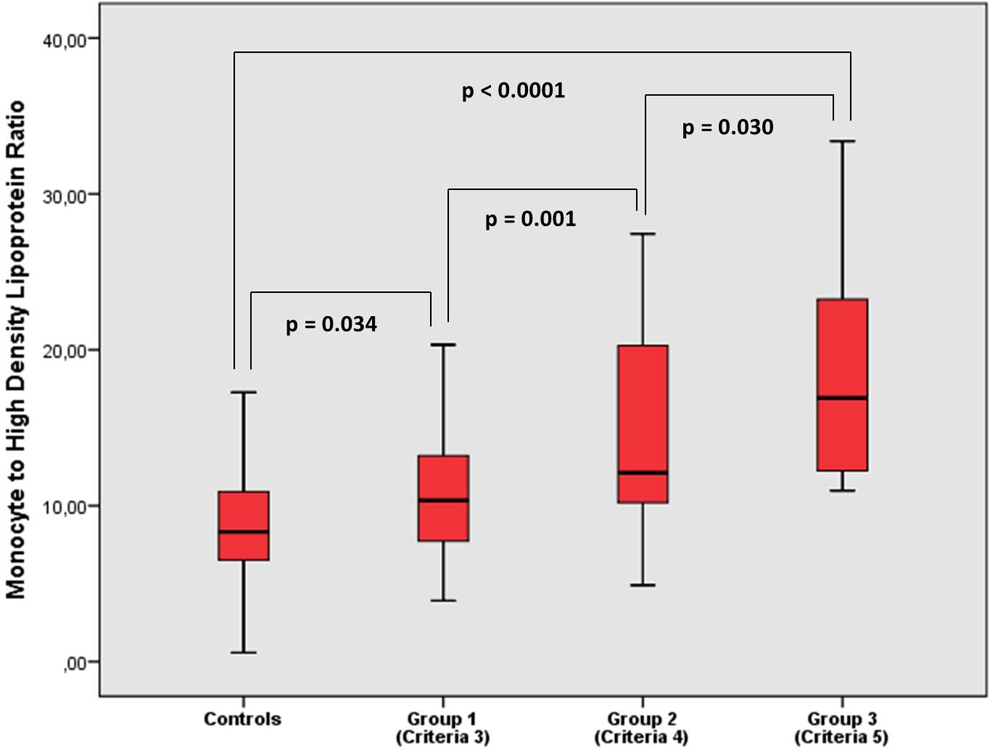
A total of 147 patients with MetS who were diagnosed according to National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) criteria 14 and 134 healthy controls, matched for age and gender, were included in our retrospective study. Basic clinical and laboratory parameters of patient and control groups were assessed and recorded. Patients were separated into 3 groups according to the NCEP ATP III criteria. Eighty-four patients with 3 criteria were placed into group 1, 44 patients with 4 criteria into group 2, and 19 patients with 5 criteria into group 3.
Metabolic syndrome was diagnosed according to the NCEP ATP III criteria. Those criteria required the presence of ≥3 of the following: Systolic blood pressure ≥130 mm Hg or diastolic blood pressure ≥85 mm Hg or treatment of previously diagnosed systemic hypertension. Fasting plasma glucose of ≥100 mg/dL or previously diagnosed type 2 diabetes mellitus. High-density lipoprotein cholesterol levels of <40 mg/dL in men and <50 mg/dL in women. Triglyceride (TG) levels ≥150 mg/dL or specific treatment for lipid abnormalities. Central obesity (waist circumference >102 cm for men and >88 cm for women).
Patients with anemia, B12 and folic acid deficiency, thyroid dysfunction, secondary hypertension, renal failure, hepatic failure, cardiovascular disease, asthma, chronic obstructive respiratory disease, acute and/or chronic infection, autoimmune disease, connective tissue disease, smoking history, alcohol consumption, cancer, and any use of medication (corticosteroids, nonsteroid anti-inflammatory drugs, antilipidemic, and immunosupressive agents) were excluded from the study. The ethics committee for Clinical Research of Anadolu University School of Medicine approved this study.
Laboratory Analysis
Venous blood samples of patient and control groups were taken after 12-hour fasting. Total cholesterol (TC), TG, and HDL-C values were analyzed with Abbott Architect C8000 system (Abbott diagnostics, USA) with original reagent. HDL-C was analyzed with direct enzymatic method without precipitation. Low-density lipoprotein cholesterol (LDL-C) was calculated using Friedewald formula (TC = LDL-C + HDL-C + TG/5). The complete blood count has been performed in the same analyzer, Sysmex XN-1000 (Sysmex Corporation, Kobe, Japan); standard tubes with constant amount of ethylenediaminetetraacetic acid have been used. Monocyte to HDL-C ratio was calculated manually.
Statistical Analysis
All statistical analyses were performed with the Statistical Package for the Social Sciences (SPSS) 15.0 software package (SPSS Inc, Chicago, Illinois). Descriptive statistics were presented as arithmetic mean (standard deviation). The significance of the mean differences between groups was assessed by Student t test and one-way analysis of variance (ANOVA). Differences were assessed by χ2 test for categorical variables. Relationships between variables were tested using Pearson correlation analysis. Receiver–operating characteristic (ROC) curve was used to demonstrate the ability to distinguish between control and clinical samples. The effect of various variables on MetS was analyzed with logistic regression analyses. P values of less than .05 were regarded as significant.
Results
No age and sex differences were observed between patients with MetS and control group (Table 1). MHR values were 13.15 ± 6.07 for patients with MetS and 9.74 ± 5.24 for the control group. MHR values of the patients were found to be statistically significantly higher than the control group (P < .0001; Table 1; Figure 1). Main clinical and laboratory characteristics of the patients and control group are shown in Table 1. Comparisons of MHR levels of group 1 (3 criteria), group 2 (4 criteria), group 3 (5 criteria), and control group showed statistically significant differences (11.15 ± 4.74, 14.73 ± 6.11, 18.52 ± 7.20, 9.74 ± 5.24, respectively; P < .0001; Figure 2). In correlation analysis, MHR showed a significantly positive correlation with the severity of MetS (r = .429, P < .0001; Table 2). All correlation analysis results are shown in Table 2.
The Clinical and Laboratory Parameters of patients with metabolic syndrome and controls.a
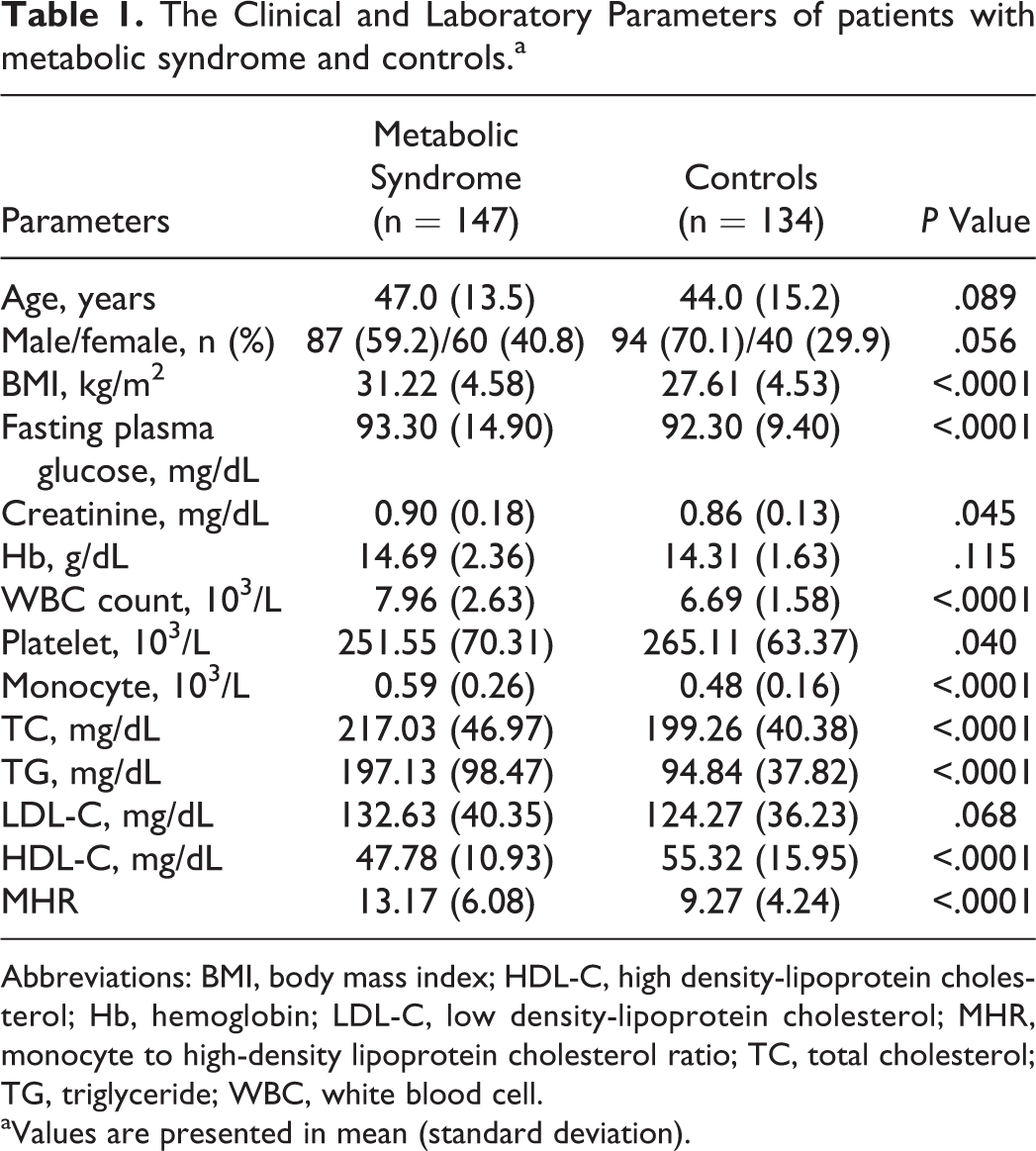
Abbreviations: BMI, body mass index; HDL-C, high density-lipoprotein cholesterol; Hb, hemoglobin; LDL-C, low density-lipoprotein cholesterol; MHR, monocyte to high-density lipoprotein cholesterol ratio; TC, total cholesterol; TG, triglyceride; WBC, white blood cell.
aValues are presented in mean (standard deviation).
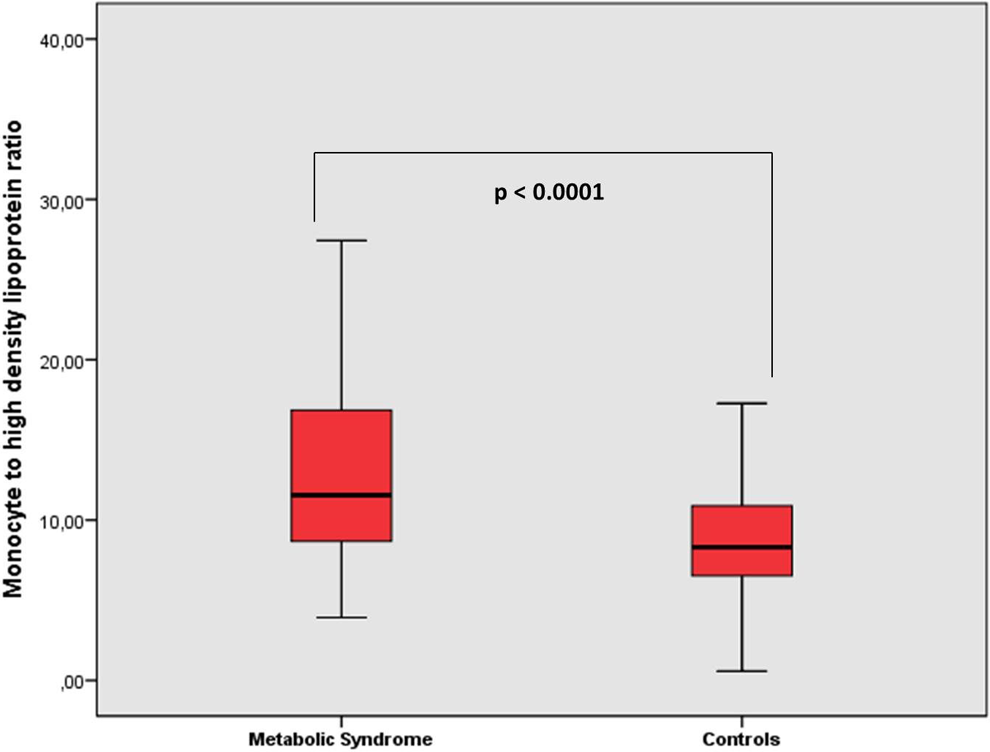
Monocyte to high-density lipoprotein cholesterol ratio was significantly higher in patients with metabolic syndrome than controls.
Comparison of monocyte to high-density lipoprotein cholesterol ratio values between patient with metabolic syndrome and controls.
MHR and Correlation Analysis of Other Parameters in Patients With Metabolic Syndrome.
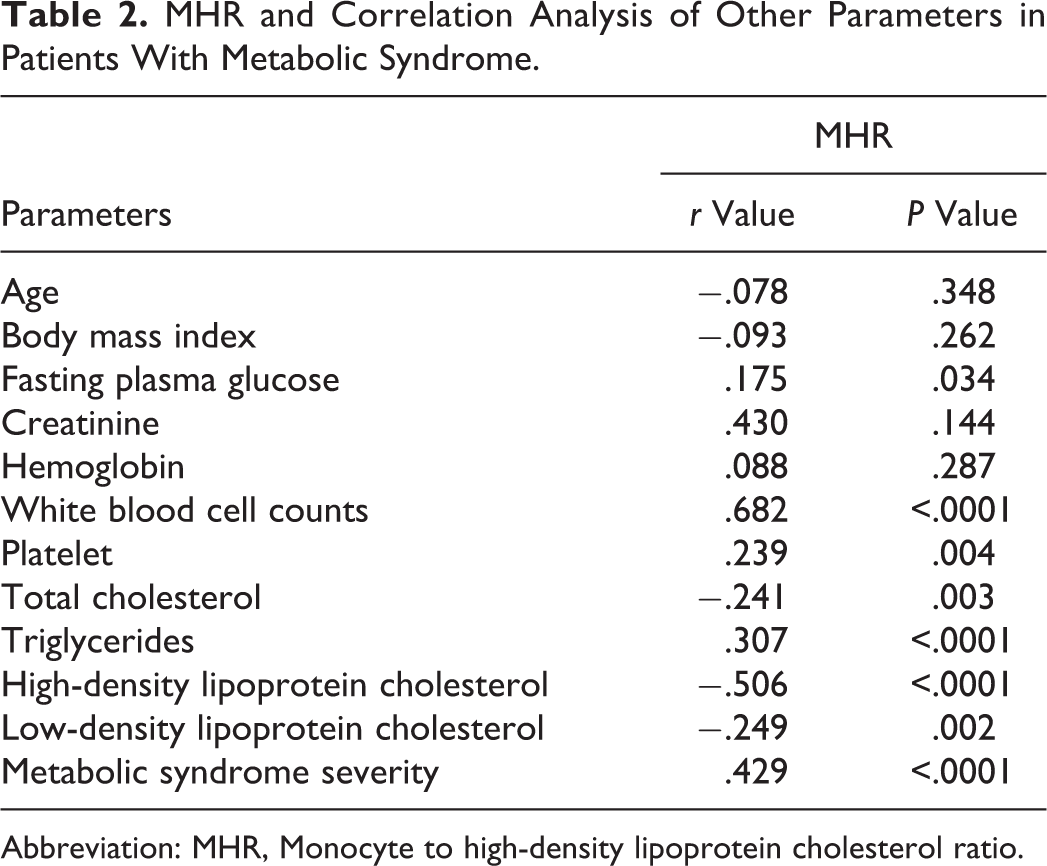
Abbreviation: MHR, Monocyte to high-density lipoprotein cholesterol ratio.
When patients with MetS were assessed with MHR in the study population, ROC curve analysis yielded a cutoff value of 9.36 with a sensitivity of 72%, a specificity of 61%, and a P value <.0001 (area under the curve: 0.714, 95% confidence interval [CI]: 0.654-0.774; Figure 3). In logistic regression analyses of MetS with several variables, MHR remained as an independent predictor of MetS (95% CI: 0.721-0.945, P = .005; Table 3). Logistic regression analysis results are presented in Table 3.
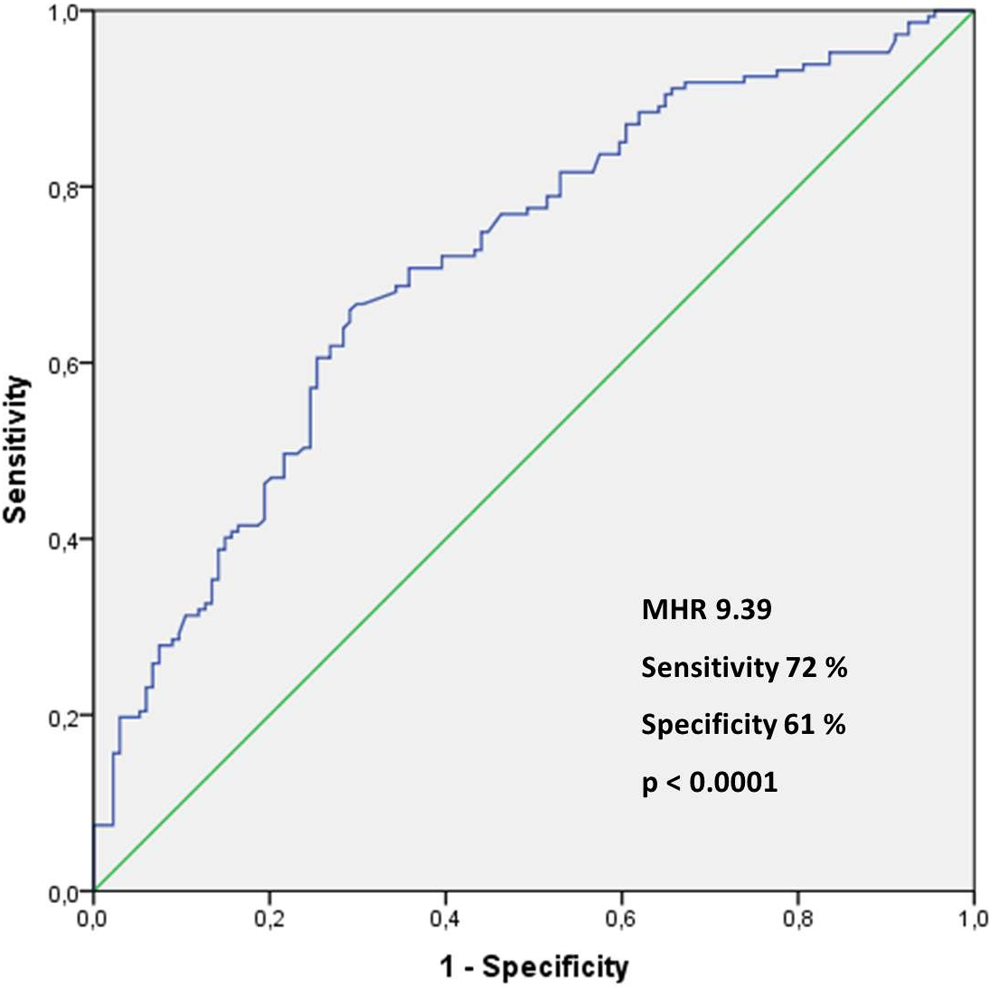
Receiver–operating characteristic curve of the monocyte to high-density lipoprotein cholesterol ratio for predicting metabolic syndrome.
Logistic Regression Analysis for Metabolic Syndrome.
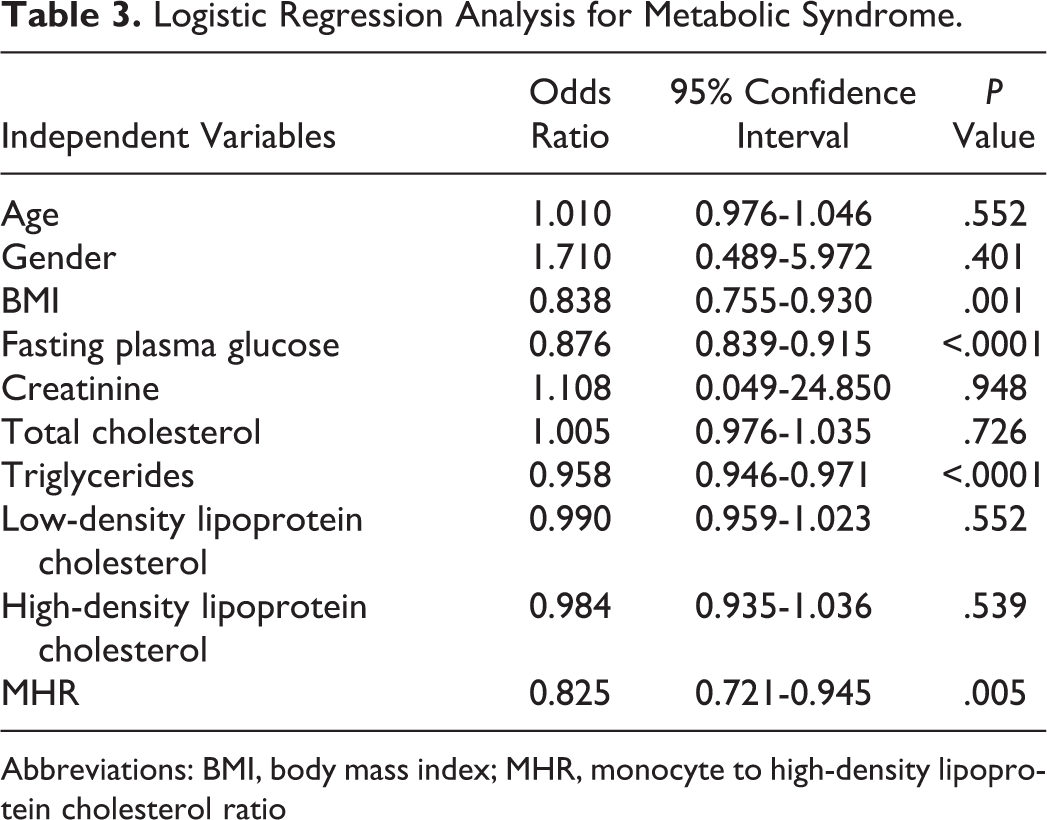
Abbreviations: BMI, body mass index; MHR, monocyte to high-density lipoprotein cholesterol ratio
Discussion
This study has investigated the effect of MHR on evaluation of MetS and its association with MetS severity. Our findings showed that MHR was higher in patients with MetS, compared to the control group. Monocyte to HDL-C ratio increased as the severity of disease increased, and a positive correlation was evident.
Atherosclerosis is a result of lipid accumulation on vessel walls; inflammatory processes and alterations in lipid levels have a significant role on its development and progression. Monocytes that are important immune system elements of inflammatory processes attach to endothelium, be converted to macrophages, settle in intimal and subintimal layers of vessel walls with oxidized low-density lipoprotein cholesterol (oxd-LDL-C), and form foam cells. 15,16 Meanwhile, HDL-C might prevent migration of macrophages and promote oxd-LDL-C output from these cells. Since anti-inflammatory features and its preventive role in atherosclerosis of HDL-C are well known, increase in MHR levels is suggested to predict disease progression and prognosis in cardiovascular disorders. 9,16 –18 In a study by Canpolat et al, 17 in patients with slow coronary flow, MHR was reported to be elevated. They also proved the correlation between increased MHR and slow coronary flow. Cetin et al 18 showed that MHR might be an independent predictor of the severity of coronary artery disease in patients with acute coronary syndrome. Arısoy et al 19 reported that in patients with myocardial infarction having ST-segment elevation, MHR was higher in patients with high thrombus load than those with low thrombus load, suggesting that MHR might be an independent predictor for thrombus load.
Although the process of atherosclerosis development is not yet well clarified, etiological causes and their interaction are undoubtedly complex. Metabolic syndrome includes various risk factors that increase the development of atherosclerosis and related cardiovascular disorders. 20,21 The complex process resulting from all those risk factors and their interaction is well proven to be related to inflammation. Obesity leads to activation of many inflammatory pathways by the secretion of pro-inflammatory cytokines and adipokines (such as leptin and resistin). Effects of adipokines and cytokines released from adipose tissue have been related to insulin resistance. 22,23 In patients with MetS, insulin resistance has an active role on both development and progression of this inflammatory process. As a result of the effects of insulin resistance on peripheral tissues, this process becomes a vicious circle. Besides, hypoxy that aggravates due to alterations in adipose tissue leads to increase in oxidative stress, macrophage infiltration, and rise in inflammatory cytokines, such as IL-1, IL-6, TNF-α and MCP-1. 11,22,23 Mirhafez et al 11 showed that cytokines such as IL-1α/β, IL-6, TNF-α, MCP-1 were higher in patients with MetS than the control group. Karabacak et al 12 reported that increased plasma MCP-1 levels and inflammation status might be related to cardiovascular risk in patients with low HDL-C.
All components of MetS are well known to be associated with inflammation. Glucose regulation disorder, hypertension, and dyslipidemia (high TG and low HDL-C) showed an association with low-grade inflammation. In patients with MetS, elevated TG and decreased HDL-C levels have important effect on this process. 24,25 Alterations in TG metabolism might lead to several changes in other lipids, and primarily HDL-C. In inflammation, decreased levels of HDL-C are associated with decrease in apoprotein A-1 (Apo A-1) synthesis in liver and changes in lecithin-cholesterol acyltransferase activity. 26 In addition, cytokines (such as IL-1, IL-6, and TNF-α) and chemokines (especially MCP-1) involved in the inflammatory process in patients with MetS play an important role in the mobilization and activation of monocytes from bone marrow. Activation of monocytes contributes to the secretion of these cytokines, as well. Besides, the replacement of Apo A-1 in the structure of HDL-C with SAA, which is released in response to cytokines from the liver and other tissues, may cause changes in the clearance and/or functional properties of HDL-C. 13,26,27 There are studies showing that HDL-C and Apo A-1 may prevent monocyte activation and attachment of monocytes to endothelium surface. Inflammation has an effect on onset and progression of atherosclerotic process. Monocyte activation and differentiation to lipid-loaded macrophages are basic issues on the development of atherosclerotic lesions. 16,28 Alterations that develop after close and complex relation between monocytes and HDL-C make MHR, which includes these 2 parameters, a significant marker. A study by Yayla et al 29 showed that MHR was higher in patients with hypertension than the control group. In another study, Aydin et al 30 reported that in patients with primary hypertension, MHR levels were higher than the control group. In the same study, they showed that MHR was higher in patients with primary hypertension with asymptomatic organ damage than in patients without organ damage. In addition, Vahit et al 31 reported that MHR was higher in patients with MetS compared to healthy controls.
In patients with MetS, regarding the role and significance of monocytes and HDL-C in the pathogenesis of the disease, MHR that includes both of these parameters might have several consequences. The high values of MHR in patients with MetS, its correlation with MetS severity, and the results of ROC and logistic regression analysis suggested that MHR might be a useful marker in the assessment of MetS.
Certain limitations of our study must be taken into account. During the study process, relationships between MHR and cytokines and other inflammatory markers have not been evaluated, prognostic role of MHR in cardiovascular end points has not been assessed, and the study has a single-centered retrospective design.
Conclusion
Metabolic syndrome generally presents with systemic inflammation and elevates the risk of cardiovascular disease development. With this study, it is suggested that MHR might be an available and useful inflammatory marker to evaluate patients with MetS and disease severity. Still, there is a need for multicentric, prospective studies to fortify our conclusions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.