
Abstract
To investigate potential clinical characteristics associated with discordance between platelet vasodilator-stimulated phosphoprotein phosphorylation (VASP-P) flow cytometry (FCM) assay and light transmission aggregometry (LTA) in defining high on-clopidogrel platelet reactivity (HPR) after ST-segment elevation myocardial infarction (STEMI). In this study, platelet responsiveness was measured by the above 2 methods simultaneously on day 1 and on day 6 of STEMI onset in 90 consecutive patients who underwent primary percutaneous coronary intervention. The FCM-derived platelet reactivity index and LTA-derived platelet aggregation rate were both significantly reduced after dual antiplatelet therapy on day 6. Multiple variable-adjusted logistic regression analysis revealed that smoking (odds ratio [OR]: 4.507, 95% confidence interval [CI]: 1.123-18.09, P = .034) and onset-to-admission time (per 1 hour increase, OR: 1.196, 95% CI: 1.023-1.398, P = .025) both were independent predictors for the discordance between the 2 methods. Additionally, improved correlation and concordance was observed in nonsmokers compared with smokers. Our data show that smoking and prolonged onset-to-admission time are associated with discordance between platelet VASP-P and LTA in defining HPR after STEMI, which should be considered when planning personalized antiplatelet therapy.
Introduction
P2Y12 receptor antagonism by thienopyridine is the cornerstone of current antiplatelet strategies recommended by practice guidelines to prevent ischemic events after percutaneous coronary intervention (PCI). Recent observational and interventional studies have identified a fraction of patients with increased risk of ischemic cardiovascular events despite receiving a standard regimen of clopidogrel, a widely used thienopyridine, which is termed high on-clopidogrel platelet reactivity (HPR). 1,2 The HPR is a strong predictor for myocardial infarction (MI) and cardiovascular death after PCI. 3,4 So far, several potential factors have been identified to influence HPR, including CYP2C19*2/*3 genetic polymorphisms, 5 microRNAs, 6 –8 drug interactions (calcium channel blockers 9 and proton pump inhibitors [PPIs] 10 ), and demographic characteristics, such as age, diabetes, obesity, and smoking. 11 –13
Clopidogrel can irreversibly bind to the P2Y12 receptor, leading to the inhibition of its downstream signaling pathway and consequently contributes to vasodilator-stimulated phosphoprotein phosphorylation (VASP-P)–mediated platelet glycoprotein IIb/IIIa (GPIIb/IIIa) inhibition 14 The platelet VASP-P level can be measured by quantitative flow cytometry (FCM), which is recognized as the most specific method for evaluating the degree of P2Y12 inhibition and lack of interference with aspirin or GPIIb/IIIa antagonists. 15,16 In addition to platelet VASP-P assay, platelet reactivity could be evaluated by the traditional light transmission aggregometry (LTA). From published literatures, the correlation between these 2 methods is modest, ranging from ∼0.4 to ∼0.5, 8,17 which indicates that these 2 methods are not interchangeable.
ST-segment elevation myocardial infarction (STEMI) is characterized by a highly prothrombotic state, 18,19 and the optimal duration of dual antiplatelet therapy after PCI in this population is still of controversy. 20 Accurate measurement of platelet reactivity is one of premises to personalized antiplatelet therapy after STEMI. The VASP-P-derived platelet reactivity index (PRI) and LTA-measured platelet aggregation (PAG) are both recommended by recent consensus to evaluate HPR. 1,2 Under this circumstance, discordance in measuring HPR is inevitably avoided when a cutoff binary value–based clinical dichotomy (responders or nonresponders) was used, which may lead to dilemma in clinical decision-making. Therefore, in the present study, we sought to evaluate potential clinical characteristics that associated with discordance in defining HPR in patients with STEMI, which is relevant for planning personalized antiplatelet therapy in this population.
Methods
Eligibility and Recruitment
We enrolled patients with STEMI presenting consecutively to Pingjin Hospital Heart Center. The diagnosis and treatment of STEMI was carried out according to recently published guideline. 21 Patients who were not suitable for primary PCI were excluded. Additionally, we only enrolled patients of Han nationality, the ethnic majority in China. Other exclusion criteria were as follows: (1) patients with congenital heart disease, valvular heart disease, congestive heart failure, cerebral and/or peripheral vascular disease, renal failure, liver insufficiency, cancer, or immune disorders and (2) patients with bleeding diathesis (platelet counts <150 × 109/L or >450 × 109/L, hemoglobin <80 g/L). All patients received a loading dose of 300 mg aspirin plus 300 mg clopidogrel and 100 mg aspirin plus 75 mg clopidogrel for the consecutive days. Informed consent was obtained from all patients, and the research protocol was approved by the ethical committee of Pingjin Hospital, which was in accordance with the principles of the Declaration of Helsinki.
Platelet Reactivity Assays
Blood samples for platelet VASP-P-FCM and LTA assays were drawn on day 1 (before clopidogrel and aspirin administration) and on day 6 of STEMI onset. The VASP-P analysis was performed within 2 hours after blood collection by a single trained and experienced technician using a platelet VASP kit (PLT VASP/P2Y12 kit, Biocytex, Marseille, France). The FCM analysis was performed using a Cytomics FC500 flow cytometer (Beckman Coulter, Miami, Florida) as previously described in our laboratory. 7,8 The PAG analysis was performed using a light transmission aggregometer (model 540-VS; Chrono-Log Corporation, Havertown, Pennsylvania) with 10 μmol/L adenosine diphosphate (ADP) (P/N 384, Chrono-Par ADP reagent; Chrono-Log Corporation) in stirred (1000 rpm) platelet-rich plasma as previously described. 8
CYP2C19*2/*3 Genetic Polymorphisms
The CYP2C19*2/*3 genetic polymorphism analysis was performed as previously described. 7,8 Briefly, genomic DNA was extracted, and the polymerase chain reaction (PCR) was performed using the following primers: CYP2C19*2: forward primer 5′-AATTAC AAC CAG AGC TTG GC-3′ and reverse primer 5′-TAT CAC TTT CCA TAA AAG CAA G-3′; CYP2C19*3: reverse primer 5′-TGT GCT CCC TGC AAT GTG AT-3′ and R 5′-TTT GGG GCT GTC ACC AAA GT-3′. The PCR products were purified with a commercially available kit (TaKaRa MiniBEST DNA Fragment Purification Kit ver. 3.0, Shiga, Japan) and the genotypes of CYP2C19*2/*3 were identified using restriction fragment length polymorphism with SmaI (QuickCut SmaI; TaKaRa)/BamHI (QuickCut SmaI; TaKaRa). The products were then separated on a 3%/2% agarose gel, and the electrophoretic bands were visualized with ethidium bromide using ChemiDoc XRS + Imaging System (BioRad, Hercules, California).
Other Measurements
Information on medical history, current health status, and medications was obtained by questionnaires. Onset-to-admission time was defined as the time of patient from onset of symptoms to reach the hospital. Smoking status was defined as current smoker (smoking ≥5 cigarettes/day or stopped <1 month and lasted more than 5 years before STEMI onset) and nonsmokers (stopped ≥1 month before STEMI onset or never smoking). Diabetes was defined as baseline use of oral antidiabetes medications or insulin. Hypertension was defined as a self-reported history of high blood pressure or the use of antihypertensive medication. Blood routine tests and biochemical assays were performed using an automated hematology analyzer (XE-5000; Sysmex, Kobe, Japan) and a Hitachi 7180 Clinical Analyzer (Hitachi, Tokyo, Japan), respectively. Transthoracic echocardiography was performed by a Philips iE33 system (Phillips, Andover, Massachusetts) on day 2. Analyses were carried out by an experienced technician blinded to the clinical and angiographic data.
Statistical Analysis
The Shapiro-Wilk test was used to assess normality. Continuous variables with normal distributions are presented as mean (standard deviation) and otherwise expressed as medians with interquartile ranges. For comparisons of platelet responsiveness before and after dual antiplatelet therapy, a Wilcoxon matched-pair test was used. For other unpaired continuous data, an unpaired Student t test or a Mann-Whitney U test was used. Categorical data were expressed as percentage and compared with Fisher exact test. Correlation between PAG and PRI was calculated using Pearson coefficient. As recent consensuses suggested cutoff values of 70% for PAG-determined (10 μmol/L ADP-induced aggregation 1 ) and 50% for PRI-determined HPR, 2 respectively, all patients with STEMI could either be classified as concordance group (refers to PAG ≥ 70% and PRI ≥ 50% or PAG < 70% and PRI < 50%) or as discordance group (refers to PAG ≥ 70% and PRI < 50% or PAG < 70% and PRI ≥ 50%), according to PAG and PRI levels measured on day 6. Agreement between HPR classifications by 2 tests was determined by κ statistics. To determine the factors that may influence the individual’s responsiveness to clopidogrel treatment (concordance or discordance) between VASP-P and PAG measurements, univariate followed by multivariable-adjusted binary logistic regression analyses was used. Receiver operating characteristic (ROC) curves were plotted to assess the accuracy of PAG for discriminating between PRI-determined low and normal responders to clopidogrel. All statistical analyses were performed using SPSS version 15.0 (SPSS, Chicago, Illinois) and GraphPad Prism version 5 (GraphPad Prism Software Inc, San Diego, California). A 2-tailed P value <.05 was considered statistically significant.
Results
Patient Characteristics
A total of 90 consecutive patients with STEMI who underwent primary PCI were enrolled in this study. The demographic and clinical features are shown in Table 1. The average symptom onset-to-admission time was 4.0 hours. Compared with day 1, PRI and PAG levels were both significantly decreased on day 6 (for PRI medians: 71.1% vs 41.9%; for PAG medians: 75.5% vs 64.9%, both P < .001; see Figure 1). Because the number of allele mutant genotype of CYP2C19*2 is relatively rare, we pooled the allele and heterozygous mutants together as the mutant genotype. The PRI-determined low responders tend to have a higher prevalence of mutant CYP2C19*2 genotype (P = .075; Table 1). There was no obvious difference in other clinical characteristics between PRI-determined normal and low responders (Table 1). The PAG-determined low responders had higher presence of anterior MI, as well as lower left ventricular ejection fraction (LVEF; borderline significance; Table 1). A 2-year follow-up data showed that no significant differences in cardiovascular events were found between low responders and normal responders determined by the 2 assays (Supplementary Table 1).
Patient Clinical Characteristics Stratified by Discharge VASP-P and PLA Assays.
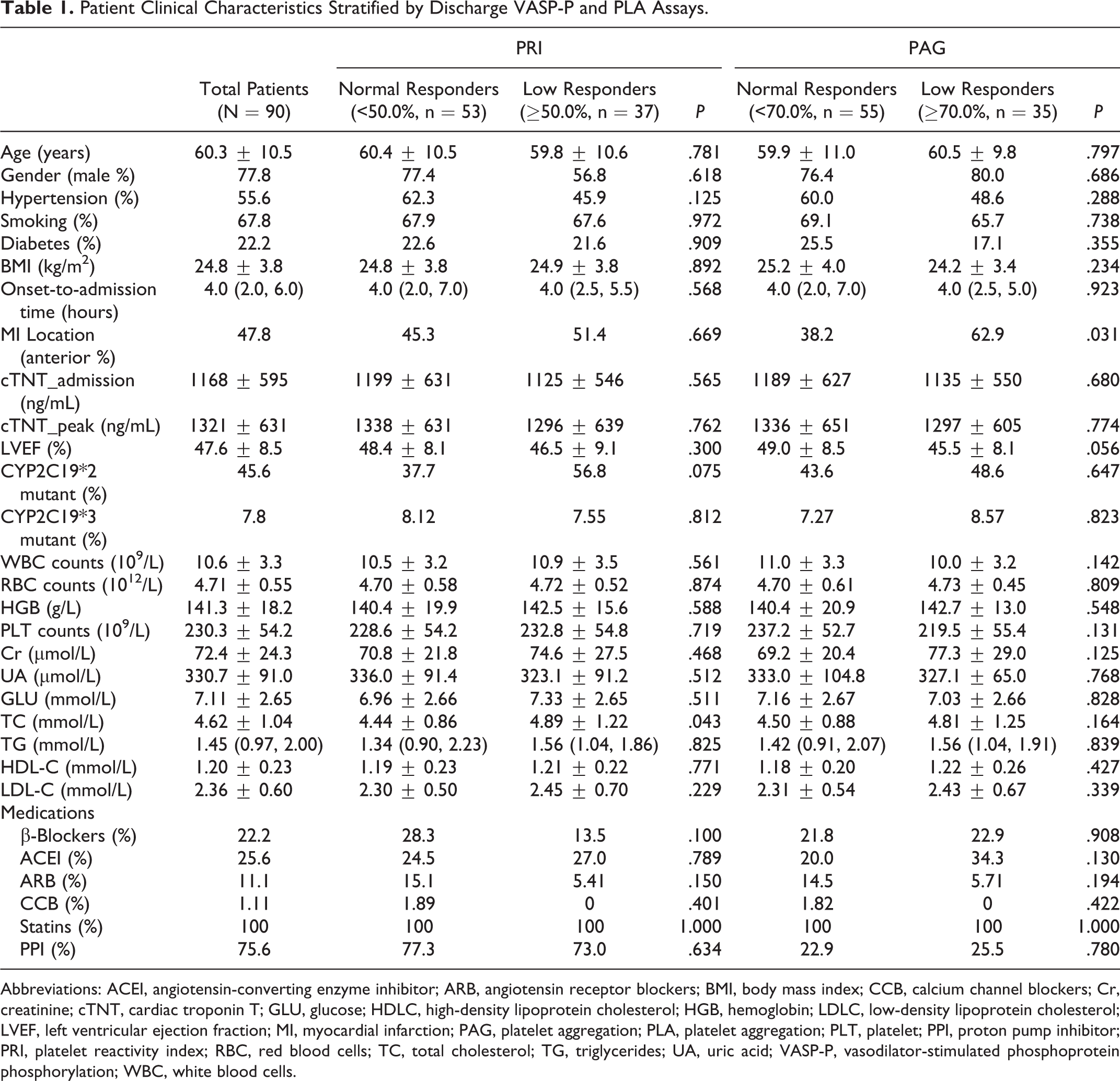
Abbreviations: ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blockers; BMI, body mass index; CCB, calcium channel blockers; Cr, creatinine; cTNT, cardiac troponin T; GLU, glucose; HDLC, high-density lipoprotein cholesterol; HGB, hemoglobin; LDLC, low-density lipoprotein cholesterol; LVEF, left ventricular ejection fraction; MI, myocardial infarction; PAG, platelet aggregation; PLA, platelet aggregation; PLT, platelet; PPI, proton pump inhibitor; PRI, platelet reactivity index; RBC, red blood cells; TC, total cholesterol; TG, triglycerides; UA, uric acid; VASP-P, vasodilator-stimulated phosphoprotein phosphorylation; WBC, white blood cells.
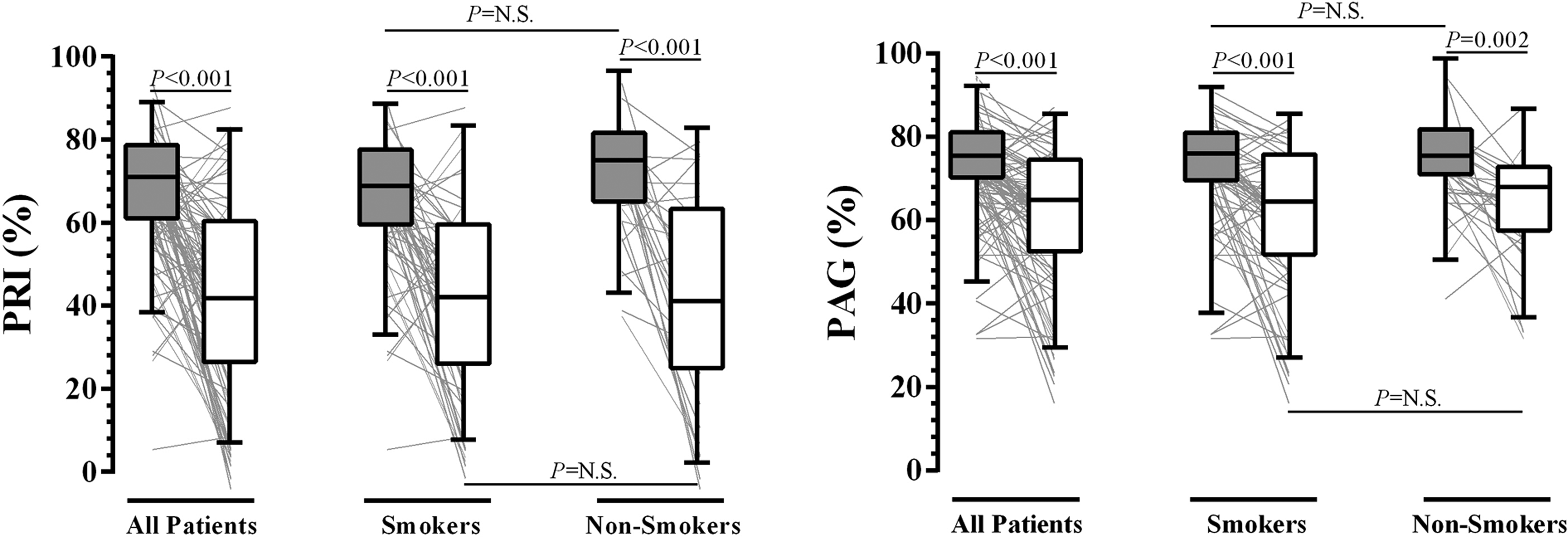
Platelet function tests on day 1 (gray box) and day 6 (white box) of ST-segment elevation myocardial infarction (STEMI) onset. The box and whisker plots: the boxes extend from the 25th to the 75th percentile, with a line at the median. The whiskers extend above and below the box to show the 5th to 95th percentiles of values. The lines beneath each box and whisker plot indicate each individual’s platelet reactivity index (PRI)/platelet aggregation (PAG) value (connecting the values of day 1 and day 6).
Logistic Regression
The clinical characteristics of concordance and discordance groups defined by VASP-P and LTA testing results on day 6 are shown in Table 2. The concordance group included 62 patients (n = 22 for PAG ≥ 70% and PRI ≥ 50%; n = 40 for PAG < 70% and PRI < 50%; see Figure 2), and discordance group consisted of 28 patients (n = 13 for PAG ≥ 70% and PRI < 50%; n = 15 for PAG < 70% and PRI ≥ 50%; see Figure 2). Compared with the concordance group, higher prevalence of smoking and prolonged onset-to-admission time were observed in the discordance group. Other clinical variables were comparable between them. Using logistic regression models, we identified STEMI symptom onset-to-admission time and smoking both were associated with the presence of discordant testing results by the 2 methods (Table 3). After adjustment by other factors that have been reported to influence platelet reactivity (age, body mass index, CYP2C19*2 and CYP2C19*3 polymorphisms, diabetes, and PPI use), onset-to-admission time and smoking status remained statistically significance (Table 3).
Patient Clinical Characteristics Stratified by Concordance/Discordance Between Discharge VASP-P and PLA Assays.
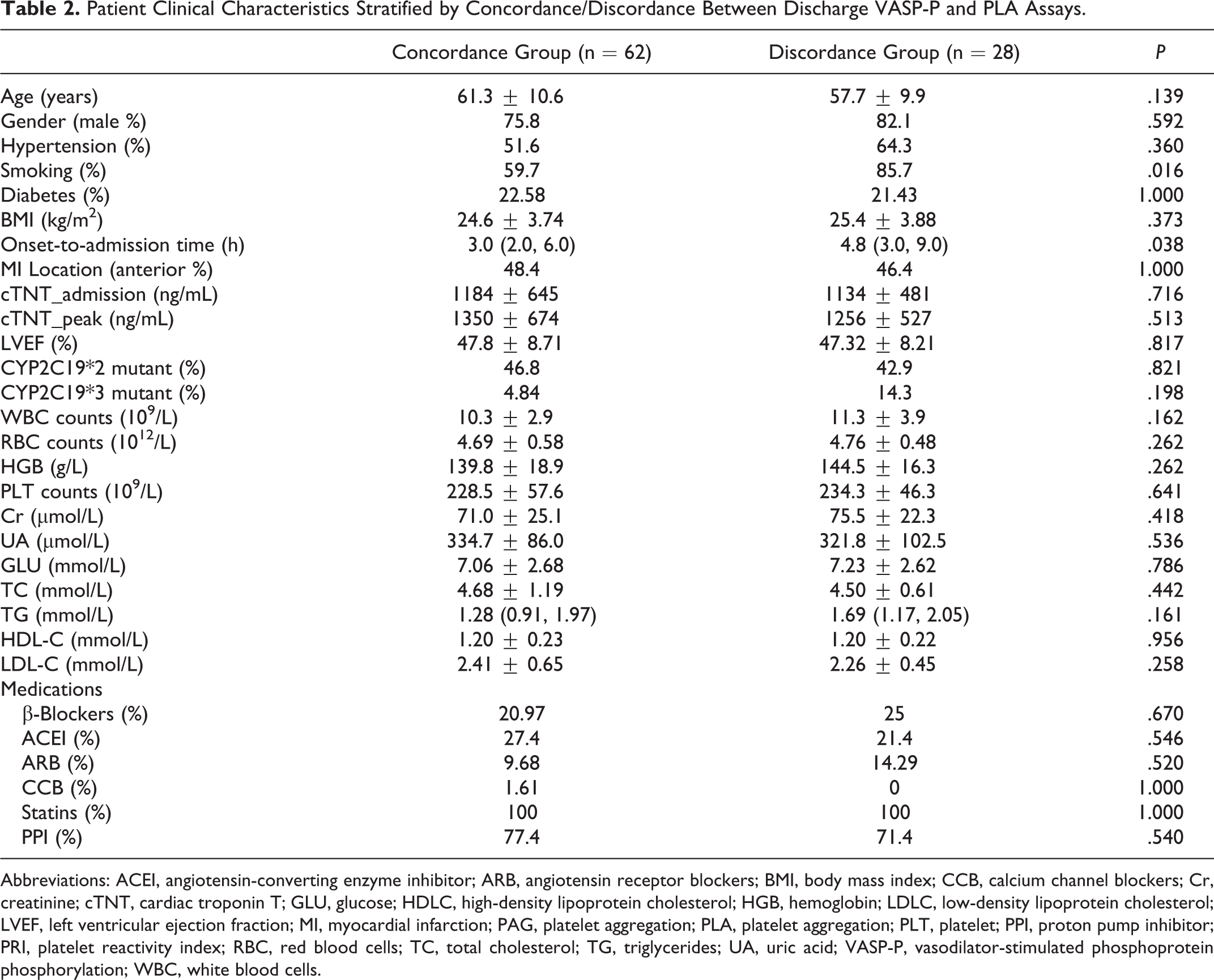
Abbreviations: ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blockers; BMI, body mass index; CCB, calcium channel blockers; Cr, creatinine; cTNT, cardiac troponin T; GLU, glucose; HDLC, high-density lipoprotein cholesterol; HGB, hemoglobin; LDLC, low-density lipoprotein cholesterol; LVEF, left ventricular ejection fraction; MI, myocardial infarction; PAG, platelet aggregation; PLA, platelet aggregation; PLT, platelet; PPI, proton pump inhibitor; PRI, platelet reactivity index; RBC, red blood cells; TC, total cholesterol; TG, triglycerides; UA, uric acid; VASP-P, vasodilator-stimulated phosphoprotein phosphorylation; WBC, white blood cells.
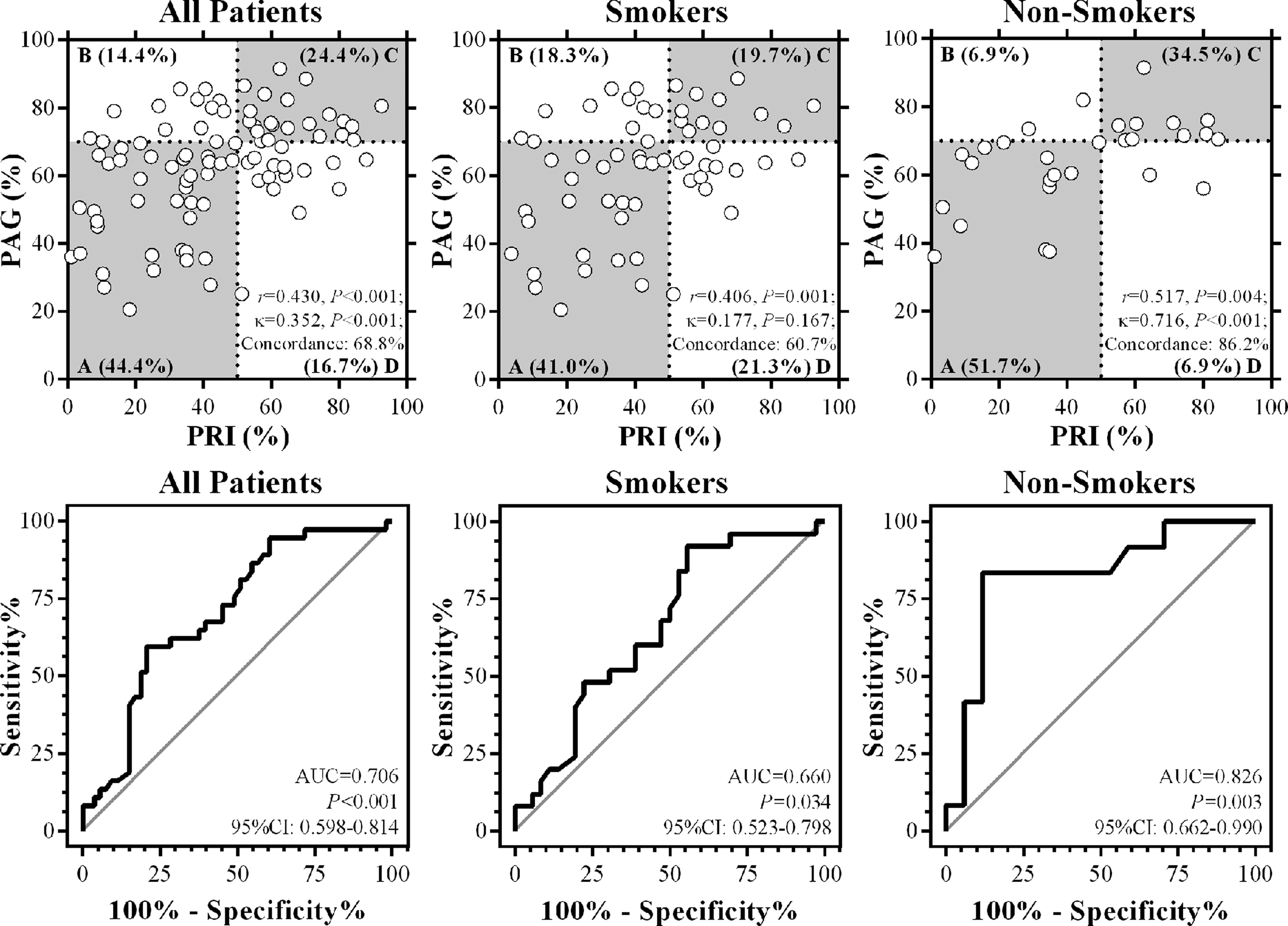
Correlation and method agreement analyses of 2 platelet function testing on day 6 of ST-segment elevation myocardial infarction (STEMI) onset. The upper panel shows the linear correlation and κ statistics (concordance analysis) of all 90 patients with STEMI, 61 smokers and 29 nonsmokers, respectively. The dots within 2 gray areas (A and C) in the plots indicate patients of concordance group, whereas the dots within 2 white areas (B and D) indicate patients of discordance group. The lower panel shows the receiver operating characteristic (ROC) curve analyses of the discriminative capacity of platelet aggregation (PAG) to identify platelet reactivity index (PRI)–determined high on-clopidogrel platelet reactivity (HPR) of all 90 patients with STEMI, 61 smokers and 29 nonsmokers, respectively.
Logistic Regression Analyses.a
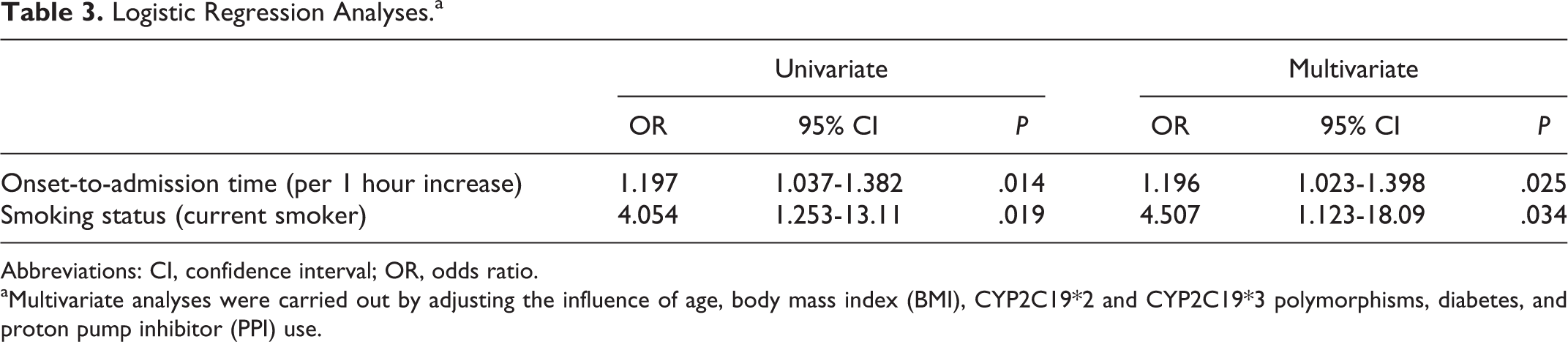
Abbreviations: CI, confidence interval; OR, odds ratio.
aMultivariate analyses were carried out by adjusting the influence of age, body mass index (BMI), CYP2C19*2 and CYP2C19*3 polymorphisms, diabetes, and proton pump inhibitor (PPI) use.
Impact of Smoking Status on Platelet Reactivity Testing Results
Smoking prevalence was 67.8% (61 of 90) in total cohort, and the prevalence was comparable between PRI- and PAG-determined normal and low responders (Table 1). As shown in Figure 1, there were no significant differences in PRI levels on day 1 and day 6 between smokers and nonsmokers, nor were PAG levels between smokers and nonsmokers. On day 6, linear correlation and κ statistics analyses revealed that the correlation coefficient and concordance between 2 methods were significantly reduced in smokers, compared with nonsmokers (Figure 2, upper panel). Additionally, using ROC curve analysis, the discriminative capacity of PAG in identifying PRI-determined low and normal responders after dual antiplatelet therapy was significantly reduced in smokers (Figure 2, lower panel).
Impact of Onset-to-Admission Time on Discordance Between PAG and PRI Tests
As shown in Supplementary Figure 1, ROC analysis showed that the cutoff value of onset-to-admission time causing discordance between PAG and PRI tests is 3.25 hours, the sensitivity is 67.86%, and the specificity is 51.61%.
Discussion
The STEMI is characterized by a highly prothrombotic state. 18,19 Efficient antiplatelet therapy has been clearly shown to prevent stent thrombosis and recurrent ischemic events in patients with STEMI receiving primary PCI. 20,22 To maximize the clinical benefit, maintaining the platelet reactivity within the therapeutic window during dual antiplatelet therapy is desirable, which requires accurate measurement of platelet reactivity. In this report, we sought to investigate the potential clinical characteristics associated with the discordant testing results between 2 widely used methods, that is, platelet VASP-P by FCM and PAG by LTA, in patients with STEMI receiving primary PCI. Using cutoff values of PRI ≥ 50% and PAG ≥ 70% (measured on day 6 of STEMI onset), respectively, to define HPR, 1,2 for the first time to our knowledge, we found that smoking and prolonged symptom onset-to-admission time both independently predict discordance between VASP-P and PAG-determined HPR. This finding reinforces the idea that, to plan for personalized antiplatelet therapy in patients with STEMI after PCI, smoking cessation or switch to novel P2Y12 antagonists (prasugrel/ticagrelor 23,24 ), which are not influenced by smoking status, should be considered.
Smoking represents one of the most important preventable and modifiable risk factors for the development of atherosclerosis 25 and is the strongest independent predictor for recurrent cardiovascular events in young MI survivors. 26 Mounting evidence shows that smoking induces multiple pathological effects, which result in platelet activation, adhesion, and aggregation. 27 On the other hand, however, recent studies showed that, compared with nonsmokers, smokers have a faster onset of clopidogrel action with great platelet inhibition, a phenomenon termed “smoker paradox,” which is associated with increased CYP1A2 activity or upregulation of CYP2B6 expression by nicotine. 28 Thus, smoking may positively modify the clinical efficacy of clopidogrel 23 and is associated with more clinical benefits than nonsmokers during dual antiplatelet therapy. 29 –31 Consequently, smoking poses contrasting effects on platelet activation in clopidogrel-treated patients, and the balance between these 2 opposing effects determines an individual’s response to P2Y12 inhibition. Notably, a recent well-designed study seems to support the enhanced platelet inhibition serving as the dominant force in clopidogrel-treated smokers. 32
Our data showed that smoking exposure could significantly lead to discordance of the 2 platelet function testing results, as demonstrated by a lower correlation coefficient and a lower concordance index κ. After adjustment by traditional risk factors that associated with HPR (age, obesity, CYP2C19*2 and CYP2C19*3 polymorphisms, diabetes and PPI use), smoking remains an independent predictor for discordant platelet function testing results. Additionally, as shown in Figure 3, the variations of platelet function testing results in smokers are more obvious compared with nonsmokers, especially in terms of PAG values, which indicates cigarette smoke exposure may confer a heterogeneous effect on platelet activation in population level.
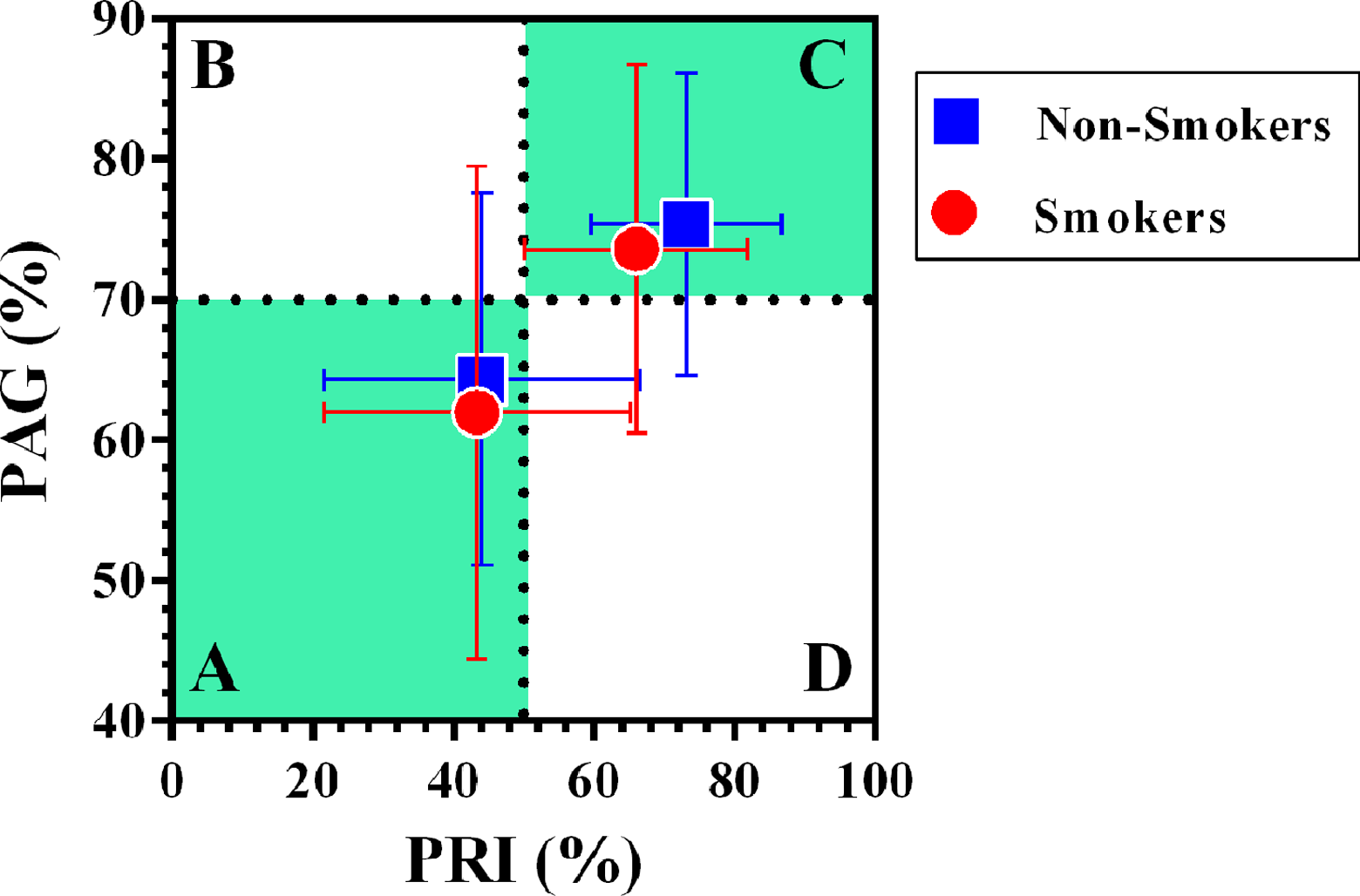
Data distribution of 2 platelet function testing results on day 1 and day 6 of ST-segment elevation myocardial infarction (STEMI) onset. The dots within area C indicate measured means on day 1 (before dual antiplatelet therapy), whereas dots with area A indicate measured means on day 6 (dual antiplatelet therapy for 6 days). The horizontal and vertical error bars indicate standard deviations of platelet reactivity index (PRI) and platelet aggregation (PAG), respectively. STEMI indicates ST-elevation myocardial infarction; PRI: platelet reactivity index; PAG: platelet aggregation.
Another finding from this study is that STEMI symptom onset-to-admission time is also independently associated with discordant testing results. Results from basic and clinical studies have demonstrated that acute heart failure would lead to increase angiotensin II levels, sympathetic overdrive, reduce nitric oxide bioavailability, and elevate inflammation cytokines. 33 All these alterations, via yet-to-be established mechanisms, contribute to platelet activation in acute heart failure. 33 In our study, in HPR patients defined by PAG levels, an increased incidence of anterior MI, as well as a decrease in LVEF (P = .056; Table 1), was observed. These characteristics are in agreement with the findings that patients with acute heart failure are more likely to present with activated state of platelets. Moreover, our previous study have shown that the number of monocyte–platelet aggregates were increased in patients with STEMI, 34 as a marker of inflammation and thrombotic disease, 35,36 themonocyte–platelet aggregates may affect the PAG determination, and a delayed onset-to-admission time indicates greater MI size and more severe inflammatory responses which may influence the concordance of PAG and PRI tests. In contrast to the positive modifying effect of smoking on clopidogrel-induced platelet inhibition, increased onset-to-admission time thus poses a negative effect on clopidogrel-induced platelet inhibition. Therefore, a prolongation in onset-to-admission time would further add complexity to an individual’s response to clopidogrel, contributing to heterogeneous testing results by widening data distributions in smokers.
In this work, the finding that smoking widens the data distribution of platelet function testing, especially in PAG levels, may also be interpreted as a potential increase in bleeding risk. However, data available so far are inclusive on this point: Some post hoc analyses supported a positive impact of smoking on bleeding risk, 11,37 while other reports did not. 31 Thus, the impact of smoking on bleeding risk in clopidogrel-treated patients remains an open question.
The present study has the following limitations. First, the relatively small sample size is not statistically powered to investigate the association between the discordant testing results and clinical outcomes, especially ischemic/bleeding events. Second, smoking status used in this study was neither quantified as pack year nor measured in serum cotinine levels, which did not allow us to investigate the quantitative effect of smoking on the discordant testing results by 2 methods. This may account for the lack of difference of PRI and PAG levels between smokers and nonsmokers in our study, because recent study showed that there might be a dose-dependent response of smoking on clopidogrel-induced platelet inhibition. 38 Third, the HPR cutoff values used in this work are obtained from recent consensus paper using post-PCI studies involving patients with stable or acute coronary syndrome; therefore, it is unclear that whether these threshold values are capable of predicting ischemic/bleeding events in patients with STEMI treated with primary PCI.
Conclusions
In this study, we demonstrate that smoking and prolonged onset-to-admission time are independent predictors for the discordance between platelet VASP-P and LTA in defining HPR (on clopidogrel) in patients with STEMI receiving primary PCI. Because LTA is susceptible to external factors with a poor reproducibility of the results, the VASP-P assay may be more suitable for defining HPR in patients with STEMI. Our work supports the concept that, to plan for personalized antiplatelet therapy after STEMI, smoking cessation or switch to novel P2Y12 antagonists is desirable.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect tothe research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received funding from National Natural Science Foundation of China (81170238, 81570335, and 81600328), Tianjin Municipal Science and Technology Committee (14JCYBJC27600 and 16JCQNJC11800), and Intra-mural research grants from Pingjin Hospital (FYZ201402, 2015ZXKF11, and FYM201533) to carry out this study.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.