
Abstract
Total joint arthroplasty (TJA) of the hip or knee (THA and TKA) is the primary surgical intervention for individuals with degenerative joint disease (DJD). Although it is commonly thought that shear force on the joint causes the degradation of articular cartilage, it is possible that there are other factors that contribute to the progression of DJD. It is plausible that specific enzymes that degrade the joint are upregulated, or conversely, there is downregulation of enzymes critical for joint lubrication. The aim of this study is to profile collagenase-1, elastase, heparanase, and lubricin levels in patients undergoing TJA in order to determine potential preexisting dysregulation that contributes to the pathogenesis of DJD. Deidentified blood samples were obtained from patients undergoing TJA 1 day pre- and 1 day postoperatively. Plasma samples were analyzed using enzyme-linked immunosorbent assay kits for elastase, collagenase-1, heparanase, and lubricin. In comparison to healthy controls, there were significant increases in circulating collagenase-1, elastase, and lubricin levels in both the preoperative and postoperative samples. There were no significant differences in heparanase levels in the preoperative or postoperative samples. Comparing the preoperative versus postoperative patient samples, only lubricin demonstrated a significant change. The results of this study confirm that patients undergoing TJA have preexisting alterations in the levels of matrix-degrading enzymes and lubricin. The alterations observed in this study may provide insight into the pathogenesis of DJD.
Introduction
The prevalence of total knee arthroplasty (TKA) and total hip arthroplasty (THA) has been increasing progressively, and this trend is predicted to continue. It has been projected that the total annual number of TKA and THA procedures will exceed 4 million by 2030. 1 Studies have previously investigated biomarkers in patients undergoing TKA or THA to identify those which may contribute to the pathogenesis of degenerative joint disease (DJD). Altered levels of various biomarkers have been reported in patients both pre- and postoperatively. 2,3 Since TKA and THA are commonly performed on individuals who experience degeneration of their joints, it is of particular interest to determine whether levels of matrix-degrading enzymes (MDEs), specifically elastase, collagenase-1, and heparanase along with the lubricating compound lubricin, are altered as part of the disease process. Although osteoarthritis (OA), a prevalent form of DJD, is characterized by degeneration of articulating cartilage, it may also involve the synovium and subchondral bone. 4 It is commonly accepted that the pathogenesis of DJD involves shear force on load-bearing joints. With the force that normally occurs on joints, there is a continuous damaging-healing process that occurs in trabecular bone in the form of microfractures that are subsequently healed by remodeling. The remodeling results in stiffer, thickened bone that more appropriately resists stress; however, this stiffer bone is less effective at absorbing shock and weight-bearing force. 5,6 This phenomenon may also explain why older individuals and those with a higher body mass index (BMI) are more prone to experiencing OA—these patients experience more force on the joints for a longer period of time. It is still unclear whether the subchondral bone thickening is an initiating factor or the result of cartilage loss. Additionally, it has been suggested that pro-inflammatory cytokines produced in the synovium diffuse through the synovial fluid (SF) to the cartilage and activate chondrocytes to produce more pro-inflammatory cytokines. 4 In trying to elucidate the multifactorial pathophysiology of DJD, it is crucial to examine MDEs for their possible role in the progression of DJD. It has been reported that the synovium in patients with OA is thickened, has increased vascularity, and has inflammatory cell infiltrates. 7 These compounds may leak into circulation and may be detectable, thus emphasizing the importance of examining the plasma of these patients.
The major function of elastase is elastin degradation, yet it has also been observed to play a role in cartilage destruction. 8 Although the major component of articular cartilage is type II collagen, type collagen III has been identified in articular cartilage at varying levels. 9 Type III collagen is known to be predominant in healing tissues, most commonly associated with dermal and epidermal healing. The repetitive damage-healing cycle of DJD may induce elevated expression of type III collagen. 10 The importance of this observation is that elastase has the ability to act as a “collagenase” and degrade type III collagen 11 ; if patients with DJD have increased type III collagen, elastase may hold more significance in the pathogenesis of DJD than previously thought. Elastase is also secreted by neutrophils and contributes to the pathogenesis of chronic inflammation by inhibiting neutrophil activation via negative feedback mechanisms. 12
Collagenase-1 is a matrix metalloproteinase (MMP-1). Matrix metalloproteinases are enzymes that break down extracellular matrix. Although collagenase-1 may be present at negligible circulating levels in healthy patients, it has been found to be increased in the joints of those with OA, 13 providing supportive evidence for its role in the pathogenesis of DJD. Although MMPs are specifically regulated by tissue inhibitor of metalloproteinases (TIMPs), it has been shown that patients with OA had elevated levels of circulating TIMP-1 and inhibitor of collagenase-1. 14 This increase in TIMP-1 may occur as an intrinsic attempt to downregulate the effects of collagenase-1.
Heparanase, in addition to cleaving heparan sulfate, has been implicated in the promotion of angiogenesis, thus allowing for increased nutrient supply to the joint. 15 Heparanase may be important in preservation of articular cartilage. Previously, it was found that the A Disintegrin And Metalloproteinase with Thrombospondin motifs (ADAMTS-4) enzyme cleaves chondroitin sulfate hyaluronan-binding proteoglycans, including aggrecan,which is a crucial structural component of cartilage. ADAMTS-4 has been observed to be upregulated in patients with OA. However, the lack of ADAMTS-5 is what inhibited cartilage degradation in mouse models. The heparan sulfate proteoglycan, syndecan-4, regulates ADAMTS-5 activation and cartilage breakdown in the murine model. 16 It may be possible that heparanase acts as an upstream regulator in this process by cleaving heparan sulfates, thus altering functionality.
Lubricin is an SF glycoprotein that is expressed in cartilage derived from mesenchymal stem cells. Lubricin plays an important role in joint mobility and may have matrix-stabilizing properties. Lubricin was shown to interact with SF components to reduce friction in joints. In healthy patients, lubricin forms a thin layer coating the articulating cartilage, which reduces the coefficient of kinetic friction. 17 Jay et al demonstrated how an intra-articular injection of lubricin decreased type II cartilage degradation in an animal model. These findings indicate that lubricin levels are also present in detectable levels in SF and potentially in circulation as well. 18
Although previous studies have investigated MDEs in TKA and THA patients, particularly involving prosthesis loosening, the role of lubricin is not yet clear. 2 Since collagenase-1 and elastase are known to degrade collagen, and heparanase degrades the ECM, it is possible these compounds are involved in the pathogenesis of DJD. Simultaneous measurement of these MDEs and lubricin may provide additional information on their contribution to the pathogenesis of joint diseases. These findings may indicate the importance of lubricin and these MDEs in joint or matrix stability and postsurgical recovery. To date, a study comparing the plasma of normal patients with that of TKA and THA patients both pre- and postoperatively has not been reported.
Patients and Methods
Deidentified blood samples were obtained from 45 patients undergoing TKA (n = 27) or THA (n = 18) day 1 preoperatively and day 1 postoperatively. The patient ages ranged from 48 to 85 years, with a mean age of 64.9 ± 10.5 years. Patient blood samples were collected into tubes containing 3.2% sodium citrate and plasma was then isolated. In order to reduce repeated freeze–thaw cycles, patient plasma samples were aliquoted into separate tubes. Citrated plasma samples from healthy individuals (aged 18-35, nonsmokers) were obtained from George King Biomedical, Inc (Overland Park, Kansas) to serve as controls. Patient and control plasma samples were stored at −80°C. Plasma samples were analyzed using enzyme-linked immunosorbent assay (ELISA) kits for elastase (Abcam, Cambridge, United Kingdom), collagenase-1 (R&D Systems, Minneapolis, Minnesota), heparanase, and lubricin (MyBioSource.com, San Diego, California). This study was approved by the institutional review board of Loyola University Chicago Health Sciences Division. Patients undergoing total joint arthroplasty (TJA) revision were excluded from this study.
Statistical Analysis
Data were analyzed using Microsoft Excel and using GraphPad Prism software (version 6). The results were expressed as median ± interquartile range. Comparisons between groups were made using the nonparametric Mann-Whitney U test for nonnormally distributed quantitative data. Correlation analysis was carried out using the nonparametric Spearman test. P values <.05 were considered statistically significant.
Results
There were significant differences in collagenase-1 levels in the preoperative (0.48 ± 0.35 ng/mL vs 0.17 ± 0.13 ng/mL; P < .0001) and postoperative (0.59 ± 0.69 ng/mL vs 0.17 ± 0.13 ng/mL; P < .0001) patient samples compared to the control samples. The difference in collagenase levels between the preoperative and postoperative samples was not statistically significant (P = .836; Figure 1).
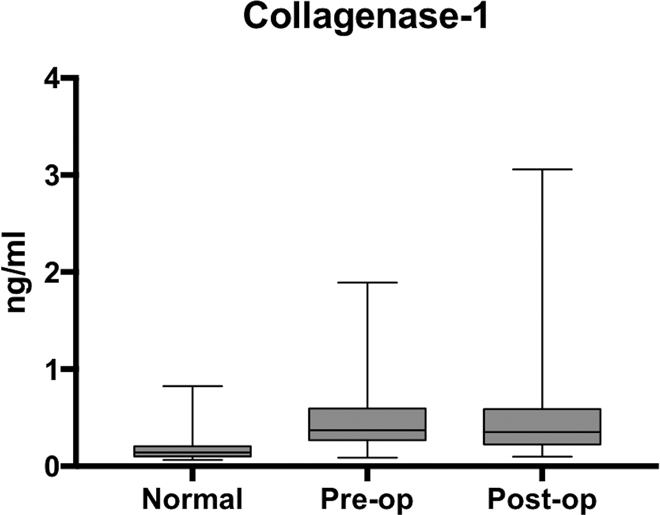
Box plot showing median levels of collagenase-1 (matrix metalloproteinase 1 [MMP-1]) measured in control, preoperative, postoperative groups. Boxes show interquartile ranges, and I bars demonstrate highest and lowest values. Preoperative versus control, P < .0001; postoperative versus control, P < .0001; and preoperative versus postoperative, P = .836.
There was a significant difference in the preoperative (200.9 ± 169.3 ng/mL vs 5.9 ± 10.4 ng/mL; P < .0001) and postoperative (225.6 ± 234.9 ng/mL vs 5.9 ± 10.4 ng/mL; P < .0001) levels of elastase compared to control. No difference in elastase levels was observed comparing the pre- versus postoperative samples (P = .855; Figure 2).
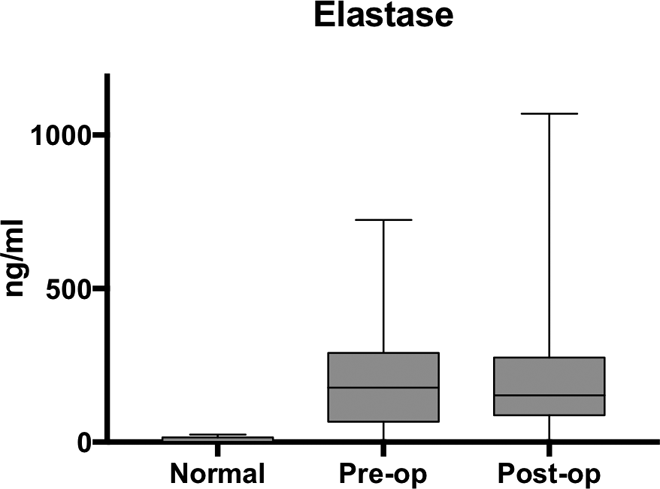
Box plot showing median levels of elastase measured in control, preoperative, postoperative groups. Boxes show interquartile ranges, and I bars demonstrate highest and lowest values. Preoperative versus control, P < .0001; postoperative versus control, P < .0001; and preoperative versus postoperative, P = .855.
Heparanase levels in the control samples (957 ± 1017 pg/mL) were not significantly different from those measured in the preoperative (926 ± 982 pg/mL; P = .7477) and postoperative (724 ± 884 pg/mL; P = .7946) patient samples. Although the mean level of heparanase trended lower postoperatively, this difference was not statistically significant (P = .3504; Figure 3).
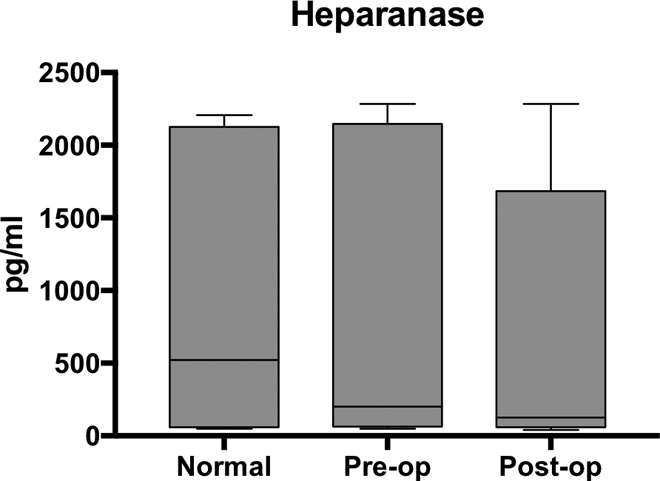
Box plot showing median levels of heparinase measured in control, preoperative, and postoperative groups. Boxes show interquartile ranges, and I bars demonstrate highest and lowest values. Preoperative versus control, P = .7477; postoperative versus control, P = .7946; and preoperative versus postoperative, P = .3504.
Lubricin levels were significantly elevated in the preoperative (4328 ± 1828; P = .0011) and postoperative (5462 ± 1512; P < .0001) samples compared to control (2344 ± 1737). Lubricin levels were also observed to increase significantly as a result of surgery (P = .0001; Figure 4). A positive correlation was observed between collagenase-1 and elastase in the preoperative patient samples (P = .0129, r = .4415), as shown in Figure 5.
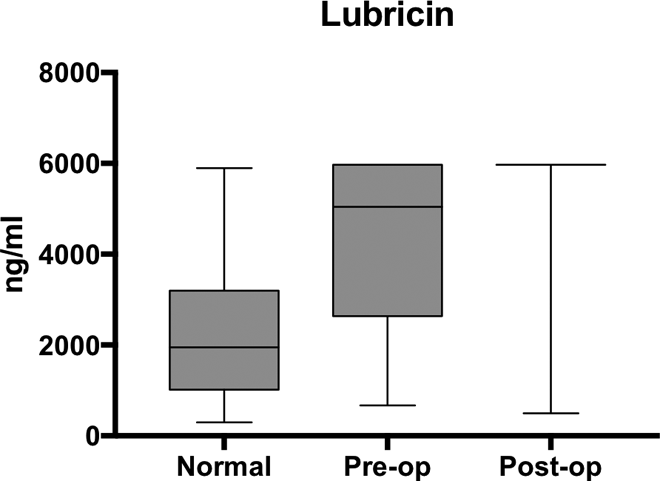
Box plot showing median levels of lubricin (proteoglycan-4) measured in control, preoperative, and postoperative groups. Boxes show interquartile ranges, and I bars demonstrate highest and lowest values. Preoperative versus control, P < .0001; postoperative versus control, P = .0011; and preoperative versus postoperative, P = .0001.
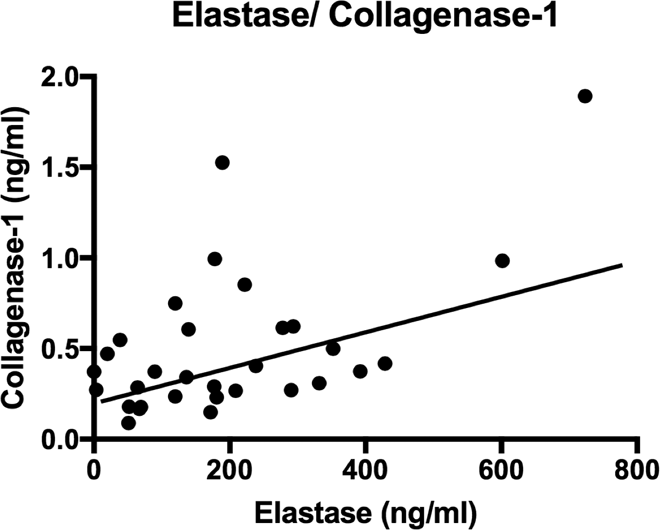
Scatter plot demonstrating the positive correlation of collagenase-1 and elastase as measured by the Spearman correlation coefficient in preoperative samples (P = .0129, r = .4415).
Discussion
Previous studies examining MDEs and their relevance to the pathogenesis of DJD have shown results consistent with those that have been observed here. 19 –21 These findings, in addition to previous data, provide evidence that patients with DJD have intrinsic abnormalities that may contribute to the pathogenesis of DJD. Although the popular belief that mechanical loading and shear force on weight-bearing joints is the major contributor to OA, the results of this study support the hypothesis that alterations in the levels of MDEs coupled with the changes in joint lubrication may contribute to osteoarthritic disease progression. There were increases in the measured levels of collagenase-1, elastase, and lubricin in patients with TJA. Although there was no significant difference in the heparanase levels, this does not exclude its importance in DJD.
In measuring elastase, there was a significant increase in patients with TJA compared to the healthy controls. Such a drastic difference provides evidence that there is dysregulation of elastase in patients who experience joint degeneration. Since elastase was previously noted to be increased during states of chronic inflammation, particularly that mediated by neutrophils, it was not surprising that patients who undergo TJA were found to have increased circulating levels of elastase. 12 This observation, coupled with the previous finding that elastase can degrade type III collagen, which is present in varying amounts in cartilage, supports the notion that elastase may have a catabolic function in the pathophysiology of DJD.
An increase in pre- and postoperative levels of collagenase-1 in comparison to healthy controls was observed. Although there was no significant difference between the preoperative and postoperative measurements, there was a positive correlation for patients with TJA (P = .0174, R = .3651). Since there are increased levels of collagenase-1 in patients undergoing TJA, this alludes to the potential role it plays in DJD. One of the major functions of collagenase-1 is to degrade type II collagen, which is the predominant type of collagen in cartilage. 8,22 Since the pathophysiology of OA is characterized by the breakdown of articular cartilage, the increased levels of collagenase-1 support the theory that there is intrinsic dysregulation of MDEs in DJD. 4
Circulating heparanase levels were not significantly different between the TJA patients and the healthy controls. It is possible that heparanase levels are only altered locally in the SF of the TJA patients. It may also be of interest to examine the functionality of heparanase in future studies to better interpret the role of heparanase in DJD. Heparanase levels were measured in this study by immunologic methods, which may not reflect its functionality in matrix degradation in DJD.
In these studies, the levels of various enzymes were measured in terms of their antigenic levels by using ELISA methods. Although the functional methods are available to measure the activity level of these enzymes, such as the zymographic methods for the collagenase-1 and elastase, such methods are relatively cumbersome and require a multistep preparative procedure. The antigenic levels of these enzymes are not subjected to any alterations in the protein content of these enzymes. However, prolonged storage may alter their functionality. This may be considered a limitation of this study; however, such an investigation will require validation of the functional methods in a larger sample size. Such studies in a larger population will be useful and provide supplementary data to our study. Regardless of this limitation, the observed changes in the antigenic level of the enzymes studied support our hypothesis regarding the pathogenic role of these proteins.
Lubricin levels have been measured previously in patients with TJA and have become of increased interest due to its lubricant properties. One study found that the levels of lubricin in SF of patients with OA was correlated with joint flexibility but not with arthritic pain. 23 Additionally, lubricin levels were found to be directly related to the degree of chondrocyte apoptosis. 24 Another study demonstrated that in a murine model, elastase was shown to degrade lubricin, 25 suggesting how interconnections between these enzymes may influence lubricin levels and functionality. Although many studies examine SF levels and this study examined lubricin in circulation, it is clear that lubricin is altered in patients with DJD compared to healthy individuals.
In this study, 10 of 30 preoperative samples exceeded the upper limits of detection, while 26 of 30 postoperative samples exceeded this limit (0 of 15 normal samples had exceeded the upper limit of detection). This supports the hypothesis that lubricin may leak out of joint capsule through the compromised synovium in patients with DJD. In the current studies, a commercially available assay for lubricin antigen levels was used. It would be of interest to validate our findings for the higher lubricin levels using additional methods. The next possible step would be to continue studying plasma samples while concomitantly testing the SF from patients undergoing TJA.
Finally, while examining possible interactions of the studied biomarkers, lubricin, and clinical parameters (eg, BMI, medication use, comorbidities, etc), it was found that a positive correlation existed between the preoperative levels of collagenase-1 and elastase (P = .0129, r = .4415). Interestingly, although a positive correlation was identified between these 2 enzymes preoperatively, there was no significant correlation in their postoperative levels (P = .235, r = .304). Further analysis of the data did not result in any significant correlation between these parameters. Therefore, because of the complex pathophysiology of this syndrome, these enzymes along with other mediators may be independently regulated.
Conclusion
It is not known whether the variations in MDE profiles have a primary influence on joint degradation or if it is secondary to other processes. It has been previously shown that patients with DJD have fibrinolytic dysregulation 26,27 and that individuals with OA have increased levels of plasmin in their cartilage. 28 This may be relevant to the current study as MMPs are regulated by specific TIMPs, which are regulated by enzymes from the serine- or cysteine-dependent protease family, such as plasmin. It may be that these patients’ fibrinolytic dysregulation holds a more important role in the pathophysiology of DJD than previously thought. Moving forward, if it is possible to correct the dysregulation of MDEs in patients with DJD, it may be possible to delay joint degeneration that eventually results in the need for arthroplasty.
Limitations
One of the major limitations of this study was the lack of age-matched controls for comparison. Control samples were collected from individuals who ranged in age from 18 to 35 years, while our patient population had a mean age of 64.9 years. This should not take away from the findings that patients with TJA have preexisting dysregulation of the coagulation and fibrinolytic systems. Future studies involving age-matched controls may build on the findings presented here.
Footnotes
Acknowledgments
The authors gratefully acknowledge the technical support from the staff of the hemostasis and thrombosis laboratories for facilitating the logistics of the blood collection, storage, and analysis of the samples included in this study. This research was a part of Students Training in Approaches to Research (STAR) program for medical students. The authors are thankful to Dr. Gail Hecht and Dean Linda Brubaker for their support and encouragement during this study. The authors are also thankful to Dr. Eva Wojick for providing support and resources to conduct this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.