
Abstract
We evaluated the diagnostic criteria for disseminated intravascular coagulation (DIC), which was published by the Japanese Society of Thrombosis and Hemostasis (JSTH), in 232 patients with suspected DIC without hematopoietic injury or infection. The diagnoses of the patients were as follows: DIC (n = 116), pre-DIC (n = 54), and non-DIC (n = 63). The efficacy of the diagnostic criteria for DIC was evaluated using a receiver operating characteristic analysis. The area under the curve and odds ratio for the global coagulation test (GCT) scores in the diagnosis of “DIC” were high, whereas those for the diagnosis of “DIC and pre-DIC” were low, suggesting that the addition of a reduced platelet count (RPC), antithrombin (AT), and soluble fibrin (SF)/thrombin AT (TAT) complex was required to diagnose DIC and pre-DIC. When the GCT score with the RPC, AT, and TAT/SF values was used, the cutoff DIC score for the diagnosis of DIC or DIC and pre-DIC was 6 points. For predicting the outcome, a scoring system that used the GCT result was useful, but the addition of RPC, AT, or SF/TAT was not. The modified diagnostic criteria of JSTH, which included the GCT score and the RPC, AT, and TAT/SF values, were useful for diagnosing both DIC and pre-DIC.
Introduction
The main underlying diseases of disseminated intravascular coagulation (DIC) include
1
–4
but are not limited to infectious diseases, hematologic malignancies, solid cancer, obstetric complications, and aneurysms. There are several pathophysiological states of DIC, including bleeding type, organ failure type, and asymptomatic type.
5
Thus, the diagnostic criteria established by the Japanese Ministry Health, Labor and Welfare (JMHLW) classified DIC based on the presence of hematopoietic injury.
6
The Japanese Society of Thrombosis and Hemostasis (JSTH) recently proposed a modified version of the JMHLW DIC criteria,
7
which includes hematopoietic injury type, infection type,
8
and basic type. The diagnostic criteria for DIC established by the JMHLW,
6
the International Society of Thrombosis and Haemostasis (ISTH),
9
and the Japanese Association for Acute Medicine (JAA)
10
are based on a scoring system that includes the results of global coagulation tests (GCTs), including the prothrombin time (PT), fibrinogen level, platelet count (PLT), and the levels of fibrin and fibrinogen degradation products (FDPs) and
Disseminated intravascular coagulation is reported to be associated with a high rate of mortality 11 –13 because of its association with severe organ failure and major bleeding. Thus, an early diagnosis and prompt treatment are required. 14 The ISTH Guidance for the diagnosis and treatment of DIC 15 recommends the use of a scoring system that uses GCT results to diagnose DIC. In the previous evaluation of the 3 diagnostic criteria, 16 the JAA diagnostic criteria displayed high sensitivity but low specificity, whereas the ISTH overt DIC diagnostic criteria displayed high specificity but low sensitivity in the diagnosis of DIC. Given that the 3 diagnostic criteria used similar GCTs, their diagnostic abilities might be similar, suggesting that the ability to diagnose DIC by GCT results alone may be limited.
An evaluation of the efficacy of DIC treatment in relation to the JMHLW DIC score at the beginning of treatment 17 suggests that the early diagnosis and treatment of DIC are essential for improving the prognosis of DIC patients. It is necessary to measure the changes in the GCTs and the hemostatic molecular markers such as plasmin–plasmin inhibitor complex, antithrombin (AT), soluble fibrin (SF), and thrombin AT (TAT) complex for diagnosing the disease state within 7 days before the onset of DIC, which is considered to be pre-DIC. 17 Although the diagnostic criteria for nonovert DIC have been proposed by the ISTH subcommittee and several researchers, 18 –21 the criteria for diagnosing early-phase DIC have not been sufficiently established.
In the present study, this scoring system was evaluated in the diagnosis of the basic type of DIC. Table 1 shows the JSTH DIC criteria for the basic type of DIC.
The Diagnostic Criteria for the Basic Type of DIC (Without Infection or Hematopoietic Injuries) Established by the Japanese Society of Thrombosis and Hemostasis.
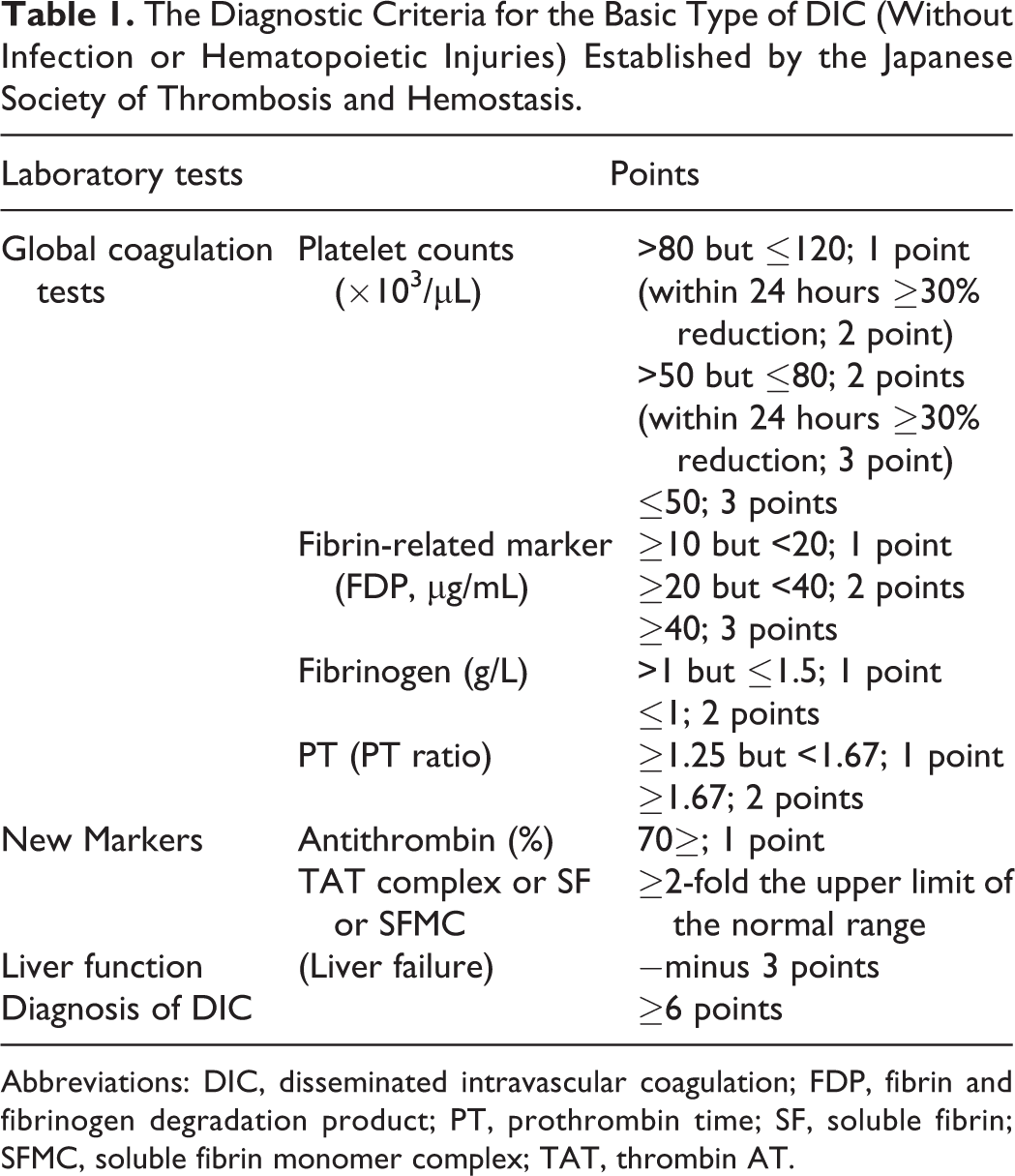
Abbreviations: DIC, disseminated intravascular coagulation; FDP, fibrin and fibrinogen degradation product; PT, prothrombin time; SF, soluble fibrin; SFMC, soluble fibrin monomer complex; TAT, thrombin AT.
Materials and Methods
Total of 519 patients with suspected DIC from January 1, 1989, to December 31, 2014, were included in the present study. After excluding 232 patients with hematopoietic injury and 108 patients with infection, 179 patients remained and were included in the present study (Figure 1). One hundred sixteen patients were diagnosed according to the JMHLW diagnostic criteria. 6 It was possible to determine the presence of hemostatic abnormalities within 7 days before the onset of DIC in 54 patients; these were considered to be the pre-DIC cases, 17 and 63 patients did not develop DIC during their clinical course (non-DIC; Table 2). The underlying diseases of the patients in the study population included stomach cancer (n = 32), lung cancer (n = 27), liver cancer (n = 9), pancreatic cancer (n = 6), bile duct cancer (n = 6), origin unknown cancer (n = 5), breast cancer (n = 5), prostate cancer (n = 5), other cancers (n = 19), organ failure (n = 24), obstetrics diseases (n = 7), trauma (n = 6), and others (n = 28).
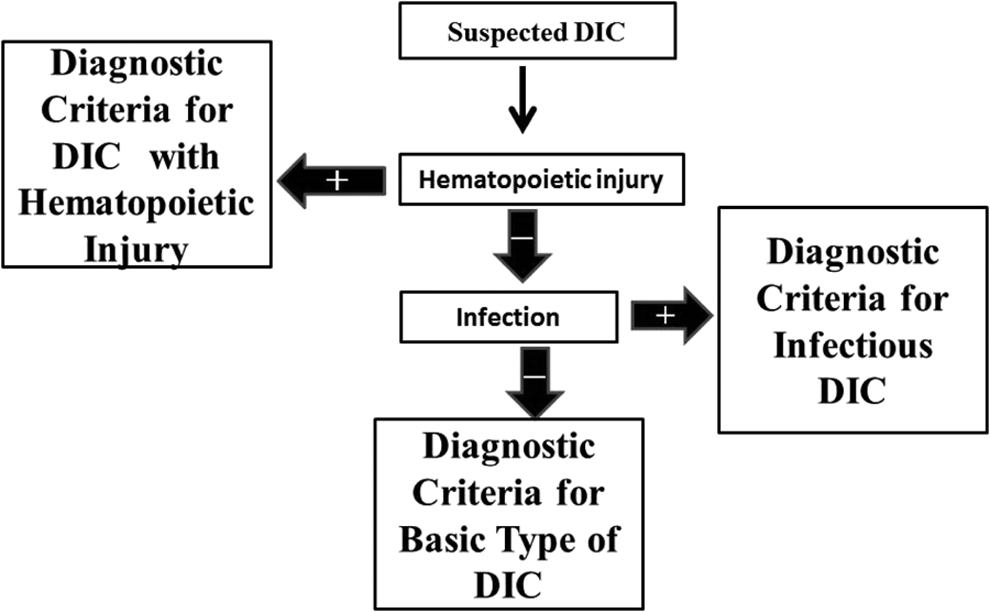
The protocol of the Japanese Society of Thrombosis and Hemostasis for the diagnosis of DIC. DIC indicates disseminated intravascular coagulation.
Participants.a
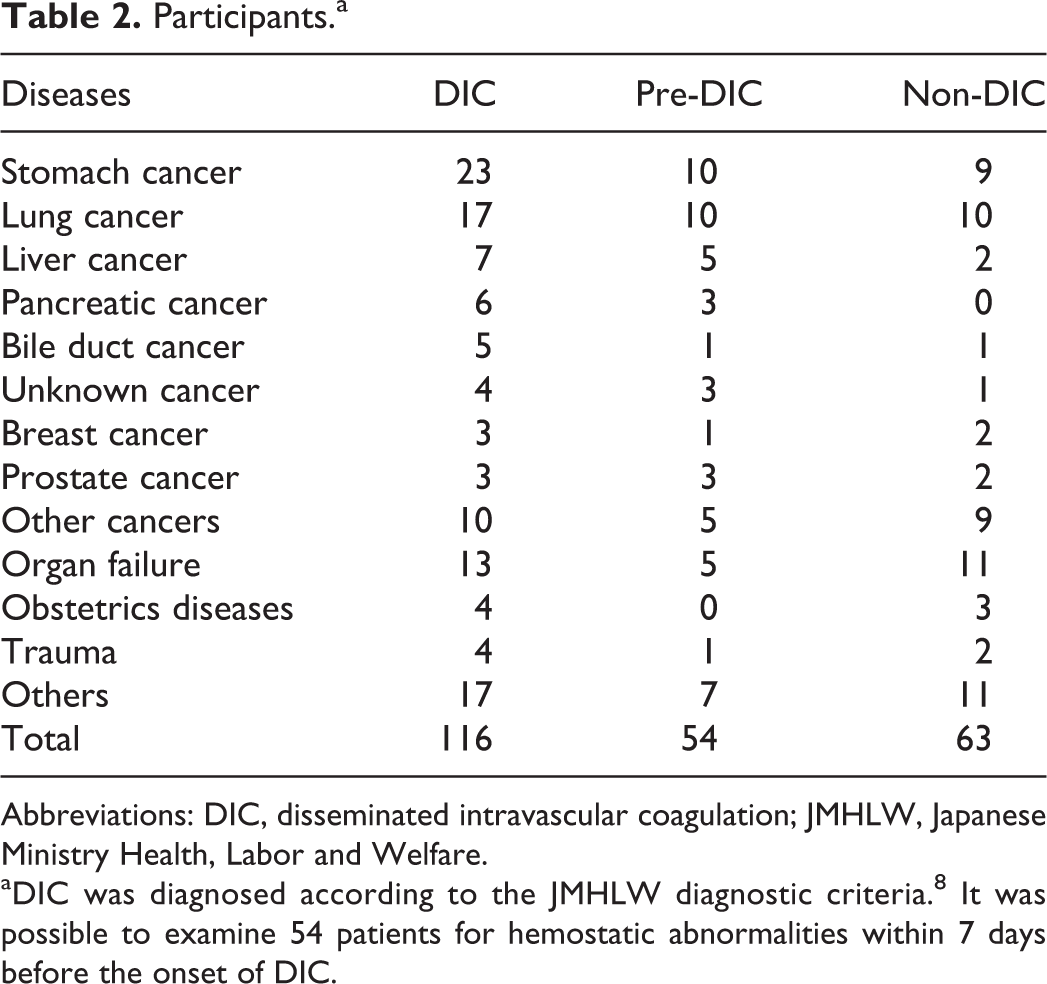
Abbreviations: DIC, disseminated intravascular coagulation; JMHLW, Japanese Ministry Health, Labor and Welfare.
aDIC was diagnosed according to the JMHLW diagnostic criteria. 8 It was possible to examine 54 patients for hemostatic abnormalities within 7 days before the onset of DIC.
The study protocol was approved by the Human Ethics Review Committee of the Mie University School of Medicine, and the study was carried out in accordance with the principles of the Declaration of Helsinki. The cases in which 1 or more of the following laboratory findings were present were included in the following study: an FDP value of ≥10 μg/mL, a fibrinogen level of ≤1 g/L, and a PT ratio of ≤1.25. The mortality rate was calculated as the number of death within 28 days after the registration/the total number of each group. The resolution was evaluated by each of the diagnostic criteria for DIC 14 days after the diagnosis of DIC.
The PT, fibrinogen,
Statistical Analysis
The data are expressed as the median (25th to 75th percentile). The Mann-Whitney U test was used to test for the statistical significance of differences between groups. The efficacy of the DIC diagnostic criteria was evaluated by a receiver operating characteristic (ROC) analysis. P values of ≤.05 were considered to indicate statistical significance. All of the statistical analyses were performed using the Stat Flex, a software program (version 6; Artec Co Ltd, Osaka, Japan).
Results
No significant differences were observed in the age or sex of the patients with DIC, pre-DIC, and non-DIC (as diagnosed by the JMHLW DIC diagnostic criteria; Table 3). The mortality rate of the DIC (62.9%) and pre-DIC (64.8%) patients was higher than that of the non-DIC (27.0%) patients. The resolution rate from the DIC group was similar to that from the DIC (42.2%) and pre-DIC groups (40.7%). The JMHLW, ISTH, and JAA DIC scores of the patients with DIC were significantly higher than those with pre-DIC and non-DIC. No difference was observed between pre-DIC and non-DIC. The hemostatic marker levels are shown in Table 4. The PT ratio, PLT, FDP, fibrinogen, and AT values of the DIC patients differed significantly from those of the pre-DIC and non-DIC patients, and the TAT level and the degree of SF elevation of the DIC patients differed from those of the non-DIC patients. The PT ratio, PLT, fibrinogen, and TAT values of the pre-DIC patients differed from those of the DIC patients. The evaluation of each scoring system was carried out by an ROC analysis (Figure 2), and the cutoff DIC score was decided according to the point of intersection between the sensitivity curve and the “1 − specificity” curve.
DIC, Pre-DIC, and Non-DIC, as Diagnosed by the JMHLW Diagnostic Criteria.
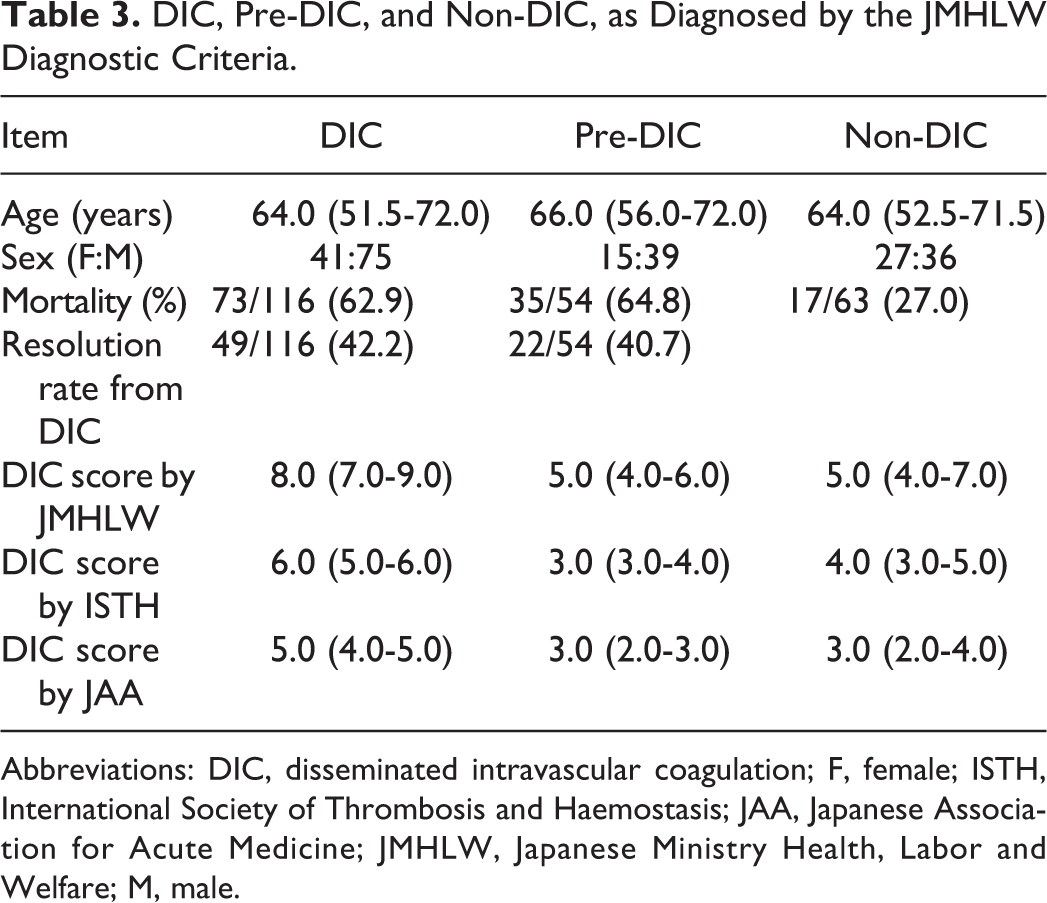
Abbreviations: DIC, disseminated intravascular coagulation; F, female; ISTH, International Society of Thrombosis and Haemostasis; JAA, Japanese Association for Acute Medicine; JMHLW, Japanese Ministry Health, Labor and Welfare; M, male.
The Hemostatic Marker Levels in Patients With DIC, Pre-DIC, and Non-DIC.
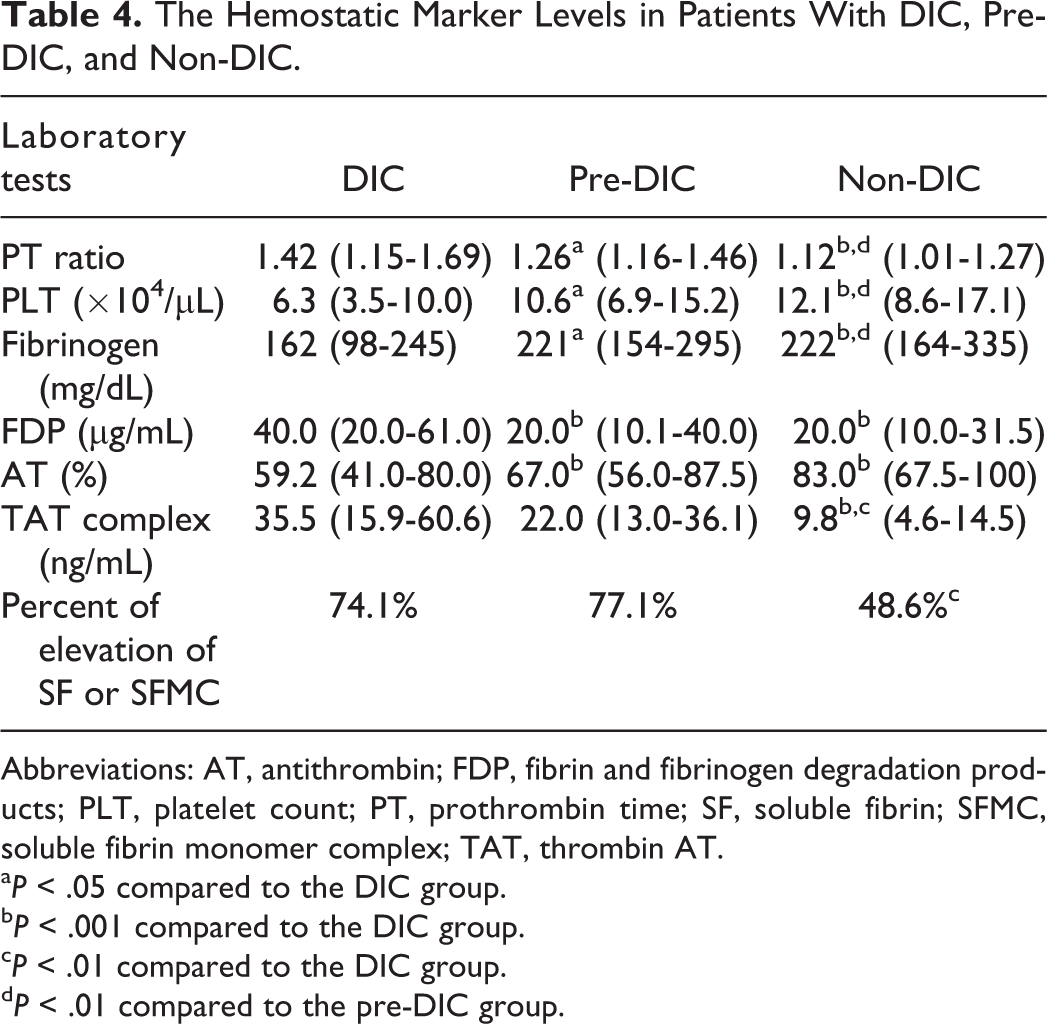
Abbreviations: AT, antithrombin; FDP, fibrin and fibrinogen degradation products; PLT, platelet count; PT, prothrombin time; SF, soluble fibrin; SFMC, soluble fibrin monomer complex; TAT, thrombin AT.
a P < .05 compared to the DIC group.
b P < .001 compared to the DIC group.
c P < .01 compared to the DIC group.
d P < .01 compared to the pre-DIC group.
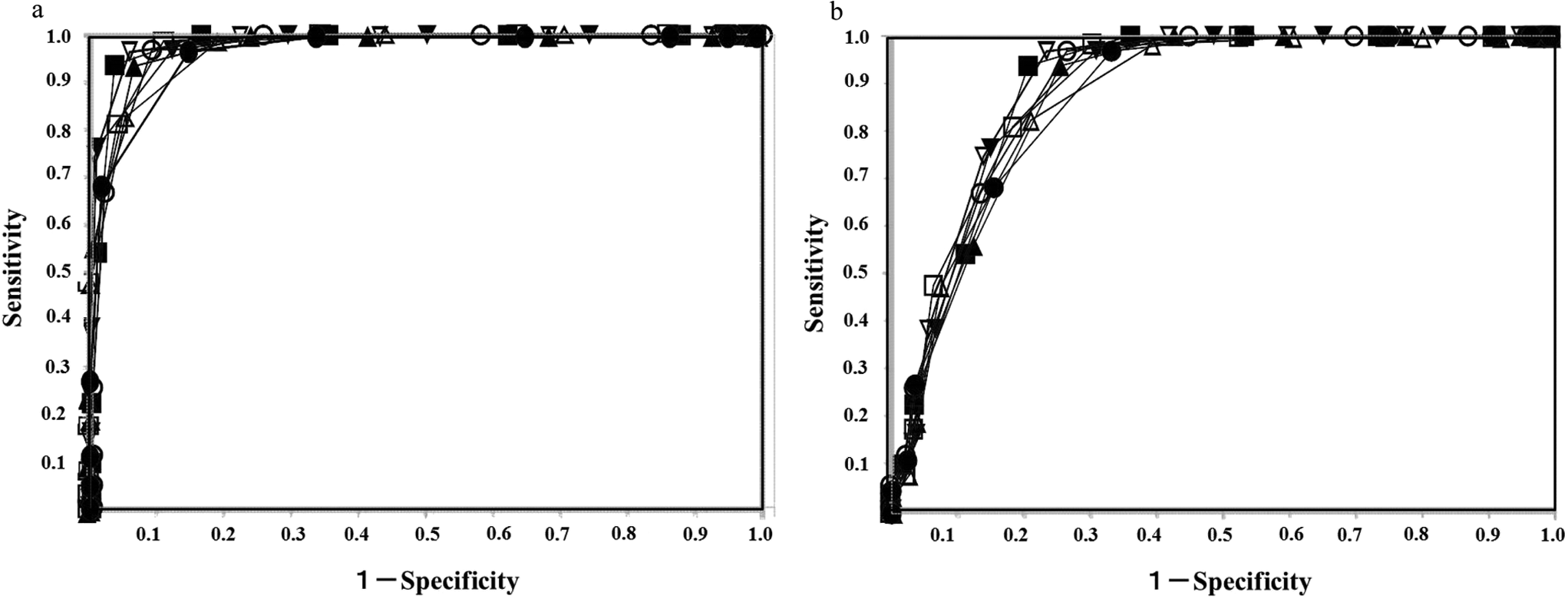
The receiver operating characteristic (ROC) analysis for disseminated intravascular coagulation (DIC) without pre-DIC (A) and for DIC with pre-DIC (B). Closed circles, global coagulation test (GCT); open circles, GCT + reduced platelet count; closed triangles, GCT + antithrombin (AT); open triangles, GCT + soluble fibrin (SF)/thrombin AT (TAT) complex; closed square, GCT + reduced platelet count + AT; open square, GCT + reduced platelet count + SF/TAT; closed reversed triangles, GCT + AT + SF/TAT; open reversed triangles, GCT + reduced platelet count + AT + SF/TAT.
In the diagnosis of DIC versus non-DIC (Table 5), the cutoff DIC score for “GCT,” “GCT + reduced platelet,” “GCT + AT,” and “GCT + reduced platelet + AT” was 5, whereas that for “GCT + SF/TAT,” “GCT + reduced platelet + SF/TAT”, “GCT + AT + SF/TAT,” and “GCT + reduced platelet + AT + SF/TAT” was 6 (Table 5). The lowest area under the curve (AUC) value was 0.965 in GCT and the highest AUC value was 0.987 in GCT + reduced platelet + AT and GCT + reduced platelet +AT + SF/TAT (Figure 2A). GCT and GCT + reduced platelet + AT + SF/TAT showed the lowest and highest odds ratios, respectively (177 and 1137).
The Relationship Between the Diagnostic Scoring System and the Ability to Diagnose DIC Without Pre-DIC Versus Non-DIC.
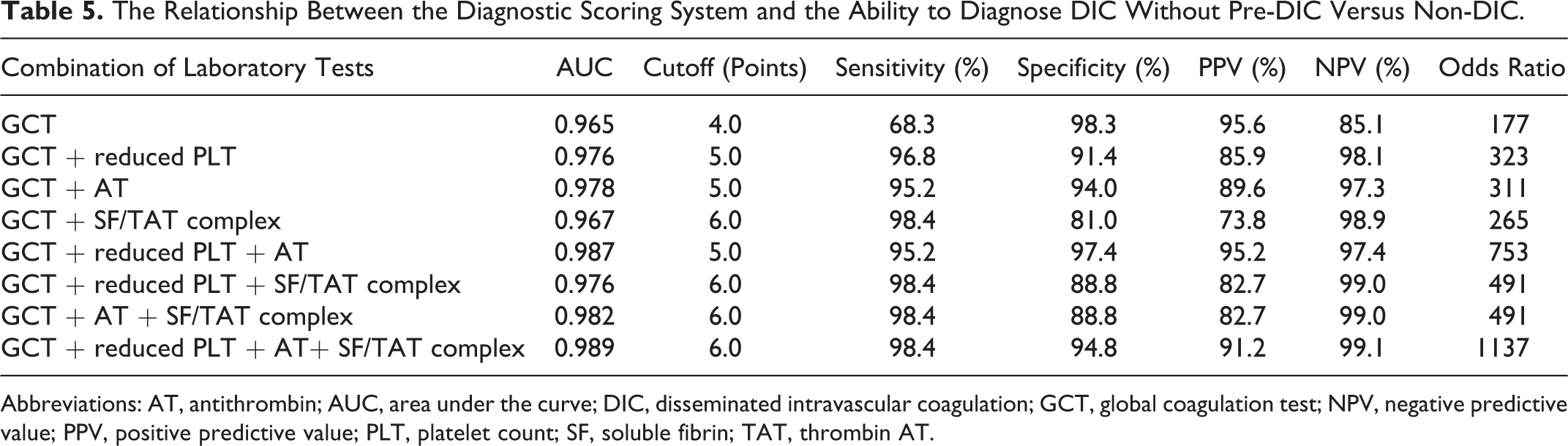
Abbreviations: AT, antithrombin; AUC, area under the curve; DIC, disseminated intravascular coagulation; GCT, global coagulation test; NPV, negative predictive value; PPV, positive predictive value; PLT, platelet count; SF, soluble fibrin; TAT, thrombin AT.
In the diagnosis of DIC and pre-DIC (Table 6), the cutoff DIC score for DIC and pre-DIC was the same as that for DIC. The lowest AUC value was 0.872 in GCT, while the highest AUC value was 0.903 in GCT + reduced platelet + AT + SF/TAT (Figure 2B). GCT + reduced platelet + SF/TAT and GCT + reduced platelet + AT + SF/TAT showed the lowest and highest odds ratios, respectively (61.5 and 237). Both the AUC value and the odds ratio were higher in the diagnosis of DIC than in the diagnoses of DIC and pre-DIC.
The Relationship Between the Diagnostic Scoring System and the Ability to Diagnose DIC With Pre-DIC Versus Non-DIC.
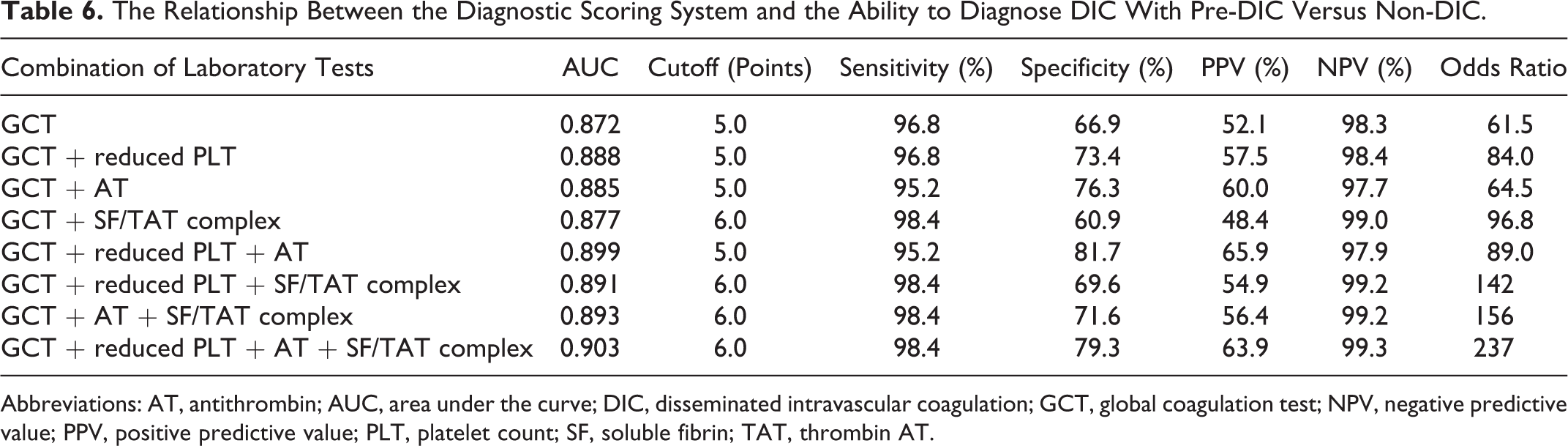
Abbreviations: AT, antithrombin; AUC, area under the curve; DIC, disseminated intravascular coagulation; GCT, global coagulation test; NPV, negative predictive value; PPV, positive predictive value; PLT, platelet count; SF, soluble fibrin; TAT, thrombin AT.
With regard to the relationship between the diagnostic score and outcome in all patients (Figure 3), the odds ratio and AUC values were low in all of the scoring systems (2.17-3.30 and 0.604-0.646, respectively; Table 7). The cutoff values of the scoring system for the outcome were similar to those for diagnosing DIC or “DIC + pre-DIC.”
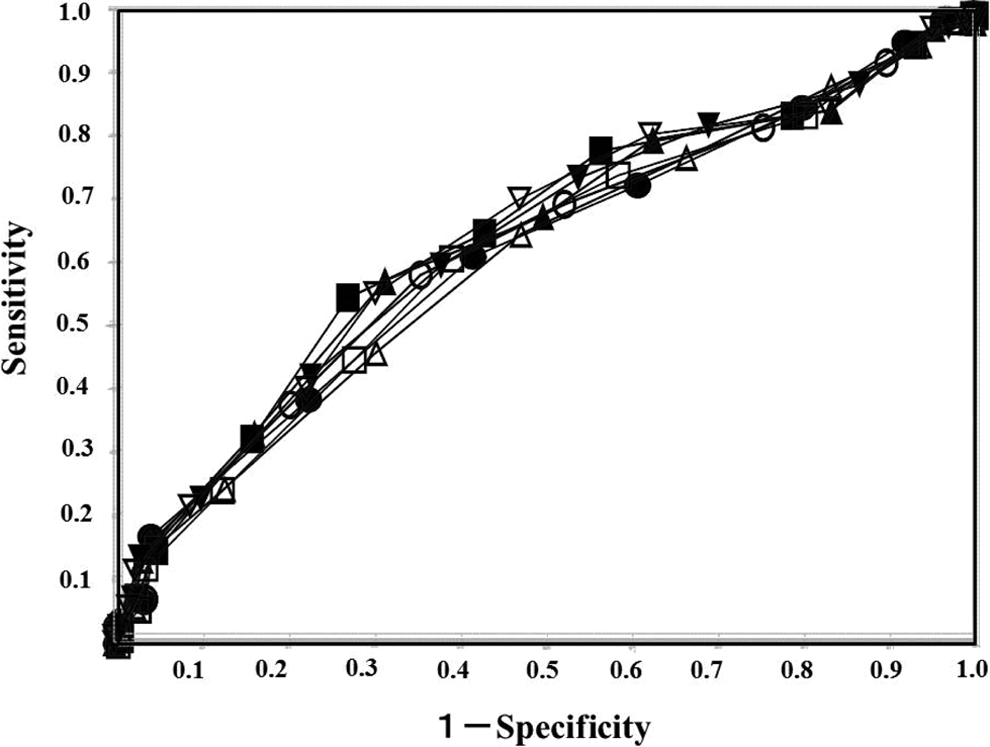
The receiver operating characteristic (ROC) analysis for the outcome in all patients. Closed circles, global coagulation test (GCT); open circles, GCT + reduced platelet count; closed triangles, GCT + antithrombin (AT); open triangles, GCT + soluble fibrin (SF)/thrombin AT (TAT) complex; closed squares, GCT + reduced platelet count + AT; open squares, GCT + reduced platelet count + SF/TAT; closed reversed triangles, GCT + AT + SF/TAT; open reversed triangles, GCT + reduced platelet count + AT + SF/TAT.
The Relationship Between the Diagnostic Scoring System and the Predicted Outcome in All Patients.
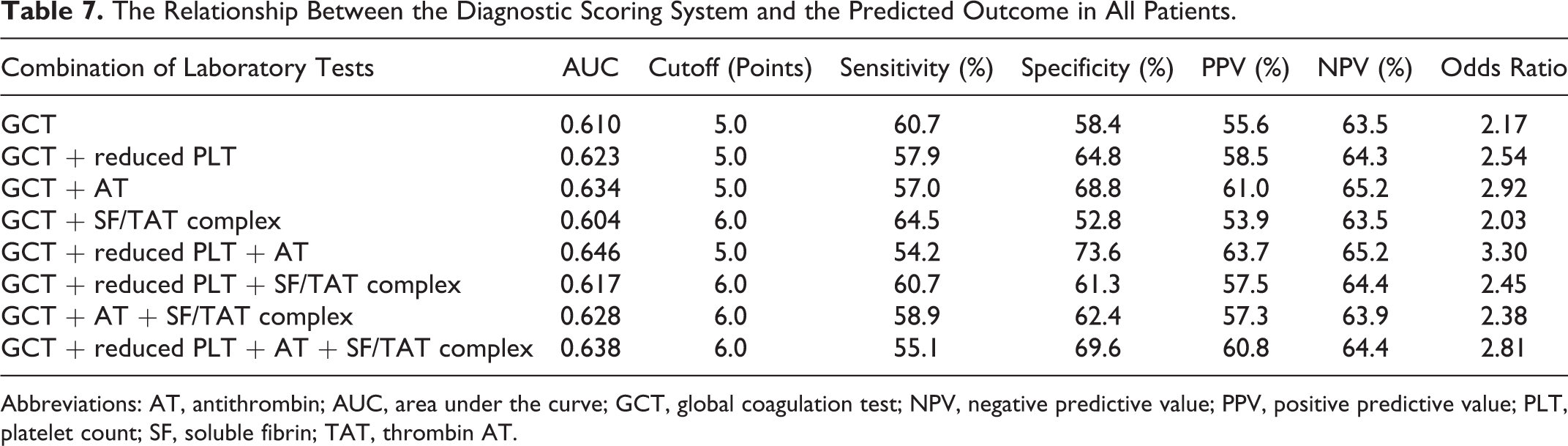
Abbreviations: AT, antithrombin; AUC, area under the curve; GCT, global coagulation test; NPV, negative predictive value; PPV, positive predictive value; PLT, platelet count; SF, soluble fibrin; TAT, thrombin AT.
Discussion
Although many studies have reported the usefulness of the diagnostic criteria for infectious diseases 10,22 or hematological malignancies, 14,22 few reports have evaluated the diagnostic criteria for other diseases. The outcome of diseases other than infection and hematological malignancies is also poor. 14,23 Although the outcome of DIC was improved by treatment in the early stage of the disease (such as pre-DIC), 14 the early administration of anticoagulants to patients with infectious diseases might lead to the spread of infection in patients with sepsis. 24 Several reports 21,22 refer to the state within 1 week before the onset of DIC as pre-DIC, and we therefore used this definition in the present study. The PT ratio, PLT, fibrinogen, and TAT levels in patients with pre-DIC were significantly different from those with non-DIC, suggesting that these markers might be useful for the diagnosis of pre-DIC in cases that involve the basic type of DIC. All of the parameters in the patients with DIC were significantly different from those with non-DIC. The ISTH guidance for the diagnosis and treatment of DIC recommends that DIC be diagnosed by a scoring system rather than by a single marker. 15
The ROC analysis revealed 4 cutoff values for the GCT score, high AUC, and specificity; however, the sensitivity and odds ratio were low. The addition of a reduced platelet count (RPC), AT, and SF/TAT resulted in 6 cutoff values and increased the AUC, sensitivity, and odds ratio, suggesting that the combination of a RPC, the hemostatic molecular marker levels, and GCT results increased the sensitivity and specificity in the diagnosis of DIC. In contrast, in the evaluation for the diagnosis of DIC + pre-DIC, both the AUC and odds ratio were lower in comparison with DIC. The addition of an RPC, AT, and SF/TAT improved the ability to diagnose DIC + pre-DIC. These findings show that the modified JMHLW diagnostic criteria for DIC, which use the GCT score, RPC, and the hemostatic molecular marker levels, can be used to diagnose both overt DIC and pre-DIC in patients in whom basic type DIC was suspected. Many patients with solid cancer were included in this study. Solid carcinoma is usually complicated with DIC after it progresses, resulting in a high mortality rate among these patients.
With regard to the relationship between the diagnostic score and the outcome in the whole study population, the odds ratio and AUC were low in all of the scoring systems, suggesting that the mortality rates of patients with DIC or pre-DIC were too high in the present study. A previous study reported that the odds of mortality in DIC patients and non-DIC patients were similar (2.63). 25
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a Grant-in-Aid from the Ministry of Health, Labour and Welfare of Japan for Blood Coagulation Abnormalities and from the Ministry of Education, Culture, Sports, Science and Technology of Japan.