
Abstract
Introduction:
There are limited studies evaluating the ability of the Hestia criteria to accurately identify patients with acute pulmonary embolism (PE) at low risk of early mortality. We sought to externally validate the Hestia criteria for predicting in-hospital and 30-day post-PE mortality.
Methods:
We retrospectively identified consecutive, adult, objectively confirmed PE patients presenting to the emergency department at our institution from November 21, 2010, to January 31, 2014. We ascertained the total number of Hestia criteria met for each patient, calculated the proportion of patients categorized as low risk (ie, no Hestia criteria met), and determined the accuracy of the Hestia criteria for predicting in-hospital and 30-day all-cause mortality. Mortality was determined through Social Security Death Index searches.
Results:
A total of 577 patients with PE were included, of which 19 (3.3%) and 35 (6.6%) died in hospital or within 30 days of presentation. Both in-hospital and 30-day case fatality rates rose as the number of Hestia criteria increased. One-hundred forty nine (25.8%) patients were classified as low risk for early mortality, and none of these patients died within 30 days (negative predictive values of 100%). The Hestia criteria had excellent sensitivity (100%, 95% confidence interval [CI] = 79.1%-100% and 100%, 95% CI = 87.7%-100%) for predicting in-hospital and 30-day mortality but low specificity (<27.5% for both). The c-statistics for in-hospital and 30-day mortality were 83.5%, 95% CI = 77.1%-89.9% and 78.5%, 95% CI = 71.9%-85.1%. The predictive accuracy of the Hestia criteria remained acceptable in patients >80 years of age, with active cancer or chronic cardiopulmonary disease.
Conclusion:
The Hestia criteria have an acceptable predictive accuracy to identify patients with PE at low risk for in-hospital or 30-day mortality.
Introduction
Guidelines suggest that patients with pulmonary embolism (PE) who are identified to have a low risk of early mortality may be candidates for treatment without admission to the hospital (ie, discharge from the emergency department) or with hospital admission and early discharge. 1,2 Data from randomized trials and observational studies suggest that treating appropriately selected patients with acute PE at home does not increase early mortality, recurrent venous thromboembolism, or bleeding risk. 3,4
As part of a large prospective derivation study performed in the Netherlands, the Hestia criteria (consisting of 11 vital sign, laboratory and clinical risk factors) were shown to have high sensitivity and negative predictive value (NPV) for identifying low-risk patients with PE. 5 However, a paucity of studies externally validating the Hestia criteria have been published. The goal of this study was to externally validate the Hestia criteria for predicting in-hospital and 30-day post-PE mortality.
Methods
Preparation of this study report was in accordance with the Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD) statement. 6
For this retrospective cohort study, we identified consecutive patients diagnosed with acute PE between October 21, 2010, and January 31, 2014, using computerized billing records for admissions to Hartford Hospital (Hartford, Connecticut). The hospital’s computerized billing system contains information on demographic characteristics (age, gender, race), source of admission, International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis and procedure codes, admission and discharge dates, and discharge status. To be eligible for inclusion into this study, patients had to be ≥18 years of age, present to our institution through the emergency department, and have a primary diagnosis of PE (ICD-9-CM code = 415.1x). Consistent with prior studies, we excluded patients lacking objective confirmation of acute PE according to clinical guidelines. 5,7 The following were considered confirmatory studies for the diagnosis of acute PE: high-probability perfusion–ventilation lung scan (V/Q scan), computed tomography pulmonary angiography (CTPA) or pulmonary angiography diagnostic for PE, or a nondiagnostic V/Q scan or CTPA in combination with an abnormal compression ultrasonography of the lower extremities. 1,2 All patients included in this study were managed according to usual clinical practice for our institution.
While no formal sample size calculation was performed, prior to starting this analysis we queried the electronic health record (EHR; starting from the date of its implementation) and billing systems at our institution and determined the number of evaluable patients for this analysis would be similar to that of the original Hestia criteria derivation study. 5
Risk stratification of patients with acute PE using the Hestia criteria were performed according to published methods (Appendix A). 5 Patients meeting none of the Hestia criteria were classified as low risk for early mortality. Data necessary to classify patients as low- or high risk of early mortality according to Hestia were obtained by linking all included patients identified through the billing system to the hospital’s EHR. We used vital signs (heart rate [HR], blood pressure [BP], oxygen [O2] saturation) and laboratory values (serum creatinine, platelet count) obtained as close to the time of emergency department presentation as possible (but within 24 h). The presence of cancer, cardiopulmonary disease, severe liver disease (defined as diagnosed cirrhosis), heparin-induced thrombocytopenia, need for intravenous pain medication, medical/social reason for treatment in hospital, and recent clinical events (gastrointestinal bleeding within 14 days, stroke with 4 weeks, surgery with 2 weeks) were assessed at time of departure from the emergency department. Missing vitals were assumed to be normal. All data for this study were abstracted by trained study personnel.
All-cause, in-hospital, and 30-day post-PE mortality served as a priori end points for this study. In-hospital mortality was determined using the discharge status field for the index admission within the hospital billing system and EHR. Thirty-day mortality was based upon searches of the Social Security Death Index (SSDI) 8 performed >1 year after the last day of eligible inclusion.
Baseline characteristics are described with means ± standard deviations (SDs) for continuous data and counts and proportions for categorical data. We ascertained the total number of Hestia criteria met for each patient; calculated the proportion of patients categorized as low risk; and determined the sensitivity, specificity, NPV, and positive predictive value (PPV) of the Hestia criteria along with 95% confidence intervals (CIs) for prognosticating early mortality. Overall discriminative power of the Hestia criteria was assessed using the c-statistic. In addition to analyses in the total population, we also evaluated the predictive accuracy of the Hestia criteria in patients stratified as >80 years of age, those with active cancer (defined as cancer under the care of an oncologist or known metastatic disease), and cardiopulmonary disease (ie, presence of chronic lung disease or heart failure). These subgroups were chosen as they have been included in other clinical prediction rules for PE mortality 7,9,10 but are not explicitly part of the Hestia criteria. 5 All database management and statistical analyses were performed using IBM SPSS Statistics version 22.0 (IBM Corp, Armonk, New York). The study was approved by the Hartford Hospital institutional review board with a waiver of informed consent.
Results
A total of 603 patients with a primary ICD-9-CM code for acute PE and objective confirmation of diagnosis were identified. Of these, 26 were not seen in our institution’s emergency department, leaving 577 for analysis. Baseline characteristics of the cohort, stratified by low- and high risk per the Hestia criteria, are depicted in Table 1.
Characteristics of Pulmonary Embolism Patients.
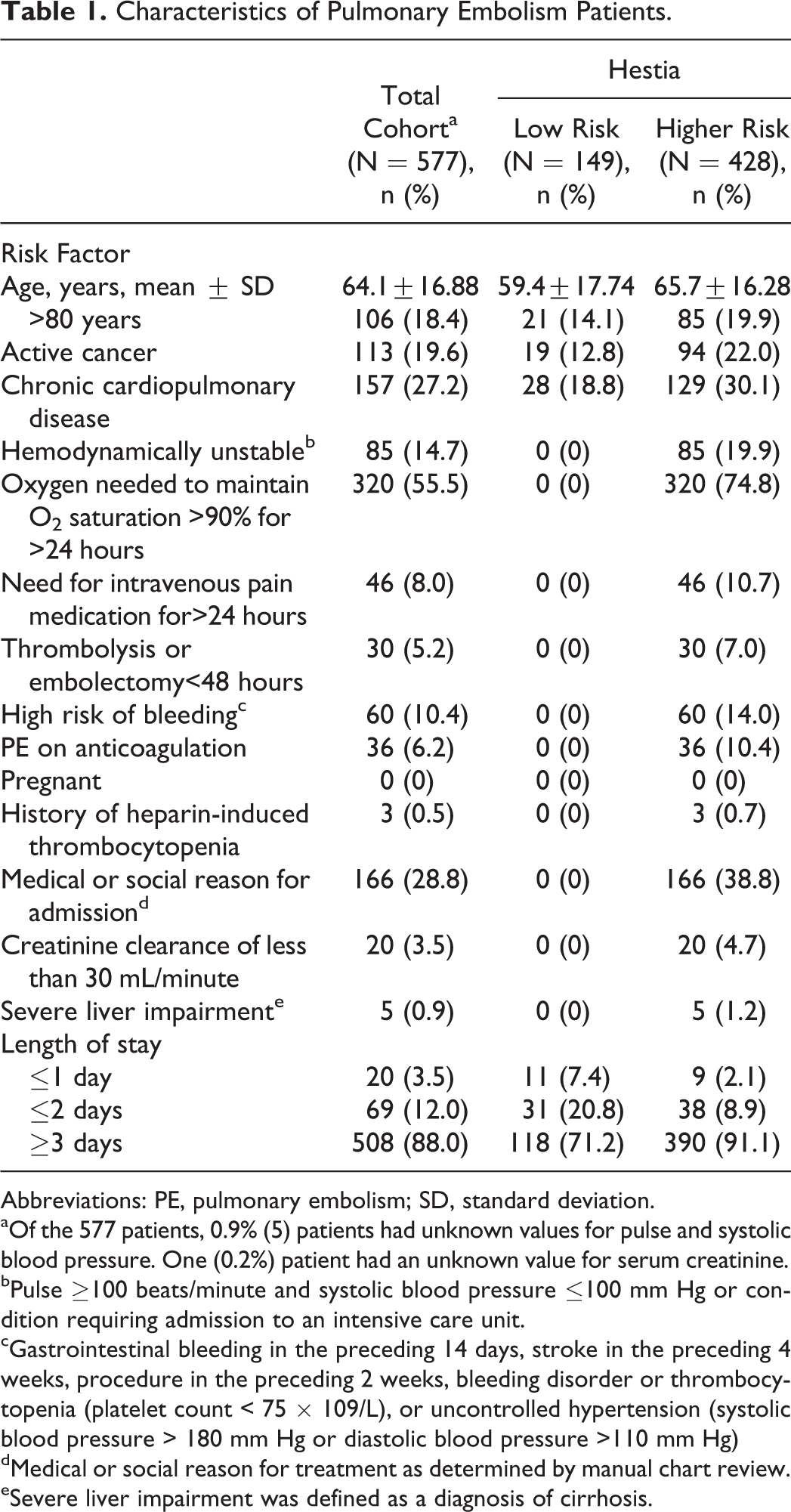
Abbreviations: PE, pulmonary embolism; SD, standard deviation.
aOf the 577 patients, 0.9% (5) patients had unknown values for pulse and systolic blood pressure. One (0.2%) patient had an unknown value for serum creatinine.
bPulse ≥100 beats/minute and systolic blood pressure ≤100 mm Hg or condition requiring admission to an intensive care unit.
cGastrointestinal bleeding in the preceding 14 days, stroke in the preceding 4 weeks, procedure in the preceding 2 weeks, bleeding disorder or thrombocytopenia (platelet count < 75 × 109/L), or uncontrolled hypertension (systolic blood pressure > 180 mm Hg or diastolic blood pressure >110 mm Hg)
dMedical or social reason for treatment as determined by manual chart review.
eSevere liver impairment was defined as a diagnosis of cirrhosis.
Of the 577 included patients with PE, 19 (3.3%) died in hospital and 35 (6.6%) died within 30 days of presentation to the emergency department (Table 2). Most patients were not treated as outpatients or with an abbreviated hospital admission as evidenced by 88% of patients having a length of stay ≥3 days. The rate of in-hospital mortality rose as an increasing number of Hestia criteria were met (0 criteria = 0%, 1 = 0.5%, 2 = 6.4%, 3 = 10.6%, and >3 = 13.2%). Thirty-day mortality also rose as an increasing number of Hestia criteria were met (0 criteria = 0%, 1 = 3.2%, 2 = 9.5%, 3 = 17.0%, and >3 = 21.1%). About one-quarter of patients (n = 149, 25.8%) were classified as low risk for early mortality. None of these low-risk patients died within 30 days, resulting in the Hestia criteria having NPVs of 100% for both mortality time points (Table 3). The Hestia criteria had excellent sensitivity (100% and 100%) but low specificity (26.7% and 27.5%) for predicting in-hospital and 30-day mortality. The PPVs for the Hestia criteria were low (<8.2% for both mortality time points). The c-statistics for in-hospital and 30-day mortality derived from Hestia risk category distributions were 83.5% and 78.5% (Figure 1). The Hestia criteria classified 19.8%, 16.8%, and 17.8% of patients with PE >80 years of age, with active cancer or chronic cardiopulmonary disease, as low risk. The Hestia criteria’s sensitivity and NPV for identifying patients at low risk of early mortality remained high among each of these subsets of patients.
In-Hospital and 30-Day Mortality Within Risk Strata Derived From the Hestia Criteria.
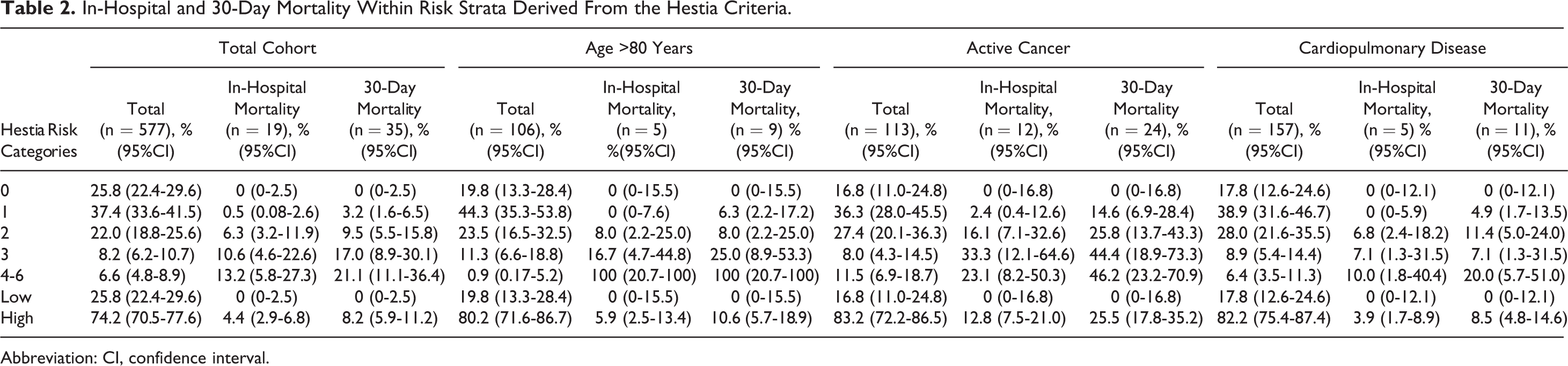
Abbreviation: CI, confidence interval.
Hestia Criteria Test Characteristics for In-Hospital and 30-Day Mortality.
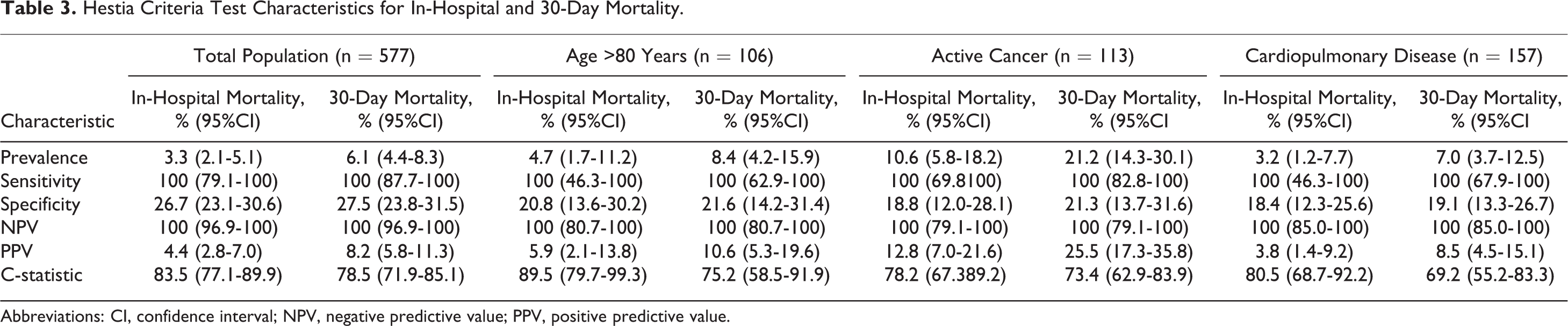
Abbreviations: CI, confidence interval; NPV, negative predictive value; PPV, positive predictive value.
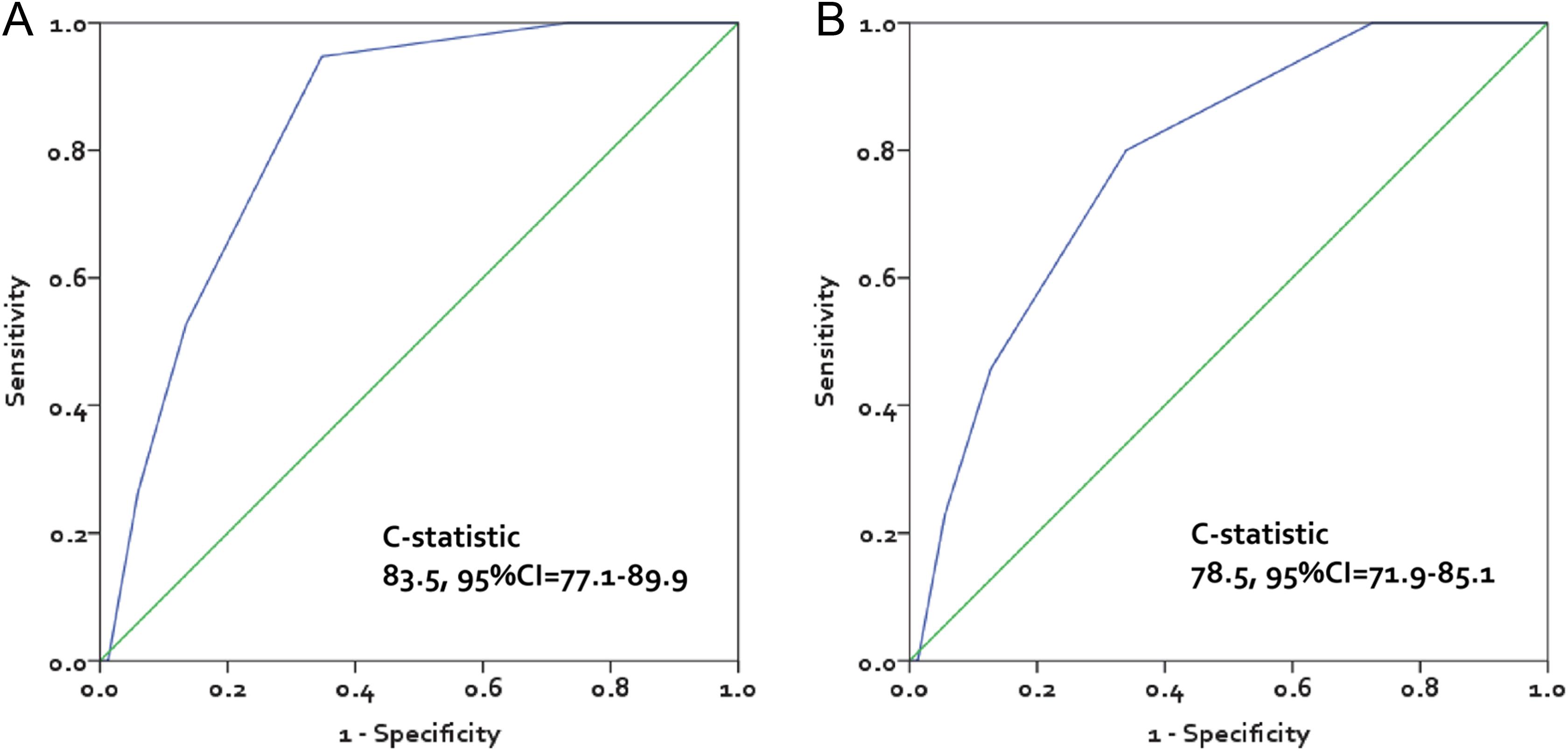
Receiver–operator characteristic curves panel A reflects in-hospital mortality and panel B reflects 30-day mortality. CI indicates confidence interval.
Discussion
Acute PE treatment guidelines support early discharge and/or home treatment of PE patients at low risk of early mortality as long as they have adequate home support. 1,2 The Hestia criteria classified ∼26% of patients with acute PE in our study as low risk and exhibited sensitivity and NPVs of 100% for both in-hospital and 30-day all-cause mortality. These results suggest the Hestia criteria can adequately identify a cohort of low-risk patients with PE who are unlikely to die within the first 30 days of emergency department presentation. However, because a minority of patients with acute PE (6.1% in our study) die within 30 days of presentation, the Hestia criteria classifies a substantial number of patients who ultimately survive into the high-risk group (hence, the low specificity observed in this analysis). Predictive tests rarely have both high sensitivity and specificity. When using a predictive test to support the use of a less conservative treatment strategy such as discharging a patient with PE home early or directly from the emergency department, high sensitivity and NPV values are preferable test characteristics.
Our estimates of the Hestia criteria’s sensitivity and NPV as well as the c-statistic for predicting 30-day all-cause mortality were somewhat higher than those observed in the original derivation study (sensitivity = 82%, 95% CI = 48%-97%; NPV = 99%, 95% CI = 97%-100%, c-statistics = 67.9%, 95% CI = 53.6%-82.2%). 5 Perhaps, the most notable difference between the Hestia derivation study and our own is in the proportion of patients with PE classified as low risk (25.8% in this study vs 51% in the Hestia derivation). Our smaller proportion of patients with acute PE categorized as low risk may be partially explained by the patient population which included a larger proportion with cardiopulmonary disease (27.2% vs 9.4%) or active cancer (19.6% vs 14.3%), requiring O2 supplementation to maintain O2 saturation >90% (55.5% vs 13.8%) or at high risk of bleeding (10.4% vs 2.6%). Additionally, the Hestia criteria derivation study’s methods (ie, predefined inclusion/exclusion criteria and need for informed consent) may have also contributed to the selection of a healthier, less generalizable study population. 5 Interestingly, a recent study by Werth and colleagues 11 which risk stratified 439 patients with acute PE with the Hestia criteria found 148 (33.7%) had score of 0, representing a low-risk population estimate more in line with our own. These studies taken together may suggest that retrospective scoring of Hestia may result in the classification of smaller proportions of patients as low risk (despite missing laboratory values being assumed to be within normal limits).
Unlike other clinical rules used for predicting early post-PE mortality, 7 the Hestia criteria do not (at least directly) classify patients of advanced age or those with chronic cardiopulmonary disease or active cancer as being high risk for early mortality. When we evaluated the predictive accuracy of the Hestia criteria in each of these patient subsets, we found the Hestia criteria to have comparable sensitivity and NPVs to the overall study population (albeit the evaluable sample sizes of the subpopulations were limited and 95% CIs wide). Interestingly, a growing body of literature 12 –14 suggests up to 45% of patients with active cancer having PE (the latter often diagnosed incidentally during the cancer workup) can be safely treated at home or following an abbreviated hospital stay. To aid in the selection of lower risk patients with active cancer, predictive scales such as POMPE-C, 12 Registro Informatizado de la Enfermedad Tromboembolica Venosa (RIETE), 13 and the criteria by Font et al 14 have been developed. Collectively, these scales have sensitivity >87.5% and NPVs >95.6% and acceptable overall discriminative power (c-statistics = 68%-86%). Of note, the selection criteria for identifying low-risk patients studied by Font and colleagues 14 (ie, systolic BP<100 mmHg, O2 saturation <90%, active bleeding, platelet count <50 × 109/L, renal failure and medical or social [including poor medication adherence] reasons requiring hospitalization) are fairly similar to the Hestia criteria. 5 To our knowledge, no prior study has assessed the predictive accuracy of the Hestia criteria in an active cancer-specific population. In our study, the Hestia criteria classified 16.8% of the 113 patients with active cancer having PE as low risk, with predictive accuracy that rivals scales such as POMPE-C and RIETE. 12,13
Our study has limitations that require consideration. First, this validation study was performed retrospectively and therefore may be subject to biases, including bias resulting from misclassification of risk factors or from missing data. Of note, the amount of missing data in our analysis was no worse than that reported in the original Hestia derivation study. 5 Second, this was a single-center study limiting its generalizability and sample size. However, baseline characteristics and mortality rates were consistent with national estimates, 15 and our sample size of objectively confirmed patients with PE was of similar size to that of the Hestia criteria derivation study. 5 Next, although our retrospective study demonstrated the Hestia criteria can identify a cohort at low risk of early mortality and suitable for outpatient management or an abbreviated hospital stay, 88% of all patients (and 71.2% of low-risk patients) in our study remained in hospital for 3 days or more. It is possible that in-hospital management of acute PE provides therapeutic benefits that are not duplicated in the outpatient environment. If this is the case, mortality rates in our low-risk patients may not be generalizable to those treated as outpatients for following an abbreviated admission. Interestingly, a recent study by Roy et al suggested hospitalization (vs outpatient) of patients with PE may be associated with an increased risk of adverse events. 16 Finally, due to restrictions on the availability of SSDI data, we had to limit the inclusion of patients to those presenting to our emergency department prior to January 31, 2014. 17 Despite this, the sample size of patients available for final analysis was robust. Moreover, we are unaware of any programmatic changes in evaluation and treatment of patients with PE at our institution since January 2014. Consequently, the likelihood of selection bias resulting from the unavoidable exclusion of patients after this date is low.
Conclusion
The Hestia criteria demonstrated acceptable predictive accuracy for identifying patients with PE at low risk of early mortality. The sensitivity and NPV of the Hestia criteria remained high in advanced age patients and those concomitantly diagnosed with active cancer or cardiopulmonary disease. Additional prospective external validation studies of the Hestia criteria should be performed.
Footnotes
Appendix A
Authors’ Note
ERW, CGK, GJF, WFP, CC, JRS, CIC contributed to Study concept and design. ERW, CGK, CIC contributed to acquisition of data. ERW, CGK, GJF, WFP, CC, JRS, CIC contributed to analysis and interpretation of data. ERW, CGK, and CIC contributed to drafting the manuscript. ERW, CGK, GJF, WFP, CC, JRS, CIC contributed to critical revision of the manuscript for important intellectual content. ERW, CGK, CIC contributed to administrative, technical or material support. CIC contributed to study supervision. CIC had full access to all the study data and take full responsibility for the integrity of the data and the accuracy of the data analysis. All authors read and approved the final manuscript. The authors meet criteria for authorship as recommended by the International Committee of Medical Journal Editors (ICJME) and were fully responsible for all content and editorial decisions, and were involved in all stages of manuscript development.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CIC has received grant funding and consultancy fees from Janssen Scientific Affairs, LLC; Bayer Pharma AG; and Boehringer-Ingelheim Pharmaceuticals, Inc. CC, JRS are employees of Janssen Scientific Affairs LLC. GJF has received grant funding for Novartis, Cardiorentis, Cardioxyl, Cempra Pharmaceuticals, Trevena, Intersection Medical, Siemens, The Mayday Foundation, Pfizer; and is on the advisory board and speakers bureau for Janssen Scientific Affairs. FWP has received grant funding and consultancy fees from Abbott, Alere, Banyan, Cardiorentis, Janssen Pharmaceuticals, Portola, Roche, The Medicine’s Company, Prevencio and Singulex. ERW and CGK have no conflict of interest germane to this manuscript to report.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Janssen Scientific Affairs, LLC, Raritan, NJ, USA.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.