
Abstract
Appropriate timing of bivalirudin discontinuation as a bridge to warfarin is complicated, as bivalirudin may cause a falsely prolonged international normalized ratio (INR). The purpose was to evaluate patient and medication characteristics associated with differences in INR prolongation caused by bivalirudin. Adult patients receiving bivalirudin as a bridge to warfarin in 2014 were retrospectively evaluated. Patients were excluded if they had known thrombophilia or inappropriate INR monitoring after discontinuation of bivalirudin. Data recorded included indication for bivalirudin use, bivalirudin dosing, and coagulation assays. Univariate analysis was performed to determine variables associated with a larger change in INR when discontinuing bivalirudin. Variables with P < .3 were included in multivariate analysis. In total, 50 patient admissions were included in the analysis. Patients with ventricular assist devices represented the majority of the patient population (74%). The most common INR goals were 2.0 to 3.0 and 2.5 to 3.5. The mean initial weight-based bivalirudin rate was 0.076 mg/kg/h, and the mean increase in INR when starting bivalirudin was 0.6. The mean final weight-based bivalirudin rate was 0.13 mg/kg/h, and the mean change in INR after stopping bivalirudin was 0.8. On multivariate analysis, factors associated with a larger change in INR after stopping bivalirudin included higher serum creatinine (P = .033), greater change in INR after initiation of bivalirudin (P = .028), and higher final bivalirudin rate (P < .001). The change in INR when starting or stopping bivalirudin appears to be patient specific and dose related. A nomogram was developed to predict the ideal timing of bivalirudin discontinuation. Prospective evaluation of the nomogram is under way.
Keywords
Background
Bivalirudin is a direct thrombin inhibitor (DTI) that may be used as a bridge to warfarin in patients who are unable to receive unfractionated or low-molecular-weight heparin. Notable patient populations who may utilize bivalirudin include patients with heparin-induced thrombocytopenia (HIT) and patients in whom there is concern regarding the development of HIT antibodies, such as patients with ventricular assist device (VAD) thrombosis. Bivalirudin boasts several pharmacologic advantages, including a rapid onset of action, the ability to inhibit fibrin-bound thrombin, elimination primarily via proteolysis, lack of immunologic response, and a shorter half-life when compared to other parenteral anticoagulants. 1,2
While intravenous DTIs such as bivalirudin and argatroban possess these advantages over heparin, their use as a bridge to warfarin is often complicated by a false prolongation of the prothrombin time (PT) and international normalized ratio (INR). 1,3 –6 The prolongation in PT/INR is likely a result of the interaction between DTIs and the thromboplastin and tissue factor contained in the PT assay, along with the high molar concentrations of the DTIs needed to achieve their anticoagulant effect. 7 As a result, the INR while on a DTI may not represent the patient’s true degree of anticoagulation. Since argatroban has the lowest affinity for thrombin of the DTIs, it requires the highest molar concentrations to achieve therapeutic anticoagulation and thus causes a more pronounced prolongation of PT/INR. 3,6,7 Although typically less than with argatroban, an increase in PT/INR is frequently observed in patients using bivalirudin as well.
For patients utilizing DTIs as a bridge to warfarin, a number of strategies have been trialed as an attempt to correctly predict the appropriate time to discontinue the DTI and continue on warfarin monotherapy. The goal of therapy is to discontinue parenteral anticoagulation at the time the patient becomes therapeutic on warfarin. This will minimize the duration of time a patient is dual anticoagulated while avoiding early discontinuation of the DTI prior to achieving a therapeutic INR on warfarin alone. Strategies have included bridging patients until they reach an INR greater than 4.0 for argatroban 8 or 3.0 for bivalirudin, 9 use of a chromogenic factor X activity assay in addition to the PT/INR, 10 or using the patient’s initial increase in INR after initiation of the DTI to predict the change in INR when discontinuing the DTI. At Brigham and Women’s Hospital, bivalirudin is used in several high-risk patient populations, including patients with HIT and suspected or confirmed VAD thrombosis. Despite possibly having less of an effect on the INR than argatroban, significant variability in the change in INR has been observed when starting and stopping bivalirudin. Therefore, we performed a retrospective analysis to evaluate patient and medication characteristics associated with differences in the degree of PT/INR prolongation, with the goal of developing a nomogram to predict the ideal time to discontinue bivalirudin when used as a bridge to warfarin.
Patients/Methods
Study Design
Institutional IRB approval was obtained prior to the beginning of this study (IRB Protocol #2015P000808). We performed a single-center, retrospective cohort analysis of all hospitalized patients who received bivalirudin from January 2014 to December 2014. Patients were included in the analysis if they utilized bivalirudin as a bridge to warfarin. All medication usage was validated through the institution’s electronic medication administration record. The Stago Neoplastine CI Plus was the PT/INR assay utilized throughout the analysis.
Patients were excluded from the analysis if they used bivalirudin for percutaneous coronary intervention (PCI), as monotherapy for anticoagulation, or if they had a known thrombophilia. Patients were allowed to receive doses of warfarin prior to the initiation of bivalirudin. At our institution, the INR is checked at least daily for patients on warfarin. Once the INR is assumed to be therapeutic off of bivalirudin, the infusion is discontinued and the INR is rechecked to determine the patient’s INR on warfarin alone. Patients were excluded from the analysis if the INR was not checked within 2 to 6 hours after discontinuation of bivalirudin.
Outcomes
The primary outcome of the analysis was the patient’s change in INR when discontinuing bivalirudin. The change in INR was calculated by subtracting the first INR after discontinuation of bivalirudin from the final INR prior to discontinuing bivalirudin (Change in INR = INRprior to bivalirudin d/c − INRpost bivalirudin d/c). Other outcomes measured included the change in INR when initiating bivalirudin (Change in INR = INRafter bivalirudin started − INRprior to bivalirudin start), the duration of bridging from bivalirudin to warfarin, and the percentage of INRs within the patient’s therapeutic range after discontinuation of bivalirudin.
Demographic information collected for each patient included the indication for anticoagulation, the indication for utilizing bivalirudin, the goal INR range, and notable past medical history. Medication and laboratory data regarding the use of bivalirudin were also collected. Measures of renal and hepatic function were collected prior to the patient transitioning off of bivalirudin. Acute kidney injury was defined using the Acute Kidney Injury Network criteria. Creatinine clearance was calculated using the Cockroft-Gault equation. The weight-based rate (mg/kg/h) and total rate (mg/h) of bivalirudin were collected upon initiation of bivalirudin therapy and immediately prior to discontinuation. The first activated partial thromboplastin time (aPTT) and INR were collected prior to and after initiation and discontinuation of bivalirudin. The duration of therapy with bivalirudin and the duration of the bridge with bivalirudin to warfarin were recorded.
Statistical Analysis
Descriptive statistics including baseline characteristics, coagulation assays, and bivalirudin-related variables were stratified as continuous or binary. Continuous variables were presented as means with standard deviations or medians with interquartile ranges (IQRs). Binary variables were presented as numbers and proportions.
We performed a univariate analysis of all variables and patient characteristics collected in the analysis. An unpaired Student t test was used to compare the mean final change in INR when discontinuing bivalirudin between patient groups. Prior to performing the Student t test, all continuous variables were stratified so that they could be analyzed as binary variables in the univariate analysis. Assuming a β error of .80, an α error of less than .05 was considered to be statistically significant. All variables with a P value less than .3 were then included in a multivariate regression analysis.
Results
Baseline Demographics and Clinical Characteristics
In 2014, 175 patients utilized bivalirudin at the institution. Overall, 50 (28.6%) patients were included in the analysis. Reasons for exclusion were use of bivalirudin as monotherapy (100, 57.1%), INR checked at the inappropriate time after bivalirudin discontinuation (12, 6.9%), suspected or known thrombophilia (9, 5.1%), and bivalirudin use for PCI (4, 2.3%).
The mean age of the cohort was 55 years old, and the majority of patients were male (Table 1). Patients with VADs represented a high percentage of the cohort (37, 74%). Other common indications for anticoagulation included atrial fibrillation (30, 60%) and suspected or confirmed new-onset HIT (13, 26%). Bivalirudin was used most commonly for patients with a VAD implanted as a bridge to heart transplantation, where the goal was to avoid heparin exposure (20, 40%) for treatment of VAD thrombosis (13, 26%) or for confirmed new-onset HIT (10, 20%). The most frequent INR goals were 2.0 to 3.0 (29, 58%) and 2.5 to 3.5 (19, 38%).
Patient Demographics.
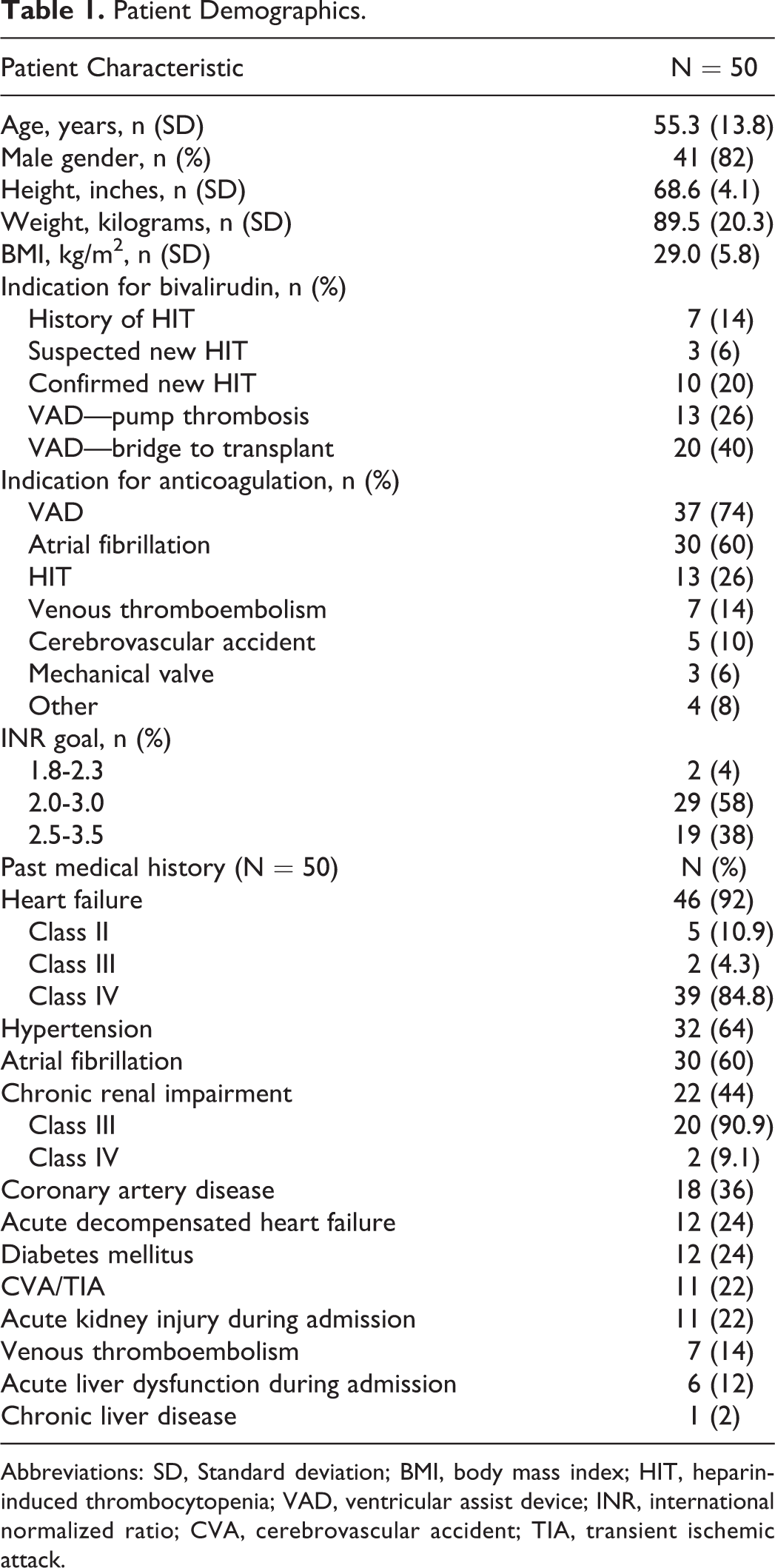
Abbreviations: SD, Standard deviation; BMI, body mass index; HIT, heparin-induced thrombocytopenia; VAD, ventricular assist device; INR, international normalized ratio; CVA, cerebrovascular accident; TIA, transient ischemic attack.
Notable past medical history in the cohort included hypertension (32, 64%), atrial fibrillation (30, 60%), coronary artery disease (18, 36%), type 2 diabetes mellitus (12, 24%), cerebral vascular accident or transient ischemic attack (11, 22%), and chronic renal impairment (22, 44%; Table 1). As a high percentage of the cohort required VAD support, heart failure was a common comorbidity (46, 92%). Thirty-nine of the 46 patients with heart failure had New York Heart Association Class IV heart failure. Acute kidney injury (11, 22%) and acute liver dysfunction (6, 12%) were relatively common within the cohort. The mean serum creatinine was 1.16 prior to transitioning off of bivalirudin. The mean creatinine clearance prior to discontinuation of bivalirudin was 70 mL/min.
Anticoagulation Characteristics
The mean initial weight-based rate of bivalirudin was 0.076 mg/kg/h (Table 2). The average initial total rate of bivalirudin was 6.81 mg/h. The mean initial INR prior to initiating bivalirudin was 1.6. The mean initial INR after starting bivalirudin was 2.2, representing an average change in INR of 0.6 after starting bivalirudin. The mean weight-based rate and total rate of bivalirudin prior to discontinuation were 0.13 mg/kg/h and 11.31 mg/h, respectively. The mean final INR prior to discontinuation of bivalirudin was 3.2, and the mean INR after stopping bivalirudin was 2.4. The average change in INR after stopping bivalirudin was 0.8. The median duration of therapy with bivalirudin was 7 days, and the median duration of bridge therapy with warfarin was 5.5 days. The mean aPTT prior to transitioning off bivalirudin was 83.6 seconds. The mean aPTT after transitioning off of bivalirudin was 55.4 seconds. The mean time between discontinuation of bivalirudin and rechecking the INR was 4.1 hours. Patients were within their therapeutic INR range in 30 (60%) of the cases. Most patients who were not within their therapeutic INR range were subtherapeutic (18, 90%).
Bivalirudin and Laboratory Results.
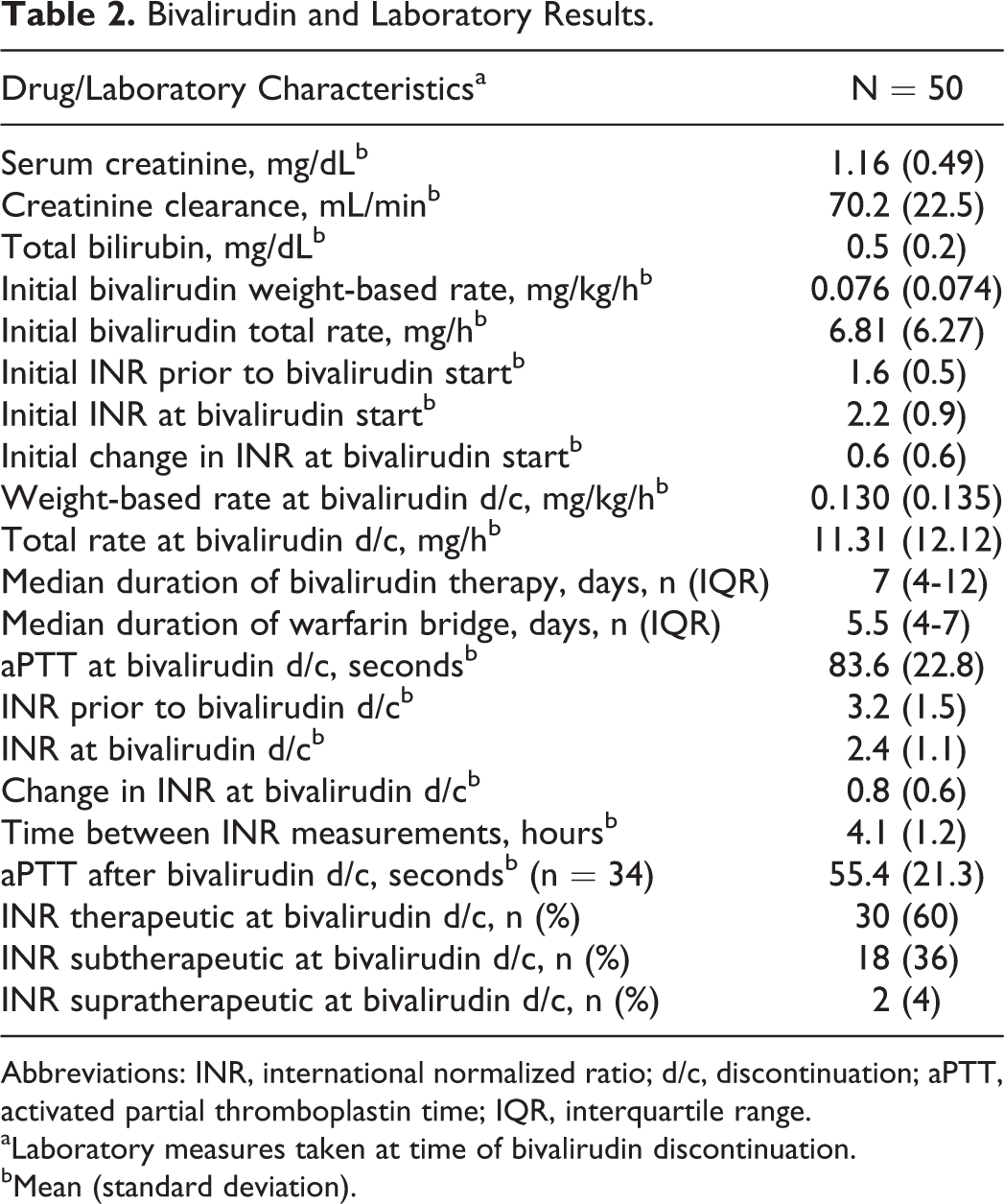
Abbreviations: INR, international normalized ratio; d/c, discontinuation; aPTT, activated partial thromboplastin time; IQR, interquartile range.
aLaboratory measures taken at time of bivalirudin discontinuation.
bMean (standard deviation).
Univariate and Multivariate Analyses
On univariate analysis, several variables were associated with a significantly larger decrease in INR upon discontinuation of bivalirudin (Table 3). Patients with a body mass index (BMI) less than 30 had a greater change in INR than those with BMI more than 30 (0.92 vs 0.50, P = .011). Patients with a diagnosis of heart failure had a significantly larger decrease in INR than those without (0.78 vs 0.30, P = .015). The change in INR after discontinuing bivalirudin was also greater in patients with an initial INR less than 1.6 (0.94 vs 0.55, P = .033).
Univariate Analysis of the Change in INR Upon Bivalirudin Discontinuation.
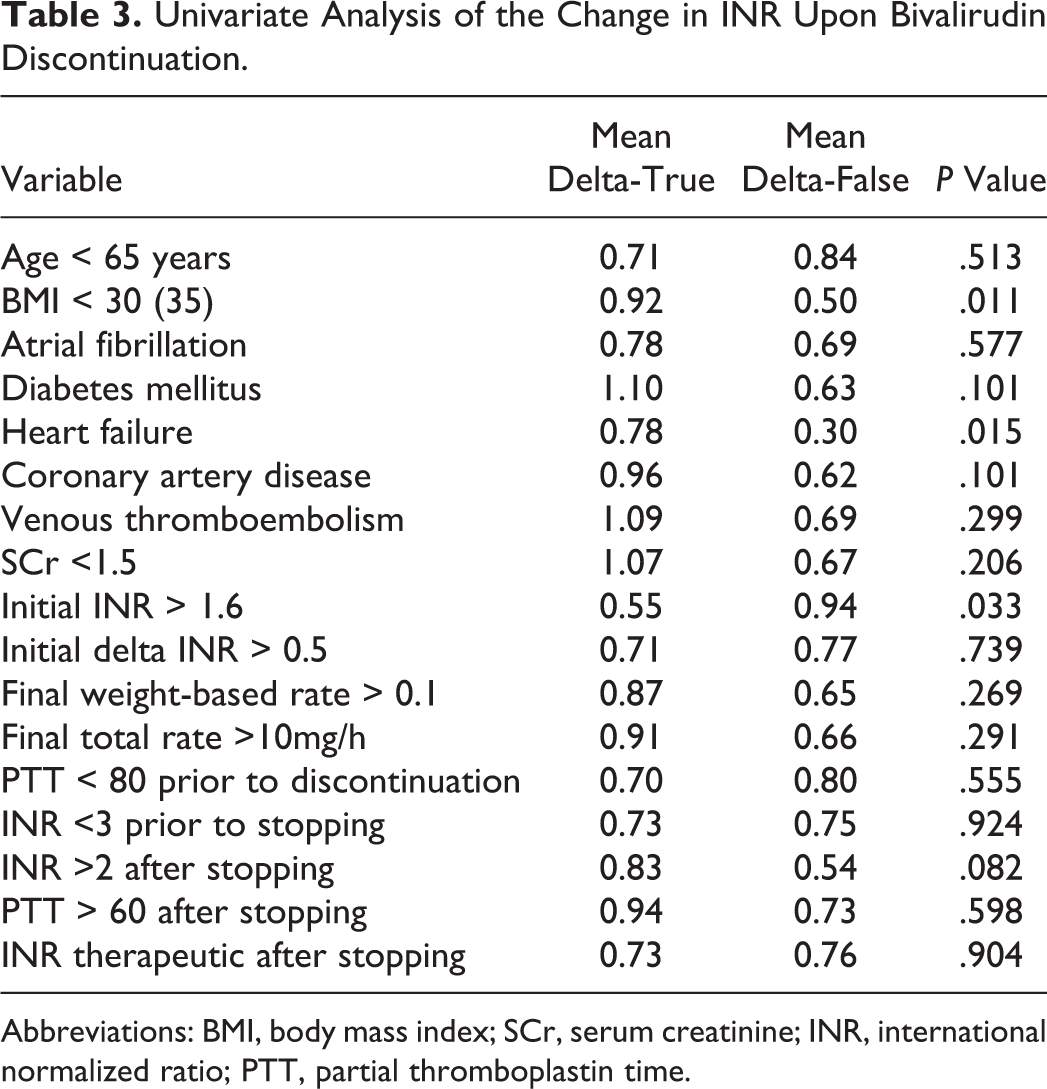
Abbreviations: BMI, body mass index; SCr, serum creatinine; INR, international normalized ratio; PTT, partial thromboplastin time.
Eleven variables had a P value less than .3 on univariate analysis and were included in the multivariate regression analysis (Table 4). On multivariate analysis, 4 variables were significantly associated with a higher change in INR when stopping bivalirudin. Patients with a higher serum creatinine had a greater change in INR when discontinuing bivalirudin (P = .033). Patients with a greater initial change in INR when starting bivalirudin (P = .028) and patients with a higher INR prior to discontinuing bivalirudin (P < .001) had a greater change in INR upon discontinuation. Finally, patients who were on a higher weight-based rate of bivalirudin (mg/kg/h) had a greater change in INR when stopping bivalirudin (P < .001).
Multivariate Analysis of the Change in INR Upon Bivalirudin Discontinuation.
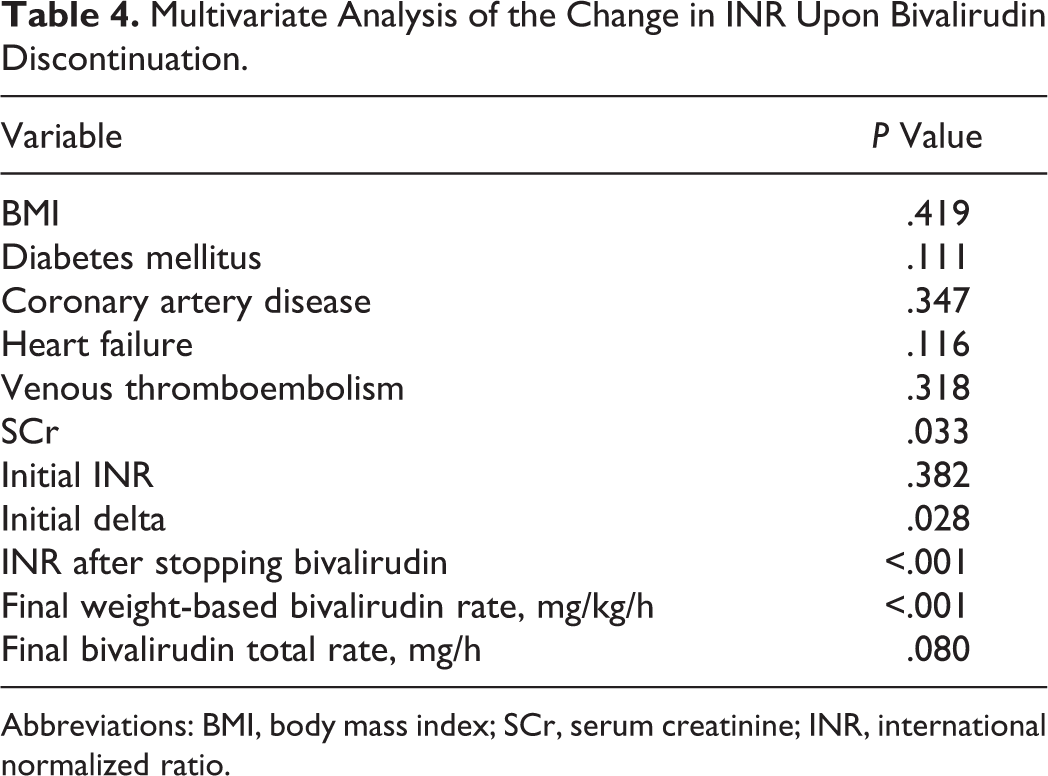
Abbreviations: BMI, body mass index; SCr, serum creatinine; INR, international normalized ratio.
Development of a Predictive Model
During data analysis, we identified and investigated a trend. The change in INR when discontinuing bivalirudin was directly proportional to the patient’s initial change in INR when starting bivalirudin and the change in weight-based bivalirudin rate from when the patient started on bivalirudin and discontinued. These observations were further corroborated by the findings of the multivariate analysis, which demonstrated that the initial change in INR when starting bivalirudin and the final rate of bivalirudin prior to discontinuation significantly affected the change in INR when discontinuing bivalirudin.
To test this theory, the ratio of final bivalirudin weight-based rate prior to discontinuation to initial bivalirudin weight-based rate was calculated for each patient (weight-based rate bivalirudin d/c /weight-based rate bivalirudin start). The ratio of final change in INR when stopping bivalirudin to initial change in INR when starting bivalirudin was also calculated (change in INRbivalirudin d/c /change in INRbivalirudin start). These 2 ratios were compared and were found to have a linear relationship in nearly a 1:1 ratio (Figure 1). The correlation between these variables was strong with an R 2 value of .8723. One data point had a significantly higher bivalirudin rate ratio than all of the other data points. When this data point was removed, the correlation between these 2 variables remained strong (R 2 = .6421, Figure 2).
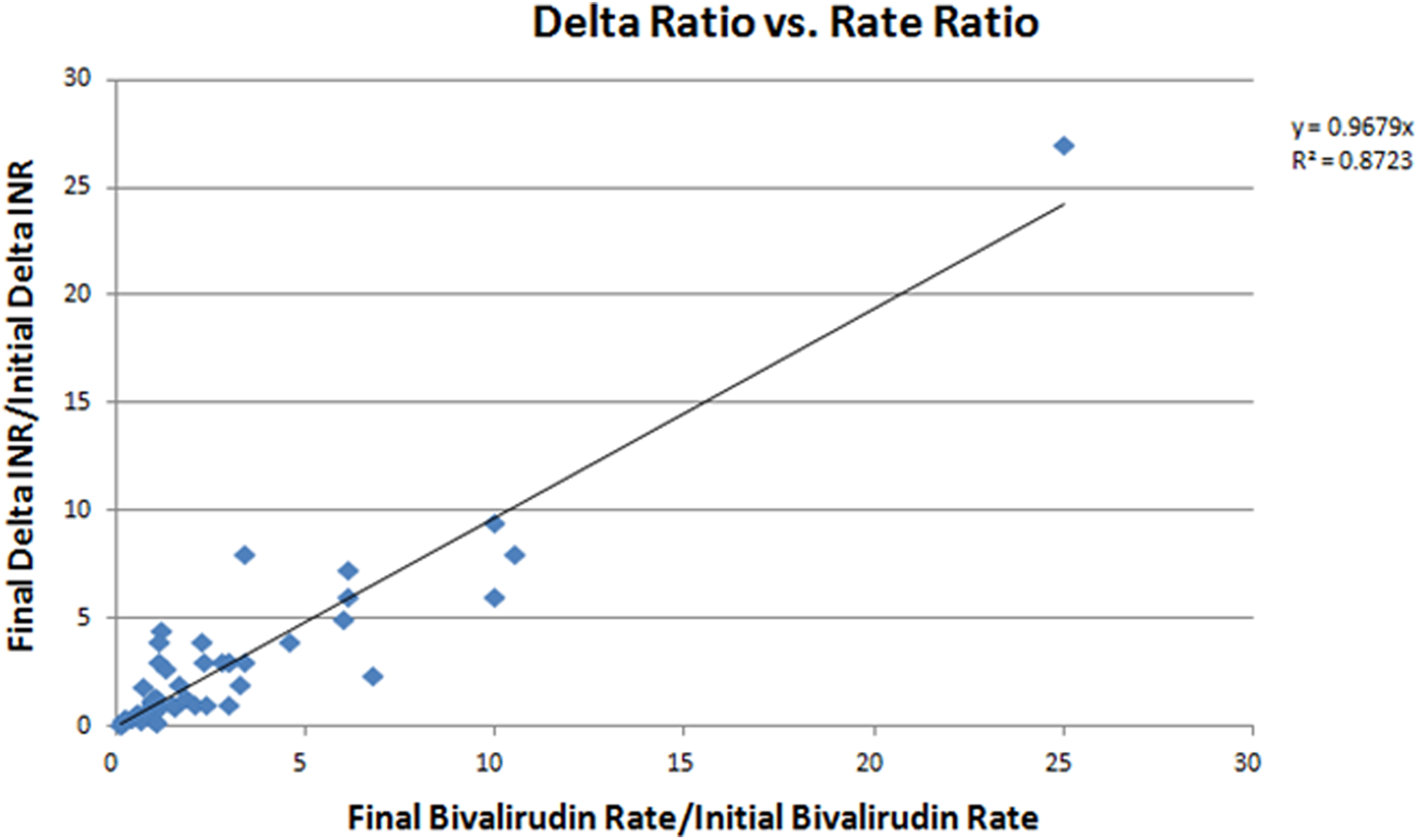
The linear correlation between the initial and final weight-based rates of bivalirudin and the change in INR when starting and stopping bivalirudin.
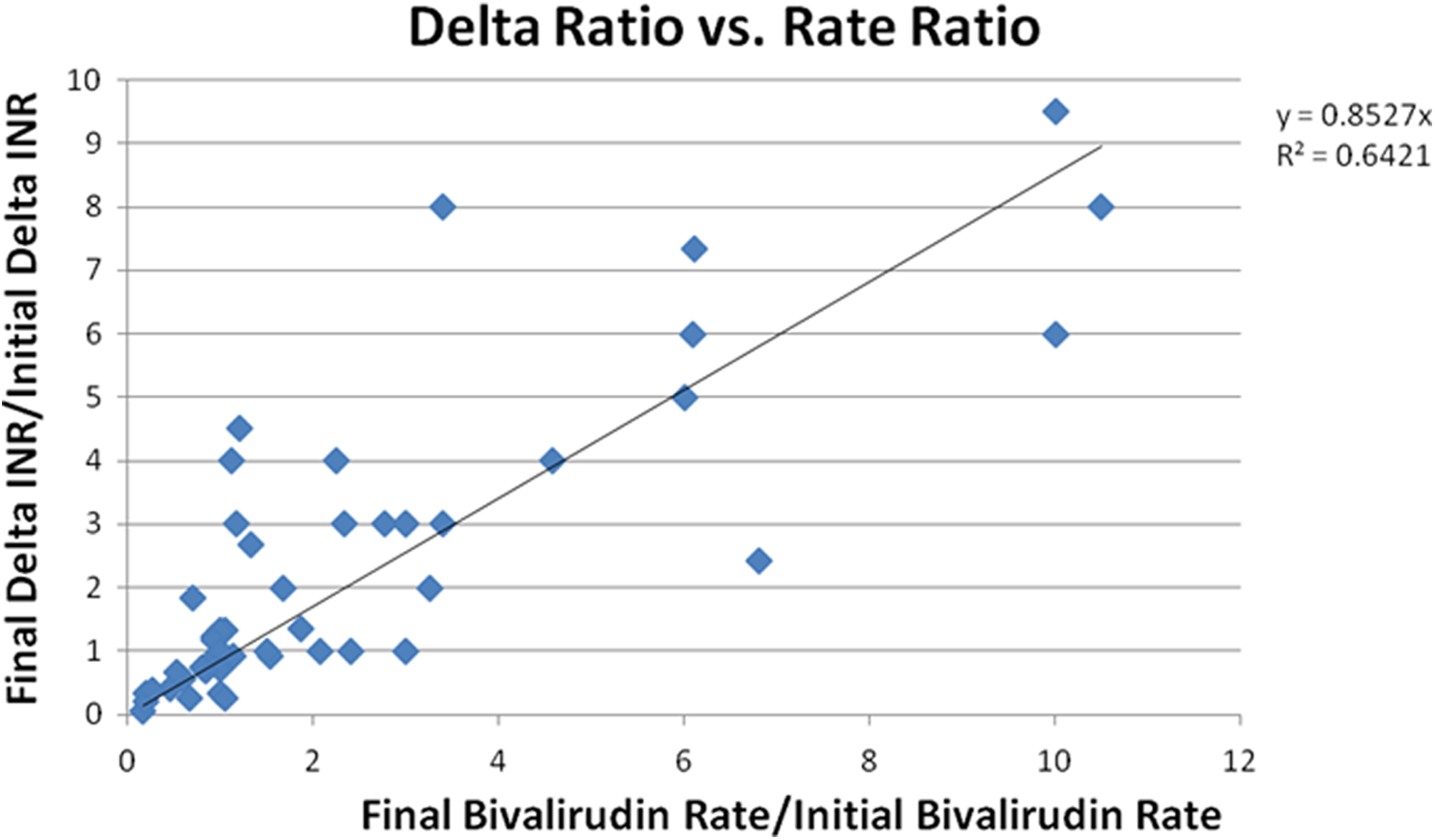
The linear correlation between the initial and the final weight-based rates of bivalirudin and the change in INR when starting and stopping bivalirudin, with 1 data point removed.
Based on this 1:1 linear correlation, a predictive equation for the final change in INR when discontinuing bivalirudin was developed. The final change in INR when discontinuing bivalirudin was equal to the initial change in INR when starting bivalirudin multiplied by the proportion of the final and initial weight-based bivalirudin rates (Change in INRbivalirudin d/c = Change in INRbivalirudin start × [weight-based ratebivalirudin d/c/weight-based ratebivalirudin start]). This model was applied to each patient in the cohort to predict the final change in INR when discontinuing bivalirudin (Table 5). The median difference between the predicted change in INR and the actual change in INR was 0.14 (IQR: 0.06-0.34). The predicted change in INR was within 0.2 of the actual change in INR in 32 (64%) of the patients. The predicted change in INR was within 0.4 of the actual change in INR in 42 (84%) of the patients.
Retrospective Application of the INR Prediction Equation.
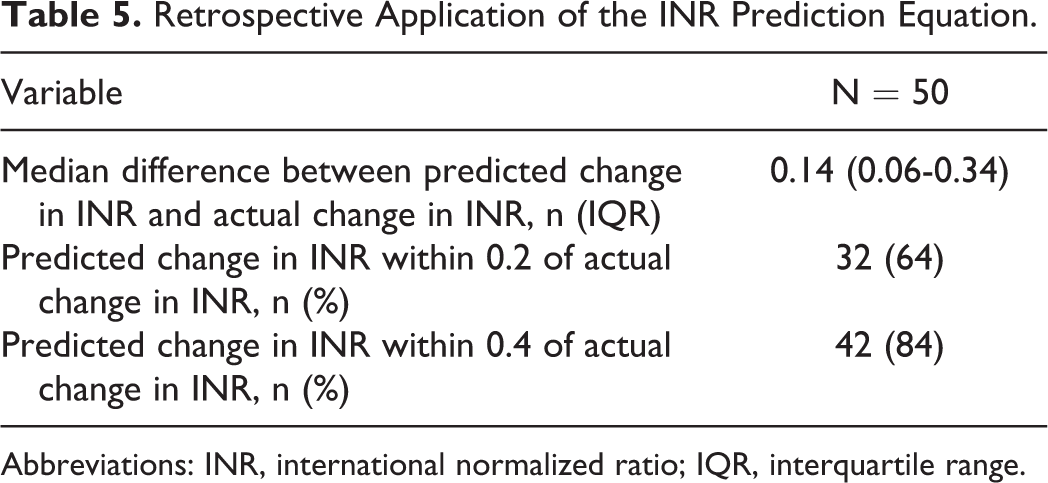
Abbreviations: INR, international normalized ratio; IQR, interquartile range.
Discussion
The impact of bivalirudin on the INR for most patients appears to be a dose-related effect. Variables associated with an increased change in INR when discontinuing bivalirudin included the initial change in INR, the serum creatinine, and the rate of bivalirudin prior to discontinuation. Because of the difficulties in predicting the warfarin-associated INR while a patient is on bivalirudin, a large percentage of patients were not within their INR target range upon stopping bivalirudin. We present evidence of a novel strategy that may improve the ability to predict a patient’s warfarin-associated INR before discontinuing bivalirudin.
The suspected mechanism for prolongation of the PT and increased INR is due to the effect of bivalirudin on the assay reagent. Inhibition of thromboplastin and tissue factor in the reagent by bivalirudin prevents activation of the PT assay. 2,7 The findings of our analysis support this mechanism, as changes in INR when starting or stopping bivalirudin were highly correlated with the weight-based rate of bivalirudin. Patients who required higher weight-based rates of bivalirudin had a larger change in INR. Patients who had a higher INR prior to discontinuation of bivalirudin likely had a greater change in INR when initiating bivalirudin and were thus bridged to a higher INR before stopping the medication. While patients with higher serum creatinine typically require lower rates of bivalirudin, given the medication’s partial renal clearance, 11,12 our cohort included a number of frail patients with low serum creatinines who required lower weight-based rates of the medication. As such, it is possible that this contributed to the association between higher serum creatinine and an increased change in INR.
An important factor that should not be overlooked is the aPTT upon discontinuation of bivalirudin. While the aPTT was not checked after discontinuation of bivalirudin in the entire cohort (n = 34), the mean aPTT was above the upper limit of normal. This suggests that there may have still been some bivalirudin in the patient’s system upon measurement of the INR. Because the bivalirudin may not have been completely eliminated, it is possible that the change in INR upon bivalirudin discontinuation was underestimated.
Clinically, the ability to predict when the INR is therapeutic on warfarin while a patient is on concomitant bivalirudin is challenging. Several strategies have been previously utilized, each with their limitations. Bridging patients to a predefined goal INR may lead to discontinuation of bivalirudin too early in some patients and overanticoagulation in others. 8 Use of a chromogenic factor X activity assay may not be readily available at all institutions and incurs an additional cost. Reliance on the change in INR when starting bivalirudin does not consistently predict the change in INR upon discontinuation. In our cohort, only 60% of patients had a therapeutic INR upon discontinuation of bivalirudin, with the majority of out-of-range patients having a subtherapeutic INR.
Development of a predictive model for appropriate timing of discontinuation of bivalirudin as a bridge to warfarin would be valuable, both clinically and economically. Increasing the proportion of patients who are within therapeutic range when stopping bivalirudin may improve clinical outcomes such as hemorrhage or thrombosis. Additionally, predictive modeling could prevent the need for expensive laboratory testing and could possibly decrease drug costs associated with extended bivalirudin use. Prospective validation of our predictive model is currently under way with objectives to accurately predict a patient’s INR after stopping bivalirudin and to increase the percentage of patients with a therapeutic INR upon bivalirudin discontinuation.
The results of this analysis must be taken in context with our study design. Because of a limited sample size, there may be additional factors associated with an increased change in INR that were not captured. Patient and medication characteristics that may have contributed to the correlation in this analysis may not be observed in a prospective cohort of patients. Prospective evaluation of the predictive model hypothesized by the results of this cohort is under way. Differences in PT/INR assays may impact this model. 3 It is also unclear whether the same principles can be applied to changes in INR cause by other DTIs, such as argatroban.
Conclusion
The change in INR when starting and stopping bivalirudin appears to be most closely related to the weight-based rate of bivalirudin being utilized. Historically, determination of the appropriate time to discontinue bivalirudin has been difficult. Prediction of the INR when discontinuing bivalirudin may be achieved using the change in INR when initiating bivalirudin and the weight-based rates of bivalirudin when starting and stopping the medication. Future research efforts will be centered on validation of a prospective predictive model for appropriate timing of bivalirudin discontinuation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JMC reports personal fees from Boehringer Ingleheim, personal fees from Bristol Meyer Squibb, and personal fees from Thoratec, all of which are outside the submitted work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.