
Abstract
Background:
Intravenous fluids with synthetic colloids such as hydroxyethyl starch (HES) are known to interfere with plasma fibrinogen concentration measurements. The aim of this study was to evaluate the effects of an HES solution on fibrinogen measurements in a clinical setting.
Methods:
The study was performed in patients who received at least 1 L of HES during intracranial tumor resection surgery. Blood samples were drawn before the start of surgery (baseline), after infusion of 1 L of HES, and at later time points. The fibrinogen concentration was measured using 3 different methods: (a) enzyme-linked immunosorbent assay (ELISA), (b) Clauss method with a photometric readout, and (c) Clauss method with an electromechanical readout. In addition, the fibrin-based clot quality was evaluated with the thromboelastometric FIBTEM test.
Results:
Forty patients were enrolled, and 25 patients were included in the analysis. The fibrinogen concentrations at baseline were 2.2, 2.3, and 2.6 g/L and after 1 L of HES 1.6, 1.7, and 1.9 g/L as measured by ELISA, the photometric test, and the electromechanical test, respectively. The electromechanical Clauss test measured significantly higher concentrations at these time points. The relative decrease, however, was comparable between methods (31%, 29%, and 25%, respectively) but significantly lower than the 44% relative decrease with FIBTEM maximum clot firmness.
Conclusion:
Despite providing different fibrinogen concentration values at baseline, the relative decrease in fibrinogen concentration after HES infusion was comparable among the 3 tests. In contrast, fibrin-based clot quality was more affected than fibrinogen concentration tests by HES infusion.
Introduction
The importance of maintaining adequate plasma fibrinogen concentration in major bleeding, both traumatic and surgical, is increasingly being recognized. The recent European guidelines on the management of severe perioperative bleeding recommend fibrinogen substitution if significant bleeding is accompanied by thromboelastometric signs of a functional fibrinogen deficit or a plasma fibrinogen level less than 1.5 to 2.0 g/L. 1 Fibrinogen concentrate has been included in algorithms for bleeding management in trauma, 2 and perioperative administration of fibrinogen concentrate has been shown to decrease bleeding in elective aortic surgery 3 and prostatectomy. 4 Thus, fast and reliable analyses of fibrinogen concentrations are important. However, widely used intravenous fluids with synthetic colloids such as hydroxyethyl starch (HES) are known to interfere with different plasma analyses of fibrinogen. The often-used measurements based on the Clauss method with a photometric readout give falsely high results in the presence of HES, but this phenomenon has only been demonstrated in in vitro studies. 5 –8 Therefore, the main objective of this study was to compare, in an in vivo clinical setting, the effects of an HES solution on fibrinogen concentration tests: the Clauss method with photometric readout, the Clauss method with electromechanical readout, and enzyme-linked immunosorbent assay (ELISA). In addition, we also studied the effect of HES in vivo on a thromboelastometric whole-blood, fibrin-based test, FIBTEM. Our hypothesis was that fibrinogen concentration tests would yield different results after the patients had received HES.
Materials and Methods
Patients
This single-center, clinical, cross-sectional study was approved by the Regional Ethical Review Board of Lund, Sweden (Protocol DNR 2012/43). Patients aged 18 years or older who were admitted for craniotomy and intracranial tumor resection at the Department of Neurosurgery (SUS Lund, Sweden) were considered candidates for inclusion in the study. Informed and signed consent was received from 40 patients from February 2012 to May 2012 (Figure 1). No patient withdrew from the study. Exclusion criteria were as follows (1) abnormal activated partial thromboplastin time, prothrombin time, or platelet count; (2) known congenital or acquired coagulation disorder; (3) known hypersensitivity to HES or creatinine levels above normal range; (4) treatment with coagulation and/or platelet inhibitors within 5 days prior to surgery.
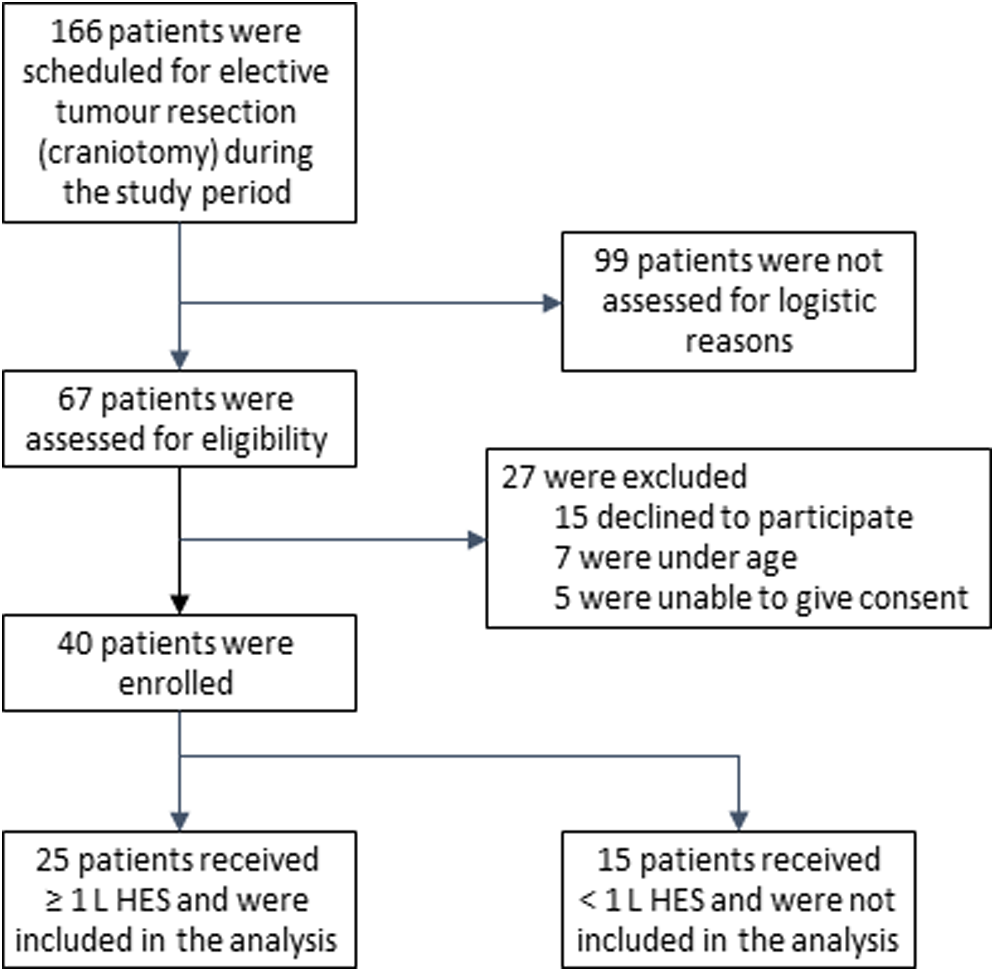
Assessment, enrolment, and analysis of study patients.
Blood Samples
Blood samples for fibrinogen analysis were obtained before the onset of surgery (baseline); after administration of 1 L of HES; at the end of surgery; and also at 3, 6, and 12 hours after the end of surgery. Arterial blood samples were drawn from the radial arterial catheters into citrated glass tubes at a volume ratio of 1:10 (BD Vacutainer Citrate Tube; glass; 0.109 mol/L citrate). At each time point, two 4.5-mL glass tubes were collected, and a portion of the blood (0.4 mL) was pipetted into a polystyrene tube (Staedler) for later thromboelastometry (see subsequently). After centrifugation (3000 rpm for 20 minutes) of the glass tubes, the supernatant was collected, aliquoted into Eppendorf tubes, and stored at −85°C until later fibrinogen concentration analyses.
Anesthetic Protocol
The patients did not receive premedication. Standard monitors, including electrocardiography, noninvasive arterial pressure, pulse oximetry, carbon dioxide, and gas analyzer, were applied during induction and maintenance of anesthesia. Anesthesia was induced with propofol (1.5-3.0 mg/kg) and fentanyl (1.5-3 µg/kg). Intubation was facilitated with rocuronium (0.5-0.8 mg/kg). Anesthesia was maintained with inhalation gas (isoflurane; MAC 1.1-1.4), with positive pressure ventilation in a circle system. Minute ventilation was adjusted to maintain normocapnia (PaCO2 of 4.5-5.5 kPa), and hypothermia was prevented with a forced air warming blanket. After induction, a radial arterial catheter was inserted for continuous measurement of blood pressure and collection of blood samples. Arterial blood gas, hemoglobin, electrolyte, and blood glucose levels were analyzed before the beginning of surgery and during surgery every 1 to 2 hours (Radiometer ABL800 FLEX; Radiometer, Copenhagen, Denmark).
Fluid regime
The fluid regime was based on a standard protocol from the anesthesia department. This was occasionally modified at the discretion of the anesthesiologist in charge, independent of the research team. At the induction of anesthesia, a basal infusion of 1.5 to 2.0 mL/kg/h of saline (NaCl 0.9%; B. Braun Medical AB) was started. Initial bleeding up to 200 to 300 mL was substituted with saline (2-3 mL per ml of bleeding) and then with HES (1-2 mL per mL of bleeding; HES; Venofundin 60 mg/mL HES; MW 130 kDa; substitution 0.42; B.Braun Medical AB). The HES was also used to compensate for the hemodynamic effects of anesthesia. Packed red blood cells (PRBCs) were administered when the concentration of hemoglobin reached below 95 to 100 mg/mL. Blood loss of more than 30% of the calculated blood volume was substituted with PRBCs, fresh frozen plasma, and platelet concentrates. A maximum volume of 2 L of saline was administered per 4 hours of surgery together with a maximum volume of 2 L of HES.
Thromboelastometry
Thromboelastometry (ROTEM; TEM International, Munich, Germany) was used for viscoelastic coagulation analysis according to the manufacturer’s instructions. To ensure sample temperature, the blood used for the thromboelastometric analysis was kept for 30 minutes in a heating block at 37°C. A FIBTEM test was run—that is, the extrinsic pathway of coagulation was activated with tissue factor and phospholipids in combination with CaCl2 and cytochalasin D. The tests were run for 60 minutes, and the maximum clot formation (MCF) was measured. Cytochalasin D inhibits the platelets’ contribution to the clot; therefore, FIBTEM-MCF represents the clot strength of the fibrin-based clot, broadly dependent on fibrin formation and polymerization alone. 9
Immunoassay of Total Fibrinogen
Enzyme-linked immunosorbent assay was used to measure the total concentration of fibrinogen in plasma. The assay contained rabbit polyclonal antibody specific for human fibrinogen and was performed according to the manufacturer’s instructions (Zymutest Fibrinogen; Hyphen BioMed, France). A calibration curve was obtained from the analysis of standard solutions of human fibrinogen provided by the manufacturer. The standard solutions were calibrated using a highly purified human fibrinogen with >99% clotting ability and which concentration was exactly determined with a protein assay.
Clotting Rate Tests According to the Clauss Method
Thrombin was added in excess to the plasma sample, ensuring the clotting time was independent of access to thrombin. The clotting time is inversely proportional to the concentration of clottable (“functional”) fibrinogen.
10
The 2 variants of the Clauss method used were as follows: Clauss method with photometric clotting time test (“Photometric test”): The clotting time was recorded using an automated coagulometer measuring turbidity (Sysmex CA 7000; Siemens AG, Erlangen, Germany). Bovine thrombin solution was added (Dade Thrombin Reagent 100 U/mL; Siemens AG, Erlangen, Germany) to the plasma samples diluted 1:10 with Dade Owren Veronal buffer (Siemens). Calibration was obtained from the clotting times of serial dilutions of standard human plasma (Siemens) with known clottable fibrinogen concentration that is traceable to the 2nd International Standard for fibrinogen in plasma. Clauss method with electromechanical clotting time test (“Electromechanical test”): The clotting time was recorded using an automated coagulometer measuring the viscosity of the sample with an electromagnetic system (STA-R-Evolution; Stago, Asnières sur Seine, France). The oscillation of a steel ball within the cuvette was measured, and an algorithm used the variations in oscillation amplitude to determine the clotting time. The reagent, STA-Fibrinogen 5 (Stago), based on human thrombin, was added to plasma samples diluted 1:20 with STA Owren-Koller buffer (Stago). The assay is precalibrated for each lot that has been determined with a secondary standard that is traceable to the 2nd International Standard for fibrinogen in plasma.
Statistical Methods
Friedman nonparametric 1-way analysis of variance was used to calculate statistical significances of intragroup variances, with Dunn multiple comparisons test to control for the family-wise error rate. The statistical significance of intergroup variances was calculated using the Wilcoxon matched-pair, signed-rank test with Bonferroni correction to control for the family-wise error rate. Power analysis was based on the first 6 patients included for analysis. We determined that the analysis of 20 patients would provide a power of 80% to show a significant difference between the fibrinogen measurement methods (main hypothesis) at a 2-sided αlevel of .05 corrected for family-wise error rate and assuming a difference of 0.2 g/L to be of clinical interest. Statistics were calculated with GraphPad Prism 6 and power analysis with G*Power 3.
Results
Of the 40 patients included in the study, 25 received an intraoperative dose of at least 1 L and a maximum of 2 L of HES (Figure 1). The preoperative characteristics of these 25 patients are presented in Table 1. Their estimated perioperative bleeding was 700 mL (70-2500 mL; median and range). The average hemodilution after infusion of 1 L of HES (calculated from the difference in the hemoglobin concentration between before surgery and after 1 L of HES) was 16.3%. Three of the 25 patients received a total of 6 units of PRBCs when the infusion of 1 L of HES was completed. Excluding these 3 patients from the hemodilution calculation yielded a hemodilution of 15.6%.
Characteristics of the 25 Patients Included in the Analysis (Means ± Standard Deviation).
Abbreviation: Hb, hemoglobin.
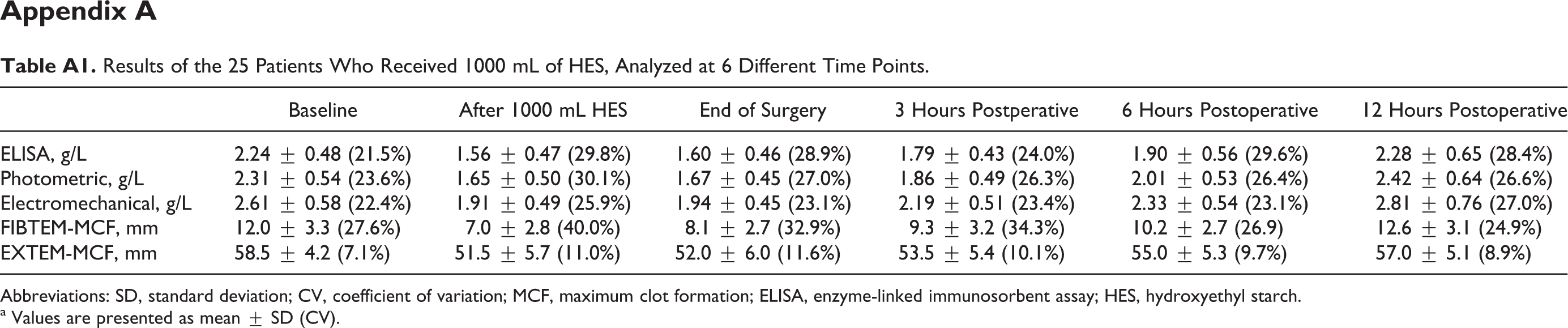
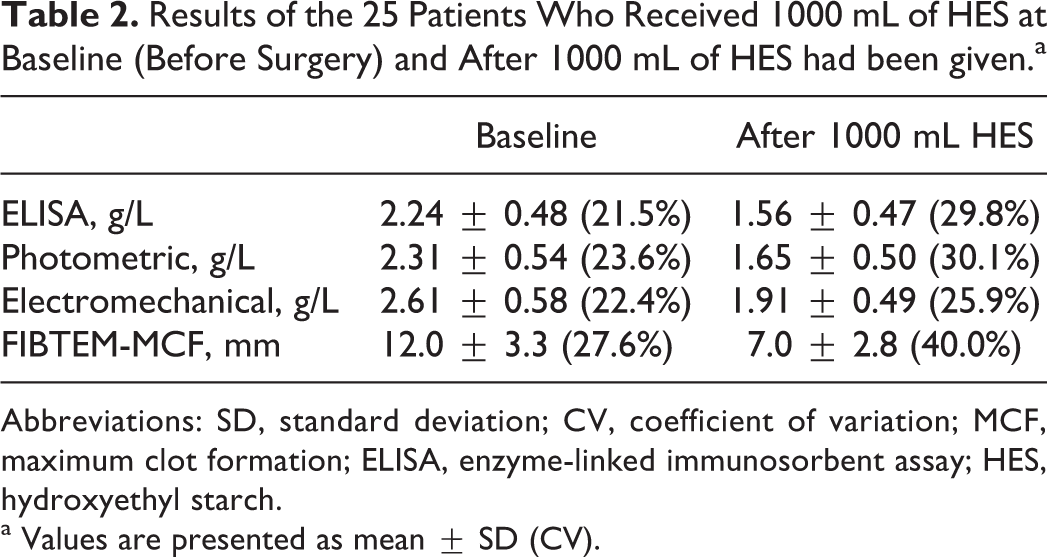
The results from the 25 patients included in the analyses are presented in Table 2, with baseline values and the results after administration of 1 L of HES. (Table A1 in appendix presents all the results from baseline until 12 hours postoperatively.) The mean preoperative values (baseline) of the plasma fibrinogen concentration in the 25 patients were 2.2, 2.3, and 2.6 g/L using the ELISA, photometric, and electromechanical tests, respectively. After administration of 1 L of HES and an average hemorrhage of 890 mL, the plasma fibrinogen concentration decreased to 1.6, 1.7, and 1.9 g/L, respectively (P < .001 for all methods; Figure 2). At these 2 time points, the electromechanical test measured significantly higher values than both the ELISA and the photometric tests (P < .001), whereas the ELISA and photometric Clauss method did not differ significantly from one another. However, the decrease in the 3 fibrinogen concentration tests did not significantly differ from one another, and the decreases ranged from 0.65 to 0.70 g/L. To compare FIBTEM-MCF with the plasma fibrinogen concentration, we calculated the changes in relation to the baseline values. After infusion of 1 L of HES, FIBTEM-MCF had decreased by 44%, which was significantly more (P < .001) than the relative decrease in plasma fibrinogen as measured using any of the fibrinogen concentration tests, that is, the ELISA, the photometric Clauss test, and the electromechanical Clauss test, which decreased by 31%, 29%, and 27%, respectively (Figure 3).
Results of the 25 Patients Who Received 1000 mL of HES at Baseline (Before Surgery) and After 1000 mL of HES had been given.a

Abbreviations: SD, standard deviation; CV, coefficient of variation; MCF, maximum clot formation; ELISA, enzyme-linked immunosorbent assay; HES, hydroxyethyl starch.
a Values are presented as mean ± SD (CV).
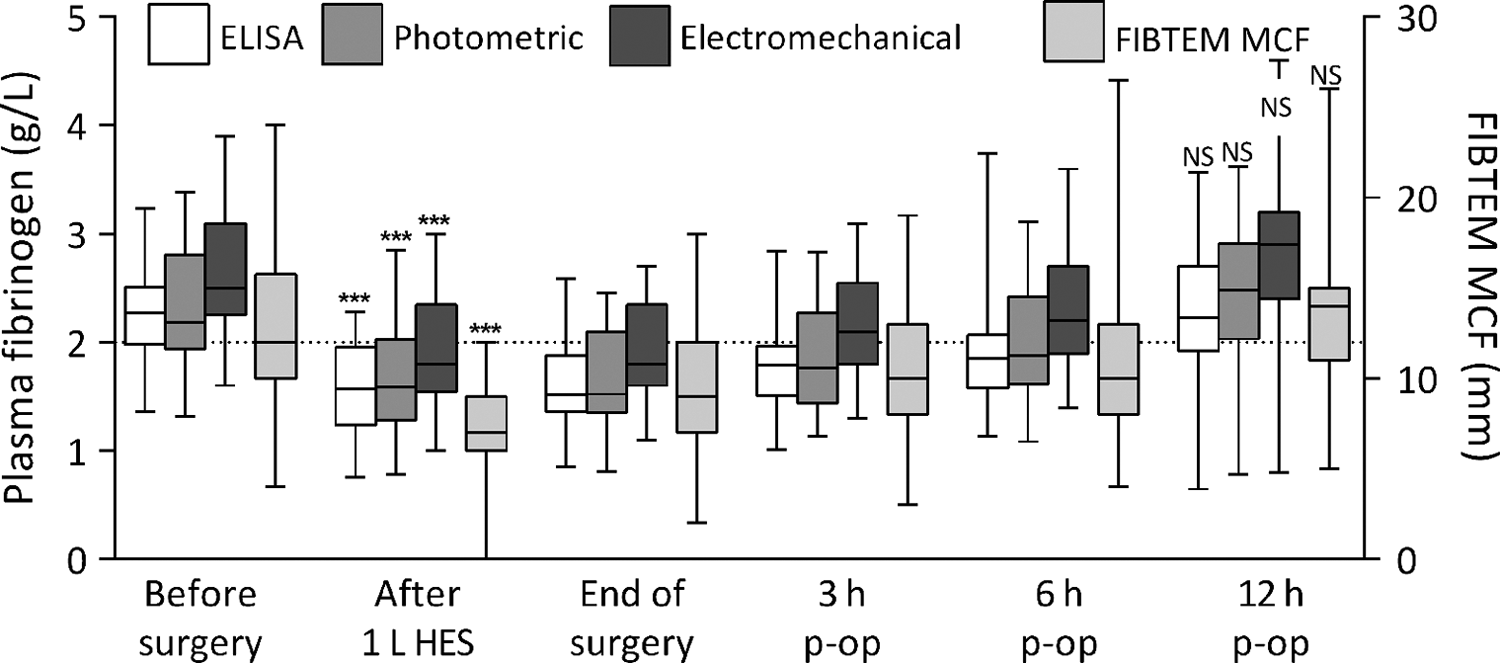
Concentration of fibrinogen in plasma (P-fibrinogen) at different times as measured using 3 different methods: ELISA, the photometric Clauss test, and the electromechanical Clauss test (left axis). The value of FIBTEM-MCF is also shown (right axis and rightmost boxplots). Comparisons of each method with baseline values (before surgery). After infusion of 1 L of HES, the plasma fibrinogen concentration obtained by each method was significantly lower than at baseline as was FIBTEM MCF, but all had returned to baseline 12 hours postoperatively (p-op). Boxes represent medians surrounded by the first and third quartiles with whiskers from the minimum to maximum values. ***P < .001 and NS is “not statistically significant” as compared with baseline values. N = 25. MCF indicates maximum clot formation; ELISA, enzyme-linked immunosorbent assay; HES, hydroxyethyl starch.
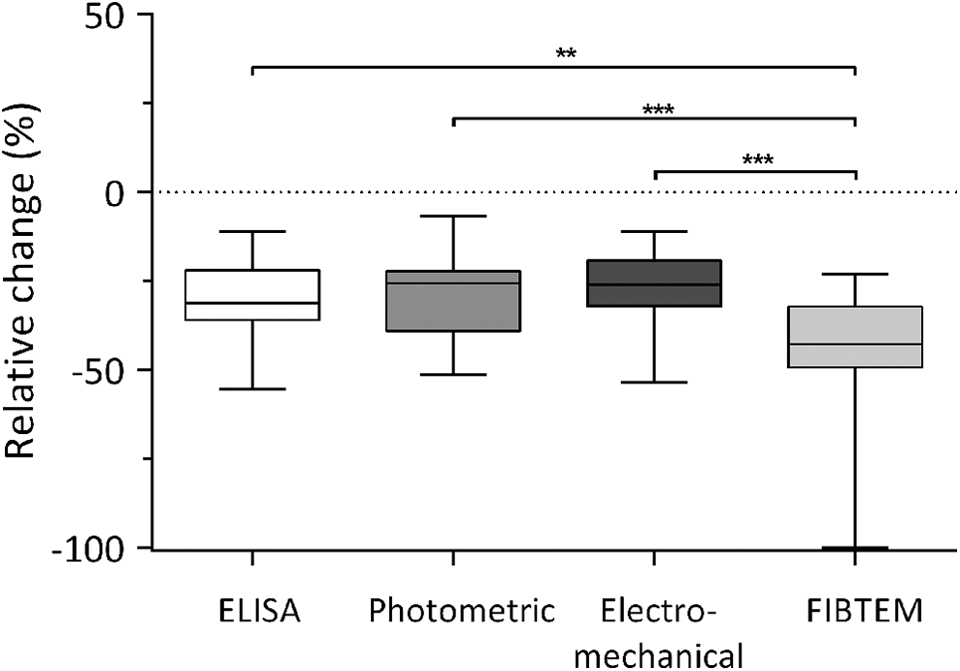
The relative change (%) in plasma fibrinogen concentrations from baseline (preoperative) until after 1 L HES, measured with 3 different tests: ELISA, the photometric Clauss test, and the electromechanical Clauss test (the 3 boxes to the left) and the relative change (%) of FIBTEM MCF (right-most box) are given. Boxes represent medians surrounded by the first and third quartiles with whiskers from the minimum to maximum values. **P < .01 and ***P < .001. N = 25. MCF indicates maximum clot formation; ELISA, enzyme-linked immunosorbent assay; HES, hydroxyethyl starch.
After the surgery, plasma fibrinogen concentrations rapidly increased and reached slightly above the baseline values on the morning after surgery, approximately 12 hours after the end of surgery. The FIBTEM-MCF followed the same pattern and was also restored to baseline values on the morning after surgery.
To evaluate the ability of the measured variables to predict surgical bleeding, the results of all 40 patients enrolled were stratified into 2 groups: one group of patients with bleeding 0 to 500 mL and one group with patients bleeding >500 mL (see appendix, Table A3). The differences in fibrinogen concentrations between the 2 groups were minimal (0.05 g/L with the photometric method and 0.03 g/L with the other 2). The difference in measured FIBTEM-MCF was also small and not significant: 13.2 ± 4.6 mm with patients bleeding 0 to 500 mL and 11.7 ± 3.9 mm with patients bleeding >500 mL.
Discussion
Our study showed that the 3 tests used to measure fibrinogen concentration—that is, the ELISA test, photometric Clauss test and electromechanical Clauss test—were equally affected by in vivo hemodilution with HES in patients undergoing intracranial tumor resection surgery. By contrast, the relative decrease in the clot strength of the fibrin-based clot was significantly greater than with any of the tests used to determine the plasma fibrinogen concentration.
In our study, plasma fibrinogen concentration after hemodilution with HES decreased by 27% to 31%, which was more than anticipated from the hemodilution calculated to 16%. This discrepancy is probably caused by in vivo consumption of fibrinogen during surgery. There were no significant differences between the 2 Clauss-based tests, which actually is in concordance with 2 studies by Adam et al 5 and Fenger-Eriksen et al, 7 respectively. Both these studies found that the validity of an immunologic method was unaffected by 30% hemodilution and that a mechanical test was more reliable than a photometric test. However, photometric readout with certain thrombin reagents, especially Multifibren U, overestimated fibrinogen concentrations at 30% hemodilution with HES, 5,7 and this overestimation was more pronounced at 50% hemodilution. 7 The combination of photometric readout and Dade Thrombin Reagent was shown to accurately measure fibrinogen concentrations and to be comparable with a mechanical readout with either the same reagent or another thrombin reagent (Multifibren U). 5 In summary, these previous studies have shown that an electromechanical readout with any thrombin reagent or a photometric readout with the Dade Thrombin Reagent accurately measures fibrinogen concentrations. Thus, together with the lower degree of hemodilution in our study (16%), it is of no surprise that the Clauss methods used in our study decreased to the same extent, both in absolute and in relative terms, after administration of 1 L of HES.
The electromechanical test measured higher concentrations than the ELISA and photometric test preoperatively as well as after infusion of 1 L of HES. Calibration with different reference plasma samples may explain this difference. In an investigation of the agreement of different Clauss-based tests, there were considerable between-center differences, probably due to calibration issues, 11 and there were also notable differences in the measured concentrations of the same standard (1st WHO International Standard). These findings emphasize the need for improved standardization of fibrinogen measurements. So our hypothesis that fibrinogen measurement methods may differ after HES hemodilution is refuted, as the photometric Clauss is higher from the beginning, and the relative changes after HES dilution are the same.
It has been previously found that FIBTEM-MCF correlates well with plasma fibrinogen concentrations. 9 However, FIBTEM-MCF is not only dependent on fibrinogen concentration but also on fibrin formation and its polymerization. Hemodilution with colloidal solutions, particularly with HES, has been shown to interfere with clot formation and polymerization, 12,13 and hemodilution with HES decreased FIBTEM clot strength more than the other solutions. 14 Thus, our present finding of a larger relative decrease in FIBTEM-MCF than fibrinogen plasma concentrations after in vivo hemodilution with HES corroborate previous in vitro findings. The FIBTEM assay and the fibrinogen measurement methods according to Clauss are all functional assays, unlike the immunoassay that measures fibrinogen concentration alone. In our study, the measured relative and absolute decrease in plasma fibrinogen after dilution with HES were the same with the immunoassay as with the 2 Clauss methods. In contrast, FIBTEM-MCF decreased more than the immunoassay. The FIBTEM-MCF differs from the Clauss methods in that the latter measures the initial formation of fibrin from fibrinogen, whereas the former measures the final or maximal fibrin clot strength. Thus, HES does not seem to affect the initial fibrinogen function to form fibrin as measured with these Clauss methods, whereas HES seems to impair the function of fibrinogen to form clots with maximal stability as measured with FIBTEM-MCF. Considering all this, FIBTEM-MCF is probably a valuable complement to fibrinogen concentration, at least if a colloid such as HES has been used. However, clinicians should be aware of the higher coefficient of variation (CV) with FIBTEM-MCF as compared with the fibrinogen concentration methods (see Table 2), both at baseline and after HES administration. Whether the higher CV represents a poor precision with the FIBTEM-MCF method or a biological variation in fibrinogen function remains to be investigated.
Neither baseline fibrinogen concentrations nor baseline FIBTEM-MCF was able to predict surgical bleeding. These findings probably reflect that bleeding in neurosurgery is more related to location of tumor (e.g., difficult resection close to major vessels) and tumor vascularity than to preoperative coagulation status. 15
There are several limitations in our study. First, this is a cross-sectional study, and it may have been preferable to include a control group receiving some solution other than HES and to compare the different methods used. Nevertheless, it still appears valuable to obtain a description of the effects of hemodilution with HES on these patients, in line with the clinical practice in our hospital. Second, we only studied mild-to-moderate hemodilution. At the same time, this represents, in fact, a more common clinical situation than the 30% to 50% hemodilution in the in vitro studies discussed earlier. Third, only 25 patients were included in the analysis. Our power analysis calculated 20 patients as being enough to reach a power of 80%. However, the power analysis was based on the results of the first 6 analyzed participants, which is an acceptable method with obvious limitations. Thus, more patients included in the study might have been able to detect differences between the different Clauss methods.
In conclusion, this study showed that, despite providing different fibrinogen concentration values at baseline, the relative decrease in the fibrinogen concentration after HES infusion was comparable among the 3 tests used to measure the fibrinogen concentration. Whole-blood fibrin-based clot quality was more critically affected by HES infusion. The relevance of these findings for clinical management requires further investigation, and issues on better standardization and calibration of various fibrinogen measurement methods need to be addressed.
Footnotes
Appendix A
The Enrolled 40 Patients Stratified into One Group of Patients Bleeding 0 to 500 mL and One Group Bleeding >500 mL.a
| Bleeding, mL | Number | Bleeding, median (range) | ELISA, g/L | Photometric, g/L | Electromechanical, g/L | FIBTEM-MCF, mm | EXTEM-MCF, mm |
|---|---|---|---|---|---|---|---|
| 0-500 | 23 | 250 (50-500) | 2.24 ± 0.48 | 2.31 ± 0.50 | 2.62 ± 0.58 | 13.2 ± 4.6 | 59.8 ± 6.2 |
| >500 | 17 | 1000 (550-2500) | 2.21 ± 0.50 | 2.36 ± 0.64 | 2.65 ± 0.68 | 11.7 ± 3.9 | 58.4 ± 6.2 |
Abbreviations: MCF, maximum clot formation; ELISA, enzyme-linked immunosorbent assay.
aBaseline (preoperative) results of all measured parameters are shown. None of the fibrinogen concentration measures or clot stability measures were significantly different between the 2 groups.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dag Winstedt received lecture fees from CSL Behring 2015. Cristina Solomon is an employee of CSL Behring and previously received speaker honoraria and research support from Tem International and CSL Behring, and travel support from Haemoscope Ltd (former manufacturer of TEG). Ulf Schött received research grants from CSL Behring 2012 and lecture fees from CSL Behring 2014.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Grants from Region Skåne (grant numbers: 194251, 356111).