
Abstract
The etiology of the prothrombotic state in myeloma has yet to be definitively characterized. Similarly, while recent evidence suggests that patients with monoclonal gammopathy of undetermined significance (MGUS) may also be at increased risk of thrombosis, the magnitude and the etiology of this risk have also yet to be defined. The present study aims to characterize patterns of plasma thrombin generation and sensitivity to the anticoagulant activity of activated protein C (APC) at the time of initial diagnosis of myeloma and in response to therapy in comparison to that observed among patients with MGUS and matched, healthy volunteers. Patients presenting with newly diagnosed/newly relapsed myeloma (n = 8), MGUS (n = 8), and matched healthy volunteers (n = 8) were recruited. Plasma thrombin generation was determined by calibrated automated thrombography. Peak thrombin generation was significantly higher in patients with myeloma (383.4 ± 33.4 nmol/L) and MGUS (353.4 ± 16.5 nmol/L) compared to healthy volunteers (276.7 ± 20.8 nmol/L; P < .05). In the presence of APC, endogenous thrombin potential was significantly lower in control plasma (228.6 ± 44.5 nmol/L × min) than in either myeloma (866.2 ± 241.3 nmol/L × min, P = .01) or MGUS plasma (627 ± 91.5 nmol/L × min, P = .003). Within the myeloma cohort, peak thrombin generation was significantly higher at diagnosis (353.2 ± 15.9 nmol/L) than following completion of the third cycle of therapy (282.1 ± 15.2 nmol/L; P < .005). Moreover, sensitivity to APC increased progressively with each cycle of chemotherapy. Further study of the etiology and evolving patterns of hypercoagulability among patients with these conditions is warranted and may have future implications for thromboprophylaxis strategies.
Introduction
Venous thromboembolism (VTE) remains a leading cause of death among patients with cancer. 1 Myeloma, a plasma cell neoplasm, has been consistently reported to be associated with a particularly high risk of VTE. 2 –4 The magnitude of this risk is reflected in current consensus guidelines which recommend the use of pharmacological thromboprophylaxis among affected patients in certain situations of high thrombotic risk, including among specific subgroups of ambulatory, nonhospitalized patients with myeloma. 5,6
The mechanisms underlying the prothrombotic state associated with this disease have yet to be fully characterized, although a number of potential causative factors have been postulated. Aberrant expression of tissue factor (TF) 7,8 ; enhanced plasma concentrations of factor VIII (FVIII), von Willebrand factor, and inflammatory cytokines 9,10 ; impaired fibrinolysis 11,12 ; procoagulant autoantibodies 13 ; and acquired resistance to the anticoagulant activity of activated protein C (APC) 14,15 have all been described in association with myeloma and may contribute to the prothrombotic phenotype.
The risk of VTE in myeloma appears to be particularly elevated at times of heightened disease activity, such as at diagnosis or at relapse. 5,6,16 Moreover, in addition to factors directly related to tumor biology, the risk of VTE in myeloma may be exacerbated through other mechanisms, including through factors related to specific antimyeloma therapies, which are frequently used in current practice. Therapeutic agents such as corticosteroids, 17 –20 anthracyclines, 21,22 and the novel immunomodulatory drugs, such as thalidomide, 23,24 are all thought to confer an additional risk of VTE, particularly when administered concurrently. 5,16 In addition, emerging evidence suggests that the VTE risk associated with the novel immunomodulatory agents may also be exacerbated by specific genomic predispositions, 25 with several studies demonstrating correlations between the incidence of thalidomide or lenalidomide-associated VTE and specific single nucleotide polymorphisms (SNPs) present in genes regulating inflammatory responses and DNA repair. 26 –28
It has yet to be conclusively determined whether a heightened risk of VTE also occurs in association with monoclonal gammopathy of undetermined significance (MGUS), a related benign condition. While a number of clinical studies suggest that affected individuals have a higher VTE risk than the general population 3,4,29 –31 and while recent data suggest that patients with MGUS have laboratory features (such as fibrinogen concentration, FVIII activity, and thromboelastography parameters), which appear to be intermediate between patients with myeloma and the general population, 32 the true magnitude of the heightened VTE risk in MGUS, if any, and the mechanisms underlying this risk have yet to be definitively characterized.
Calibrated automated thrombography (CAT) permits global assessment of multiple parameters of plasma thrombin generation in platelet rich or platelet poor plasma. 33 –35 While this research tool is not currently clinically validated for identification of patients with cancer at high risk of VTE, a number of investigators have reported correlations between certain specific parameters of plasma thrombin generation and risk of VTE. 36 –38
The present study aimed to characterize parameters of plasma thrombin generation among patients with myeloma and patients with MGUS in comparison to healthy volunteers and to investigate patterns of resistance to the anticoagulant activity of APC among the 3 groups. Moreover, we aimed to characterize evolving patterns of plasma thrombin generation among patients with myeloma in response to antimyeloma therapy.
Methods
Ethical approval to proceed with the study was granted by the local research ethics committee. The study was designed as a prospective cohort study where consecutive patients presenting with myeloma, patients with MGUS, and healthy volunteers were identified and recruited and asked to provide a sample of venous blood for analysis at baseline and following completion of consecutive cycles of antimyeloma therapy (in the case of patients presenting with myeloma). Inclusion criteria for participation in the study consisted of age greater than 18 years; a new diagnosis of myeloma or a diagnosis of relapsed myeloma requiring therapy; a diagnosis of MGUS or in the case of healthy volunteers, the absence of any evidence of myeloma/MGUS on serum protein electrophoresis. Exclusion criteria were a previous history of VTE or a bleeding disorder; the presence of hereditary thrombophilia; a history of malignancy other than myeloma; thrombocytopenia (platelet count < 50 × 109/L); liver disease; surgery within the month prior to recruitment; and exposure to an anticoagulant agent in the month prior to recruitment and exposure to antimyeloma therapy in the 6 months prior to recruitment.
The 2 distinct control groups (comprising participants with either MGUS or healthy volunteers) were matched to the subjects with myeloma based on age (±5 years), gender, smoking status, and body mass index.
Informed consent was obtained from each participant. Whole blood was collected into tubes containing citrate 0.105 mol/L by direct venipuncture using minimal tourniquet at baseline from all study participants and immediately following completion of the first three 28-day cycles of therapy from the participants with myeloma.
Additional samples for factor V Leiden (FVL) genetic analysis were collected into tubes containing EDTA. Samples were hand delivered to the laboratory where platelet poor plasma was immediately prepared from citrated whole blood by centrifugation.
Characterization of Parameters of Plasma Thrombin Generation
Plasma thrombin generation was assessed by CAT using a Fluoroskan Ascent Plate Reader (Thermo Lab Systems, Helisinki, Finland) in conjunction with Thrombinoscope software (Thrombinoscope BV, Maastricht, Netherlands) as described previously. 35,39 Briefly, in a 96-well round bottom polystyrene plate (Thermo Scientific Nunc, Massachusetts, USA), 80 µL aliquots of citrated platelet poor plasma were incubated with 20 μL of platelet-poor plasma reagent (low reagent; Thrombinoscope BV) containing 1 pmol/L TF and 4 μmol/L phospholipids (composed of 60% phosphatidylcholine, 20% phosphatidylserine, and 20% phosphatidylethanolamine) in the presence or absence of APC (human APC; 5-10 nmol/L; Haematologic Technologies Inc, Vermont, USA). Thrombin generation was initiated by automatic dispensation of a fluorogenic thrombin substrate (Z-Gly-Gly-Arg-AMC.HCl; Thrombinoscope BV) and 100 mmol/L CaCl2 into each well (final concentrations, Z-Gly-Gly-Arg-AMC.HCl, 0.42 mmol/L and CaCl2, 16.67 mmol/L), and assessment of thrombin generation parameters was completed using a thrombin generation standard. The lag time to initiation of thrombin generation, peak thrombin generation, time to peak thrombin generation, and the area under the thrombin generation curve (endogenous thrombin potential; ETP) was determined for each plasma sample. All experiments were performed in duplicate.
Detection of the FVL Arg506Gln Polymorphism
The FVL mutation status of all patients with myeloma and MGUS was ascertained by polymerase chain reaction using the Roche FVL kit and LightCycler1.2 Instrument in combination with LightCycler software 3.5. This kit allows detection and genotyping of the point mutation G to A at position 1691 of the human factor V gene from DNA isolated from human whole peripheral blood in EDTA.
Statistical Analysis
Data were described using mean and standard error of the mean for normally distributed variables or median and intraquartile ranges for nonnormally distributed variables. Statistical analysis was performed using the unpaired t test for normally distributed variables and a Mann-Whitney U test for nonnormally distributed variables. Statistical analysis was performed using Prism software (version 5.0).
Results
Eight participants with newly diagnosed or newly relapsed myeloma were identified and recruited from the cohort of patients attending the clinical hematology service of a large, university teaching hospital. Five of these patients had an immunoglobulin (Ig) G paraprotein and the remaining 3 had an IgA, light chain, and nonsecretory phenotype, respectively. Four participants among this cohort had relapsed disease: 2 of whom were previously treated with multiple lines of therapy (including combinations of alkylating agents, corticosteroids, proteasome inhibitor, and immunomodulatory agents), 1 patient was previously treated with a regimen incorporating an immunomodulatory drug in combination with corticosteroids, and 1 patient was treated with a regimen incorporating a combination of an alkylating agent, immunomodulatory agent, and corticosteroid. None of these 4 relapsed patients had received any myeloma therapy in the 6 months preceding recruitment.
Eight participants with MGUS and 8 healthy volunteers matched for age, gender, smoking status, and body mass index were also identified and recruited. No participant tested positive for the FVL Arg506Gln polymorphism. No participant was receiving treatment with either an anticoagulant or antiplatelet agent at the time of recruitment.
Six patients from the initial cohort who proceeded to receive myeloma therapy and 4 additional patients who were newly diagnosed with myeloma were recruited for assessment of thrombin generation parameters in response to therapy. Within this group, 7 patients had an IgG paraprotein and the remaining 3 had an IgD, IgA, and nonsecretory phenotype, respectively. Seven patients were treated with a regimen incorporating an immunomodulatory agent in combination with dexamethasone (all of whom received low-dose aspirin thromboprophylaxis for the duration of therapy). Of these, 4 received lenalidomide, 1 received thalidomide, and the remaining 2 were treated with pomalidomide, a novel immunomodulatory drug. The remaining 3 participants were treated with bortezomib in combination with cyclophosphamide and dexamethasone (2 of whom received low-dose aspirin thromboprophylaxis). Treatment was administered in 28-day repeating cycles. Plasma samples were obtained following completion of each cycle of therapy, immediately prior to commencing the subsequent cycle. In order to compare results from longitudinal samples generated at different time points, samples were tested in parallel with aliquots of a single control sample. Variability in peak thrombin generation and ETP measured in serial control samples at different time points was less than 5%.
Among participants with measurable disease, a progressive decline in serum paraprotein level and serum levels of the involved light chain component were observed in response to therapy (Table 1). At the point of completion of 3 cycles of therapy, 8 participants had achieved a partial response by International Myeloma Working Group (IMWG) consensus criteria 40 (no participant had achieved a complete response or very good partial response by IMWG criteria; 1 patient did not have measurable disease and so assessment of response was not determined at that point and in the case of 1 patient, results of serum paraprotein/light chains following cycle 3 were not available).
Serum Paraprotein and Serum Free Immunoglobulin Light Chain Levels at Baseline and in Response to Therapy.

Abbreviation: SEM, standard error of the mean.
aMean serum paraprotein and serum free light chains were lower than pretherapy levels at completion of each of the first 3 cycles of therapy.
Parameters of Plasma Thrombin Generation and Sensitivity to APC Prior to Commencing Therapy
Baseline peak thrombin generation was significantly higher in patients with myeloma (383.4 ± 33.4 nmol/L, P = .02) and MGUS (353.4 ± 16.5 nmol/L, P = .01) compared to healthy volunteers (276.7 ± 20.8 nmol/L; Figure 1A). A trend toward a higher mean ETP among patients with myeloma (2035 ± 171.1 nmol/L × min) compared to patients with MGUS (1935 ± 83.3 nmol/L × min, P = .6) and healthy volunteers (1817 ± 164.4 nmol/L × min, P = .4) was also observed, although this did not reach statistical significance (Figure 1B). No significant differences in lag time to initiation of thrombin generation and the time to peak thrombin generation were observed between the 3 groups (data not shown).
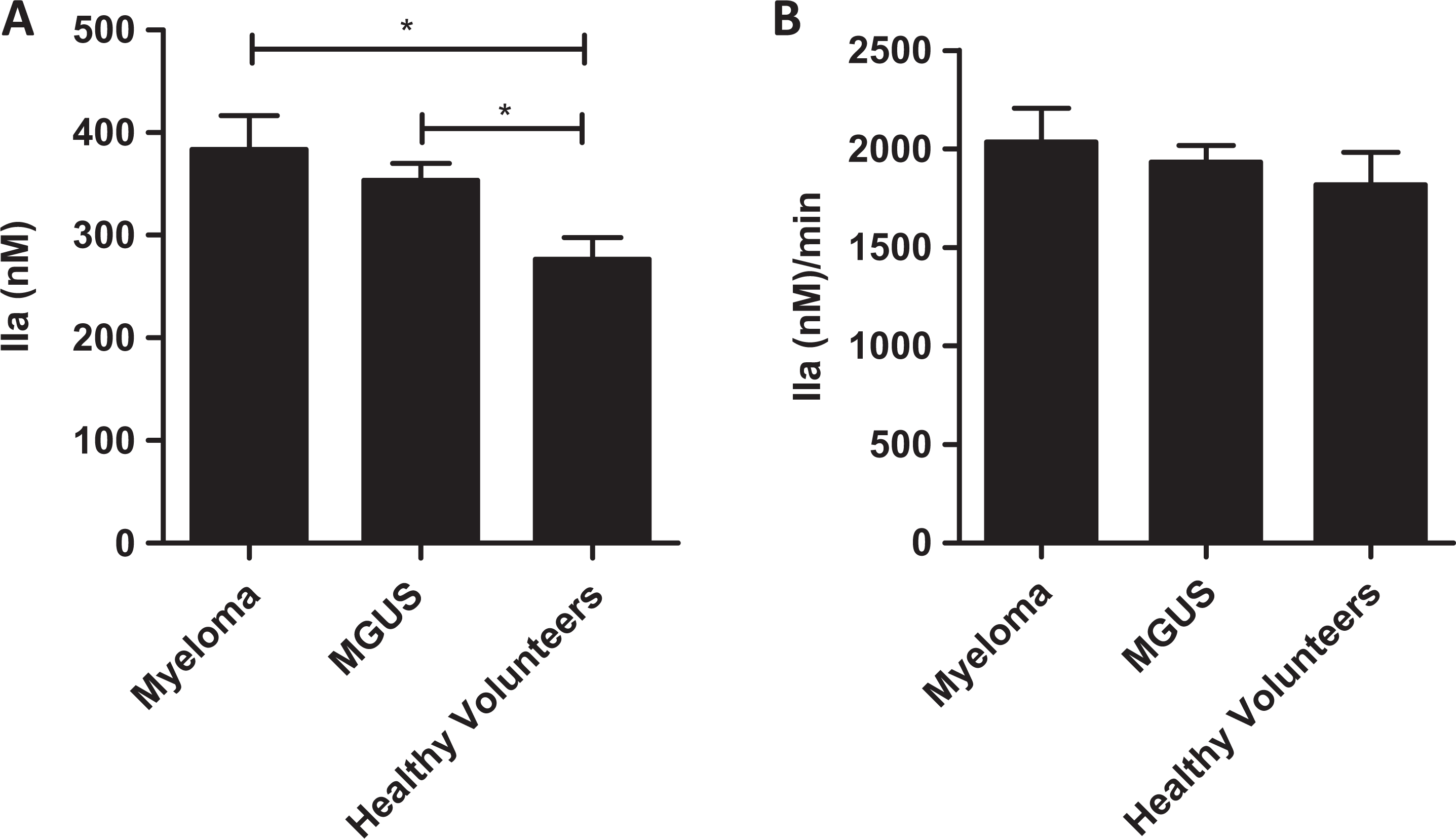
Baseline plasma thrombin generation is increased in patients with myeloma and monoclonal gammopathy of undetermined significance (MGUS) compared to matched healthy volunteers. Platelet poor plasma prepared from patients with myeloma (prior to commencing therapy), MGUS, and matched healthy volunteers was incubated with phospholipid vesicles (4 µmol/L; 60% phosphatidylcholine, 20% phosphatidylserine, and 20% phosphatidylethanolamine). Thrombin generation was initiated with 1 pmol/L sTF and 100 mmol/L CaCl2 and measured by comparing rate of fluorogenic substrate hydrolysis to a thrombin standard. Peak thrombin generated (A) and endogenous thrombin potential (ETP; B) were determined using Thrombinoscope software. All experiments were performed in duplicate. Results are expressed as mean ± standard error of the mean (SEM; unpaired t tests; *P < .05).
As expected, following incubation of plasma with APC, thrombin generation was attenuated in all 3 groups. However, in the presence of APC (10 nmol/L), mean ETP was significantly lower in control plasma (228.6 ± 44.5 nmol/L × min) than in either myeloma (866.2 ± 241.3 nmol/L × min, P = .01) or MGUS plasma (627 ± 91.5 nmol/L × min, P = .003), reflecting a more pronounced attenuation of ETP in controls (89.3% ± 3.1%) relative that observed among patients with MGUS (67.8% ± 4.3%) or myeloma (59.3% ± 8.9%; Figure 2A). Peak thrombin generation was attenuated by APC (10 nmol/L) to 54.8 ± 27.7 nmol/L in control, 111.2 ± 21.7 nmol/L in MGUS, and 149.1 ± 44.6 nmol/L in myeloma plasma. This again reflects a more pronounced sensitivity of control plasma to the anticoagulant activity of APC in contrast to MGUS and myeloma plasma, with APC attenuating baseline peak thrombin generation to 16.9% ± 9.8% in control, 29.7% ± 4.9% in MGUS, and 34.89% ± 8.9% in myeloma plasma (Figure 2B). Lag time to initiation of thrombin generation was more prolonged in the presence of APC in control plasma (23.8 ± 3.9 minutes) and MGUS plasma (23.7 ± 3 minutes) in contrast to that measured in myeloma plasma (21.7 ± 3 minutes). Similarly, the time taken to achieve peak thrombin generation was shorter in myeloma plasma (25.1 ± 3.1 minutes) and MGUS plasma (27 ± 2.8 minutes) compared to controls (29.4 ± 4 minutes).
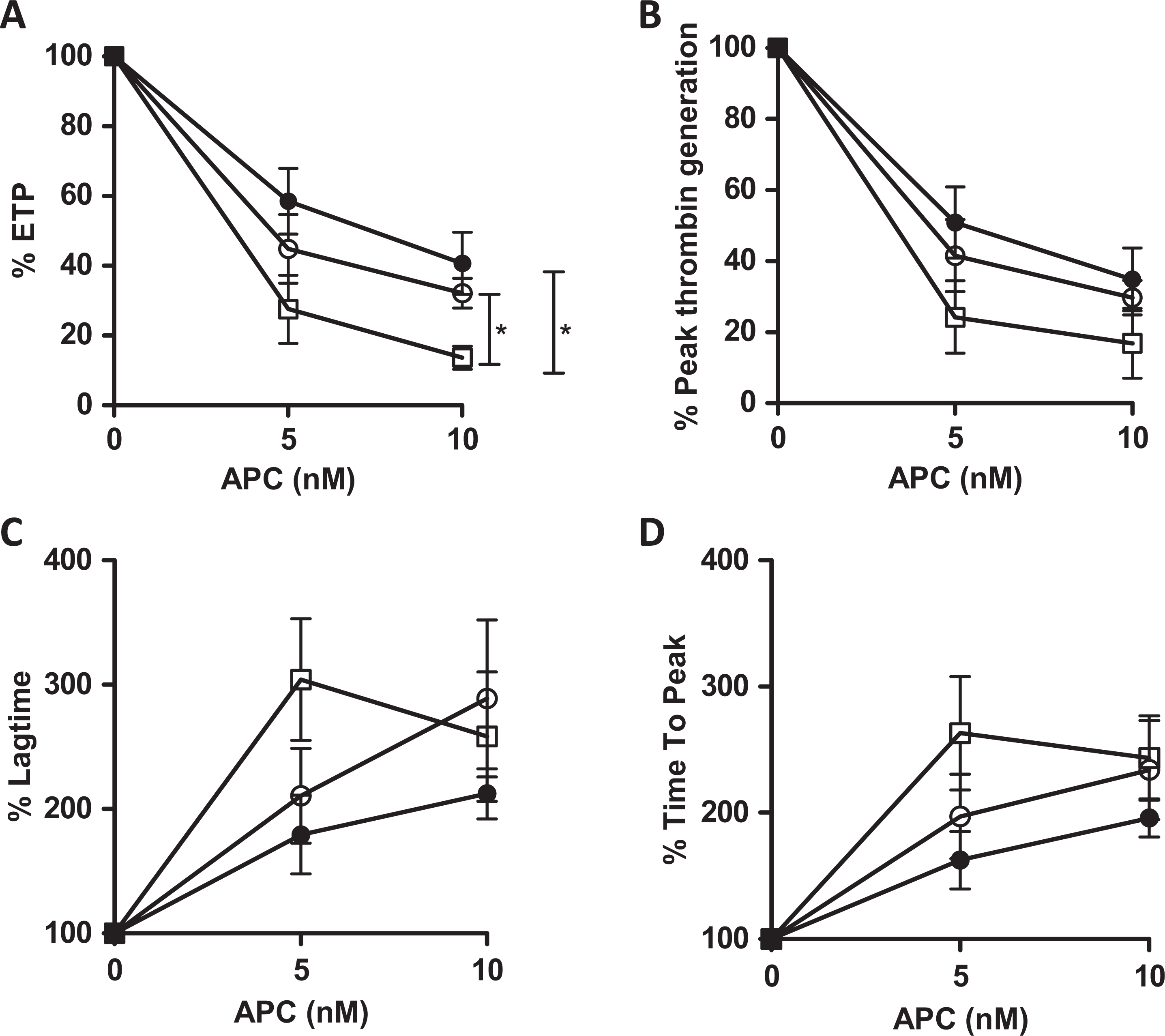
FVL-independent relative resistance to activated protein C (APC)-induced attenuation of thrombin generation in myeloma and monoclonal gammopathy of undetermined significance (MGUS) plasma compared to healthy matched volunteers. Thrombin generation was initiated with 1 pmol/L tissue factor (TF) in platelet poor plasma (healthy volunteers, □; MGUS, ^; myeloma, •) incubated with phospholipids in the presence of APC (0-10 nmol/L). APC-mediated attenuation of ETP (A) and peak thrombin generation (B) and APC-mediated prolongation of lag time (C) and time to peak thrombin generation (D) were determined as a percentage of each parameter in the absence of APC. All experiments were performed in duplicate. Results are expressed as mean ± standard error of the mean (SEM; unpaired t tests; *P < .05).
Evolving Patterns of Plasma Thrombin Generation and Acquired APC Resistance in Response to Myeloma Therapy
Among this group (n = 10), peak thrombin generation was significantly higher at diagnosis (353.2 ± 15.9 nmol/L) than following completion of the third 28-day cycle of therapy (282.1 ± 15.2 nmol/L; P = .005), with a nonsignificant trend toward progressive decline in peak thrombin generation from diagnosis to completion of cycles 1 and 2 (Figure 3A). A nonsignificant trend to progressive reduction in ETP from pretherapy (2001 ± 139.4 nmol/L × min) to following completion of the third cycle (1894 ± 96 nmol/L × min) was also observed (Figure 3B). No significant differences were observed in the lag time to thrombin generation and the time to peak thrombin generation between groups (data not shown).
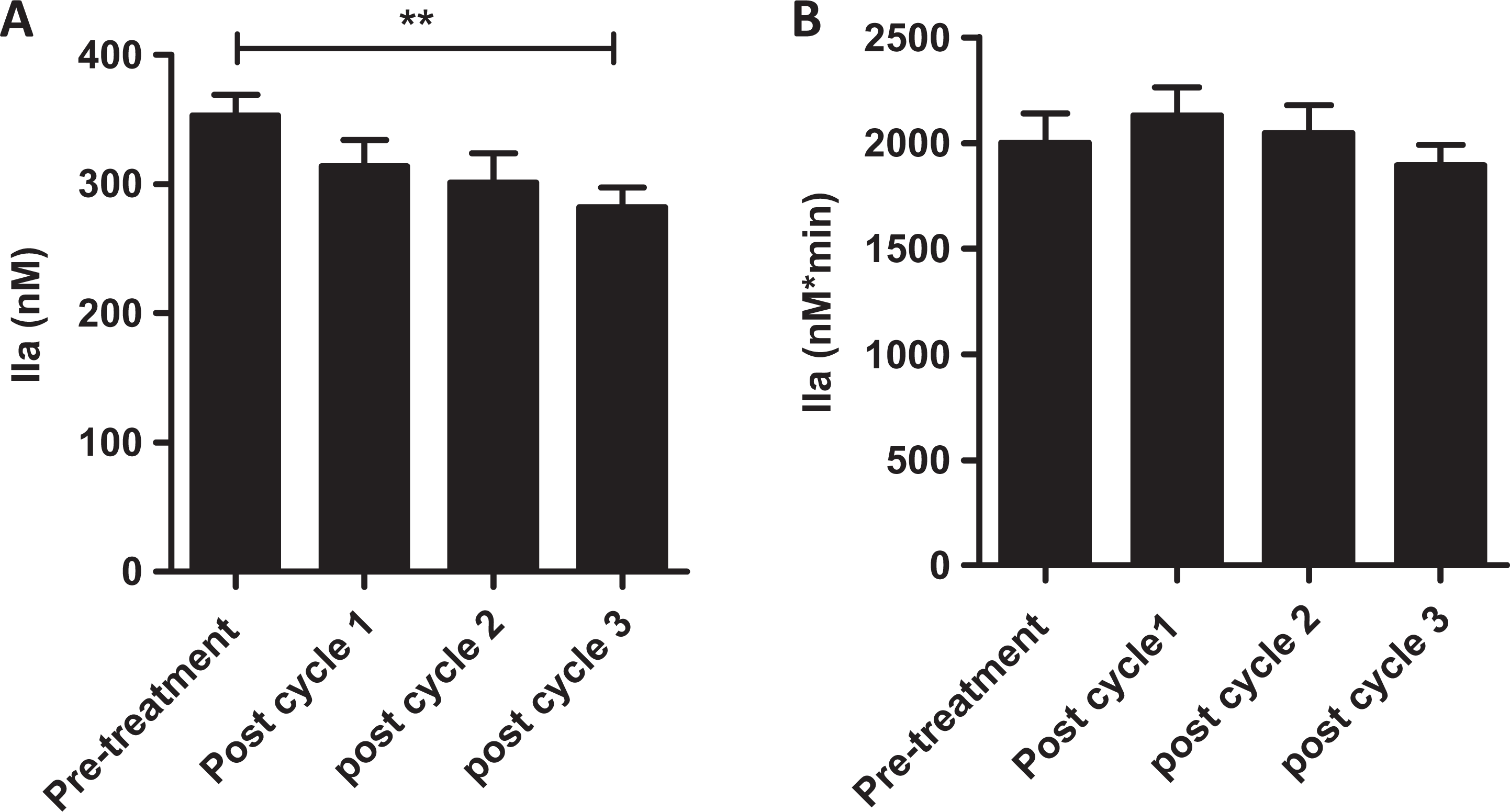
Plasma thrombin generation among patients with myeloma decreases in response to antimyeloma therapy. Thrombin generation was initiated as previously described in plasma obtained from patients with myeloma following completion of each 28-day cycle of myeloma therapy (cycles 1, 2, and 3). Peak thrombin generation (A) and endogenous thrombin potential (ETP; B) were determined for each sample using Thrombinoscope software. Experiments were performed in duplicate. Results are expressed as mean ± standard error of the mean (SEM; unpaired t tests; **P < .01).
Interestingly, sensitivity to exogenous APC increased progressively with each cycle of chemotherapy. In the presence of APC (5 nmol/L), ETP was significantly lower following completion of cycle 3 (685.2 ± 140.9 nmol/L × min) compared to before commencement of therapy (1227 ± 183.9; P = .03). Peak thrombin generated in the presence of APC (5 nmol/L) was also significantly lower following completion of cycle 3 (110.2 ± 26.6 nmol/L) compared to pretreatment (206 ± 31.3 nmol/L; P = .03). At baseline and following cycles 1, 2, and 3 of therapy, APC (5 nmol/L) suppressed ETP by 36.7%, 42.8%, 51.1%, and 58%, respectively (Figure 4A) and suppressed peak thrombin generation by 39.4%, 49.4%, 48%, and 57.7%, respectively (Figure 4B).
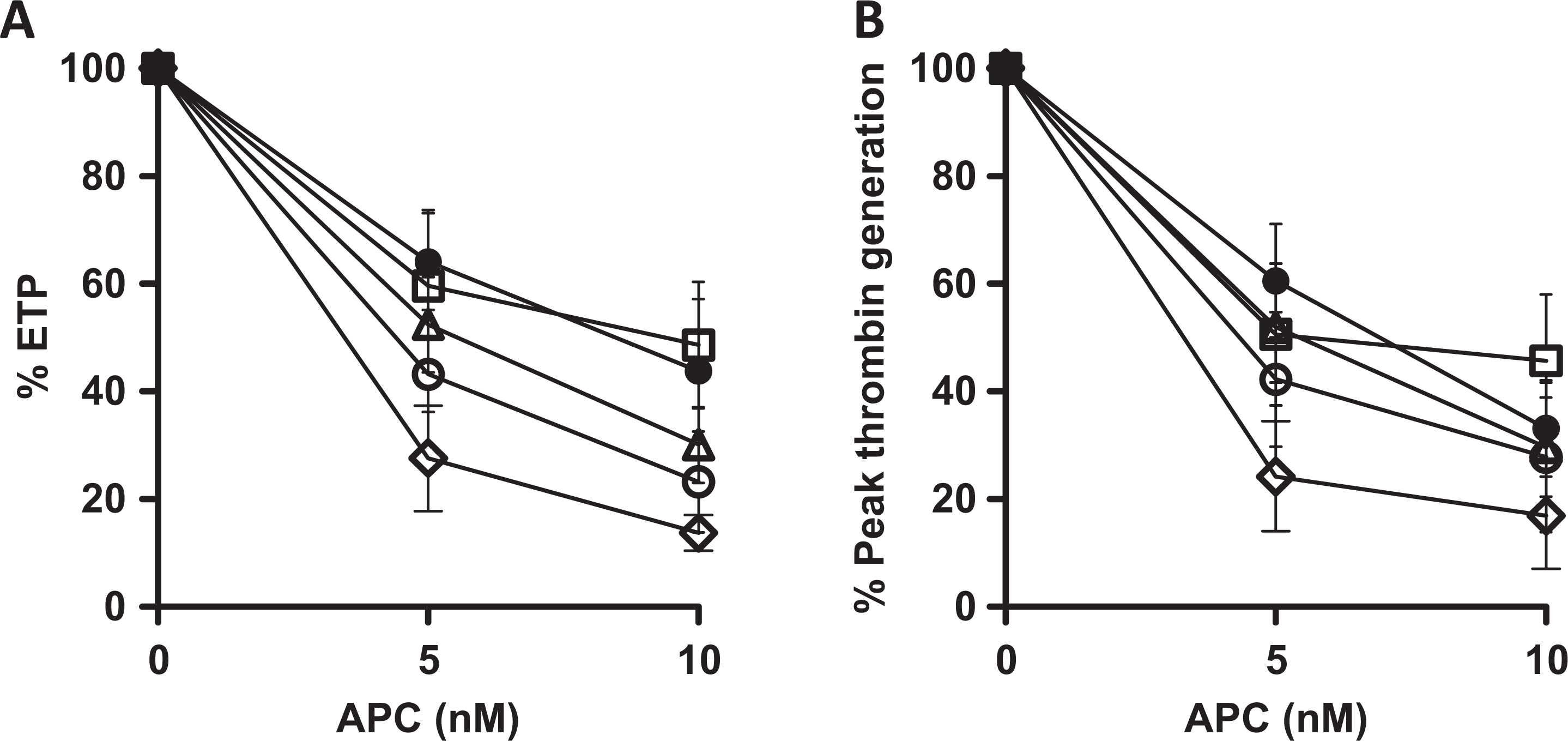
Sensitivity to the anticoagulant activity of activated protein C is enhanced in response to myeloma therapy. Thrombin generation was initiated with 1 pm tissue factor (TF) in platelet poor plasma obtained from patients with myeloma prior to commencing therapy and following completion of each of the first three 28-day cycles of therapy in the presence of activated protein C (APC; 0-10 nmol/L; pretherapy, •; cycle 1, □; cycle 2, Δ; cycle 3, ^; healthy volunteers, ◊). APC-mediated attenuation of endogenous thrombin potential (ETP; A) and peak thrombin generation (B) were determined as a percentage of each parameter in the absence of APC. All experiments were performed in duplicate. Results are expressed as mean ± standard error of the mean (SEM).
Discussion
While the risk of VTE among patients with myeloma has been well described, the molecular mechanisms underlying the etiology of the prothrombotic state in this disease remain to be fully elucidated. Previous investigators have reported evidence of enhanced microparticle-associated TF activity in plasma obtained from patients with myeloma and have suggested that this phenomenon may contribute to the increased VTE risk which occurs in this population. 7,8 Moreover, in vitro evidence also suggests that TF activity may be further enhanced in myeloma as a consequence of the effect of certain therapeutic agents, such as dexamethasone and anthracyclines, on TF expression. 18 Other studies have reported elevated plasma levels of specific proinflammatory cytokines, such as interleukin-6, occurring in association with evidence of increased coagulation activation in vitro and increased plasma concentrations of FVIII and fibrinogen. 9 However, the precise clinical implications of either of these observations and the magnitude of their effect on VTE risk in myeloma have yet to be accurately characterized.
A number of other investigators have postulated that the VTE risk in myeloma may arise as a result of prothrombotic properties attributed to the monoclonal Ig (paraprotein), which is secreted by the majority of neoplastic plasma cell clones. In vitro data suggest that this paraprotein may be implicated in fibrinolysis inhibition through a variety of mechanisms. These include prevention of normal fibrin polymerization, resulting in the formation of structurally abnormal fibrin polymers that are relatively resistant to the tissue plasminogen activator-plasmin pathway. 11,12 Others suggest that the paraprotein may act as a procoagulant autoantibody, exerting a lupus anticoagulant-like activity in vitro. 13,41 Again, the nature and magnitude of the thrombotic risk conferred by this phenomenon (if any) remain to be definitively determined. Interestingly, within our cohort, a single patient with a nonsecretory myeloma exhibited enhanced plasma thrombin generation relative to controls, suggesting that the etiology of the prothrombotic state in myeloma may not be limited to the influence of the paraprotein alone.
A large, Scandinavian-based population study demonstrated clear evidence for a genetic predisposition contributing to VTE risk in myeloma, specifically showing an enhanced risk of VTE in myeloma patients with a family history of VTE relative to that observed in patients with myeloma in the absence of a family history of VTE or among participants with a family history of VTE in the absence of a personal diagnosis of myeloma. 25 Interestingly, previous investigators have demonstrated correlations between SNPs present in specific genes involved in regulation of several cellular processes including DNA repair, inflammatory responses, and cytokine balance with the risk of thrombosis in patients exposed to the novel immunomodulatory agents such as lenalidomide 27 or thalidomide. 26,28 However, the precise mechanism underlying this apparent interaction and the implications of these findings for thromboprophylaxis strategies remain to be determined.
The APC pathway represents one of the primary natural inhibitors of blood coagulation. Resistance to the anticoagulant effect of APC has been shown to be associated with an increased clinical risk of thrombosis, and several previous studies have demonstrated evidence of acquired resistance to APC among patients with cancer. 14,42,43 Moreover, in a recent large single center retrospective study, investigators aiming to investigate the implications of acquired resistance to APC specifically among patients with myeloma reported that among their cohort of over 1100 patients, evidence of acquired resistance to the effects of APC (as determined by an APTT-sensitivity ratio) was identified in 6% of patients, a finding which was significantly associated with the risk of developing a VTE event. 15
The etiology of acquired resistance to APC remains unclear although some evidence exists to suggest that impaired APC sensitivity in cancer may, at least in part, arise from enhanced production of plasma coagulation factor V and FVIII. 44 Others have postulated that the myeloma Ig may exert an inhibitory effect on the APC anticoagulant pathway, 15,45,46 although the mechanism by which this may occur is unknown and such a phenomenon would fail to account for the presence of APC resistance among groups of patients with myeloma who do not secrete either a paraprotein or a paraprotein light chain fragment.
The results of the present study suggest that patients with myeloma exhibit enhanced plasma thrombin generation, reflecting the consistently reported observation in clinical studies that patients with this disease are at higher risk of developing VTE relative to the general population. We also demonstrate using the CAT assay that patients with myeloma exhibit reduced sensitivity to the anticoagulant activity of APC relative to that which is observed among healthy volunteers. We demonstrate that myeloma-associated elevated plasma thrombin generation and APC resistance reduce in response to myeloma therapy and are significantly attenuated following completion of 3 months of therapy. Current consensus guidelines recommend pharmacological thromboprophylaxis for subgroups of ambulatory patients with myeloma receiving treatment (provided the bleeding risk is favorable), although little evidence exists to guide duration of this therapy. 5,6 While the interpretation of our results is limited by the lack of a correlation with clinical outcomes, the suggestion that the thrombotic risk associated with active myeloma might diminish at an early stage of antimyeloma therapy reflects other recently published studies of evolving hypercoagulability in myeloma 47 and may have future implications for thromboprophylaxis strategies and patient risk stratification in this disease.
Conflicting clinical evidence exists with regard to the magnitude of VTE risk occurring in association with MGUS. In a Swedish population-based retrospective study incorporating data collected from records of over 5000 MGUS patients, investigators reported that MGUS was associated with a VTE risk which was three-fold greater than that observed among matched controls. 48 Similarly, an increased risk of VTE was reported among MGUS patients in a large hospital-based retrospective study of over 2000 patients 4 and in other smaller retrospective and prospective studies. 3,29 In contrast, previous investigators failed to detect an increased VTE risk in a number of other clinical studies, including a recent retrospective multicenter study incorporating data relating to over 1400 patients with MGUS. 30,31
In the present study, we report enhanced plasma thrombin generation and diminished sensitivity to the anticoagulant activity of APC among patients with MGUS relative to that measured in plasma obtained from age and gender-matched healthy volunteers. This finding reflects reports from a recent study which also demonstrated laboratory evidence of hypercoagulability among this population. 32 While the precise magnitude of VTE risk present in MGUS has yet to be determined, the growing body of clinical and laboratory evidence in support of the hypothesis that VTE risk is increased in this condition may have implications for current clinical practice, particularly for VTE risk stratification, where MGUS may not traditionally have been viewed as a significant risk factor for VTE.
Given that myeloma is relatively uncommon and primarily arises in the elderly among whom exclusion criteria for recruitment to this particular study were more likely to be present (eg, anticoagulant use), the population of potential participants available to us for recruitment was small, a factor which must be taken into consideration in the interpretation of our findings. However, while our study is limited by its small cohort size and as a consequence the lack of a correlation with the incidence of thrombotic events, our findings of enhanced plasma thrombin generation and APC resistance in a CAT assay in patients with both myeloma and MGUS that respond dynamically to therapy in patients with myeloma are novel. Moreover, further investigation of the evolving nature of the thrombotic phenotype among patients with myeloma receiving therapy, as was observed within our cohort, may lead to improvements in current thromboprophylaxis strategies, allowing greater accuracy in identifying patients at high risk as well as potentially avoiding prolonged exposure to anticoagulant therapies among individuals within whom thrombotic risk may have already diminished.
Footnotes
Authors’ Note
FNA was the principal investigator and takes primary responsibility for the study. MPC and BK (joint first authors) recruited the participants, performed laboratory and statistical analysis and wrote the article. SQ and KE performed laboratory analysis. OG and SOS contributed to the study concept and design. All authors have approved the final draft of the manuscript. This study was supported by an unrestricted research grant from Leo Pharma (MPC). MPC and BK contributed equally to the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MPC received an unrestricted research grant from LEO pharma in support of this study (see authors note above).