
Abstract
There are conflicting reports about the protective effect of hemophilia on the occurrence of ischemic heart disease. This study focuses on evaluation of heart function in patients with hemophilia. Cross-sectional, case–control study was done on all patients with hemophilia A or B who came to hemophilia center, and data were compared to controls. The data were collected from their charts, and heart function was evaluated by 2-dimensional, Doppler and pulse tissue Doppler. The serum troponin I level was measured in all patients as a marker of myocardial damage. Fifty patients with hemophilia took part in this study. All of them were male with mean age 29.1 years. Systolic blood pressure (mean = 121.52 ± 11 vs 115.61 ± 9.81, P = .038) and diastolic (mean = 81.94 ± 4.51 vs 75.21 ± 3.95, P = .042) blood pressure were higher in the patients. Five (10%) patients had systolic hypertension and 7 (14%) patients had diastolic hypertension. The M-mode echocardiography results showed that interventricular septum in diastole in patients with hemophilia (mean 1.143 ± 0.29) was significantly thicker than the control group (mean 0.828 ± 0.22, P < .001). Tissue Doppler echocardiography showed that late diastolic velocity of septum (Aa; P = .030), systolic velocity (S) of lateral mitral valve (P = .006), late diastolic velocity of lateral mitral (Aa) annulus (P = .038), and late velocity of (Aa) tricuspid (P = .004) had significant difference compared with the control group (P < .05). Troponin enzyme level was < 0.1 in all patients. Patients with hemophilia had higher blood pressure and more hypertension. Echocardiographic study of patients with hemophilia showed some increase in septal thickness and changes in diastolic dysfunction
Introduction
Hemophilia A and B are the most common severe inherited bleeding disorders. Hemophilia care had significant improvements within the past decade, and all of these improvements increased life expectancy in patients with hemophilia, resulting in age-related clinical problems. 1 –5
Cardiovascular disease has been reported as the second most common cause of death in patients with hemophilia in a study performed in the United States. High levels of factor VIII, which may occur during infusion of concentrate product, could increase the risk of ischemic heart disease in patients with hemophilia. 6 In addition, there are reports of increased prevalence of hypertension (HTN) in this population. 7
A study in the general population showed that tissue Doppler echocardiography is impaired in HTN, diabetes, and ischemic heart disease, independent of the result of conventional echocardiography. This suggests that tissue Doppler imaging may aid in the identification of patients at high risk. 8
The diagnosis of an acute myocardial infarction has been increasingly dependent on evaluation of cardiac biomarkers, especially cardiac troponins. Troponin release in the absence of necrosis may occur in conditions that produce increased myocyte membrane permeability. 9,10 Potential clinically useful role for troponin testing exists in tachycardia, left ventricular hypertrophy, heart failure, and pulmonary emboli.
This study focuses on evaluation of heart function in people with hemophilia by conventional echocardiography and pulse tissue Doppler echocardiography, and the serum troponin enzyme level was measured to detect possible myocardial damage in these patients.
Materials and Methods
A cross-sectional study was done on patients with hemophilia A or B who came to the hemophilia center of the referral hospital, Shiraz, Southern Iran, from April 2012 to April 2014, and data were compared to controls. Fifty patients with hemophilia who had no history of congenital heart, renal, or metabolic disease under regular follow-up were included in this study. The following data were collected from the patient’s charts by a physician: age, sex, blood pressure, hemophilia type, factor level, age at diagnosis, age at start of treatment, type of treatment (receiving fresh frozen plasma, cryoprecipitate, factor VIII, or factor IX), amount of factor usage per year, duration of factor usage, and history of thrombosis or infarction in patient or family. All of the patients were in on-demand therapy.
For each patient, a blood sampling was taken for serum troponin enzyme level, which was measured by VIDAS Troponin I (Ultra, made by BIOMERIEUX, France) kit. This study was approved by the medical ethics committee of Shiraz University of Medical Sciences, and written informed consent was obtained from the patients or parents.
The study also included 50 age-matched normal participants. These participants had no personal or family history of cardiac disease, hematologic disease, and endocrine disease. Echocardiography was performed by the same cardiologist and by the same protocol in the control group.
Blood pressure was obtained by auscultatory technique and mercury sphygmomanometer continuous, using the first and fifth phases of the Korotkoff sounds. Hypertension was defined as prior physician diagnosis of HTN and use of antihypertensive medication or systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg.
Echocardiographic Methods
Echocardiography was performed with a GE Vivid 3 echocardiographic machine (GE Vingmed, Horten, Norway) using a 3-MHz probe with pulsed Doppler tissue imaging software. All M-mode, 2-dimensional, Doppler and pulse tissue Doppler echocardiographic measures were performed on patients and control group by 1 qualified cardiologist.
Ejection fraction, shortening fraction, and septal and posterior wall thickness in systole and diastole were measured in the left parasternal long-axis view.
The pulsed Doppler sample volume was placed at the mitral valve and tricuspid tips, and 3 cardiac cycles were recorded from the apical window. Early (E) and late (A) peak velocities (m/s) and their ratio were determined for evaluation of diastolic function. Pulsed tissue Doppler imaging was obtained with the sample volume placed at the lateral corner of the mitral annulus, on the medial (or septal) and tricuspid corner in the apical 4-chamber view, and then at the anterior and posterior wall in the parasternal short-axis view. In each region, systolic (S) wave, early (Ea) and late (Aa) diastolic velocities, and ejection time were recorded.
Statistical Analysis
The numeric data are presented as mean ± standard deviation. The t test was used to compare echocardiographic data. The 1-sample, Kolmogorav-Smirnov test was used to define the distribution of variables. A P value less than .05 was considered significant for all of the statistical tests.
Sample size calculation
An exploratory study was performed. The sample size could not be calculated exactly because there are no valid assumptions among HTN, cardiac function, and cardiac biomarkers in patient with hemophilia. Based on the reported prevalence of 31.8% for HTN in 18- to 44-year-old patients with hemophilia documented by von Drygalski et al, 11 α = .05 and precision = 13% were calculated by Power SSC (Habibzadeh F, Shiraz NIOC Medical Education and Research Center, Shiraz, Iran) software for 50 patients.
Results
Fifty patients with hemophilia, 42 (84%) of whom were hemophilia A and the others were hemophilia B (16%), took part in this study. Among them, 52% of the patients had severe hemophilia (factor level <1%), 25% had moderate hemophilia (factor level 1%-5%), and 23% had mild hemophilia (factor level >5%), all of them were male with mean age of 29.1 years old (Table 1).
Demographic Data of Patients With Hemophilia A and B.

M-Mode Echocardiography
Results of M-mode echocardiography showed that interventricular septum in diastole in patient with hemophilia (mean 1.143 ± 0.29) had significant difference compared with control group (mean 0.828 ± 0.22; P < .001). Other measured M-mode echocardiographic parameters are shown in Table 2. M-mode echocardiographic parameters had no statistically significant correlation with factor level.
M-Mode Echocardiographic Parameters in Patients and Controls.
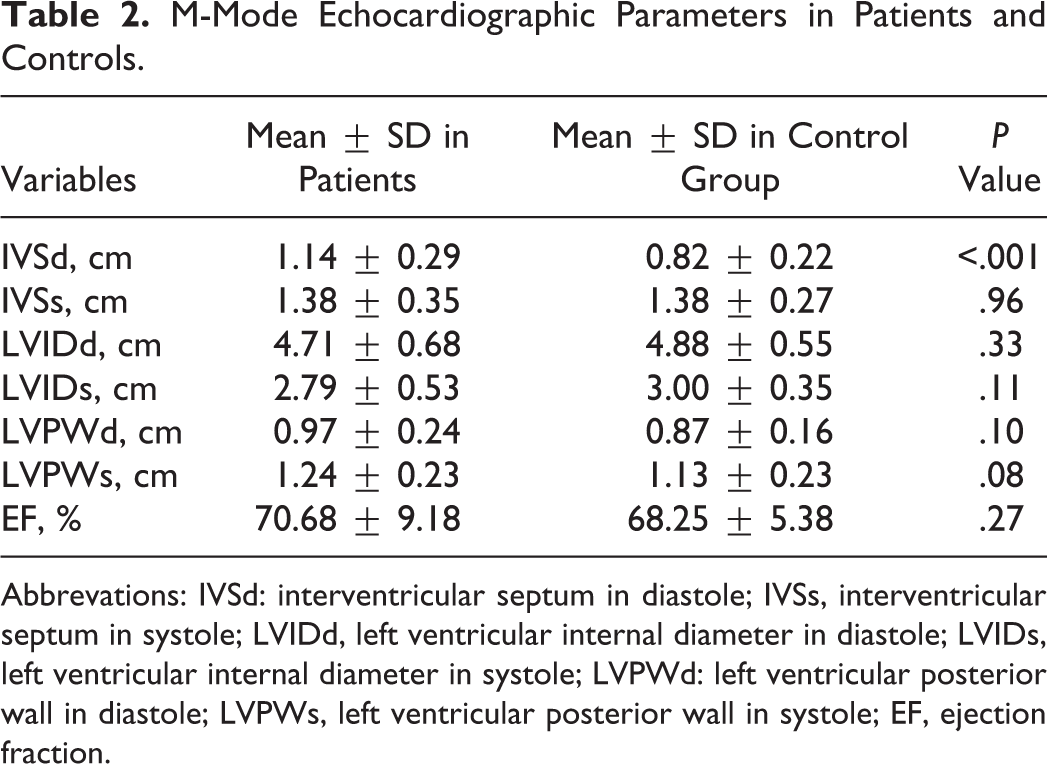
Abbrevations: IVSd: interventricular septum in diastole; IVSs, interventricular septum in systole; LVIDd, left ventricular internal diameter in diastole; LVIDs, left ventricular internal diameter in systole; LVPWd: left ventricular posterior wall in diastole; LVPWs, left ventricular posterior wall in systole; EF, ejection fraction.
Doppler Study
Late diastolic velocity of tricuspid valve was significantly lower in patients (Table 3). In the patients, 9 (18%) E/A ratio of mitral was less than 1 (impaired relaxation pattern) and 10 (20%) was more than 2 (restrictive filling pattern). In the control group, E/A ratio of mitral was between 1 and 2. E velocity of mitral (P < .05, r = −.68) and A velocity of mitral (P < .05, r = .48) had significant correlation with duration of treatment.
Doppler Study Parameters in Patients With Hemophilia and Controls.
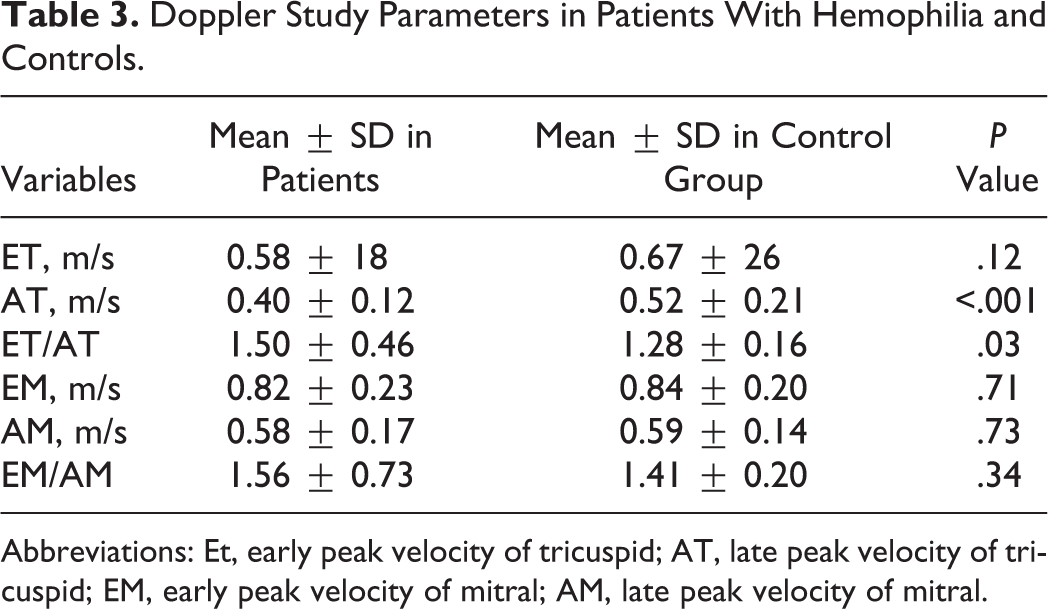
Abbreviations: Et, early peak velocity of tricuspid; AT, late peak velocity of tricuspid; EM, early peak velocity of mitral; AM, late peak velocity of mitral.
Tissue Doppler study
Tissue Doppler echocardiography showed that late diastolic velocity of septum (Aa) septum (P = .030), systolic velocity (S) of lateral mitral valve (P = .006), late diastolic velocity of lateral mitral (Aa) annulus (P = .038), and late velocity of (Aa) tricuspid (P = .004) had significant difference compared with the control group (P < .05). The tissue Doppler parameters are shown in Table 4.
The Tissue Doppler Parameters in Patients With Hemophilia and Controls.
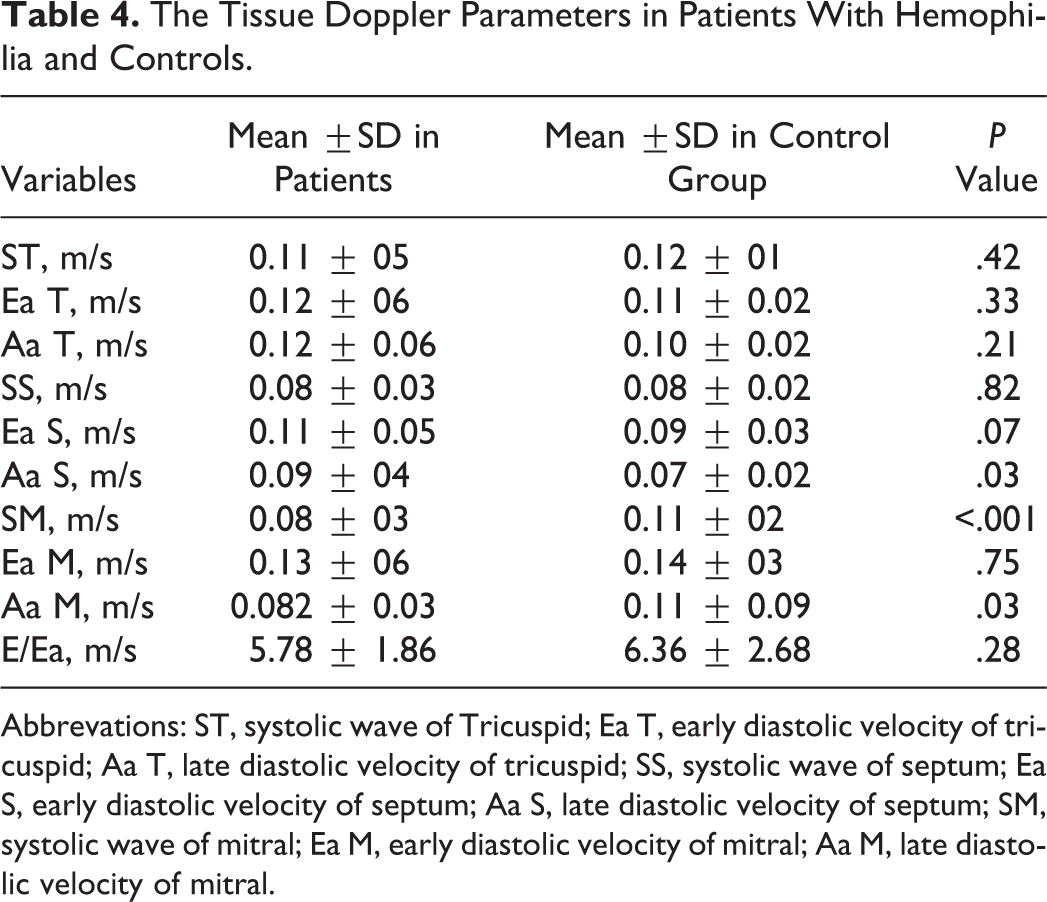
Abbrevations: ST, systolic wave of Tricuspid; Ea T, early diastolic velocity of tricuspid; Aa T, late diastolic velocity of tricuspid; SS, systolic wave of septum; Ea S, early diastolic velocity of septum; Aa S, late diastolic velocity of septum; SM, systolic wave of mitral; Ea M, early diastolic velocity of mitral; Aa M, late diastolic velocity of mitral.
The Ea mitral (P < .05, r = −.59) had significant correlation with duration of treatment. There was no significant change between echocardiography parameters in patients with factor VIII deficiency and factor IX deficiency. Troponin enzyme level was less than 0.1 in all patients. There was not a statistically significant correlation between troponin level, age, and treatment duration (P > .05).
Systolic blood pressure (mean = 121.52 ± 11 vs 115.61 ± 9.81, P = .038) and diastolic (mean = 81.94 ± 4.51 vs 75.21 ± 3.95, P = .042) blood pressure were measured in all of the patients and controls. Five (10%) patients had systolic HTN for age, and 7 (14%) patients had diastolic HTN.
Measurements of systolic blood pressure showed significant correlation with end-diastolic volume (P < .05, r = .34), S wave velocity of septum (P < .05, r = −.48), S wave velocity of mitral (P < .05, r = −.052), E wave velocity of mitral (P < .05, r = .33), E/A tricuspid (P < .05, r = −.39), E/A mitral (P < .05, r = −.39), and E/Ea mitral (P < .05, r = .43).
Measurements of diastolic blood pressure showed significant correlation with E wave velocity of tricuspid (P < .05, r = .43), A velocity of tricuspid (P < .05, r = .44), and E/Ea mitral (P < .05, r = .57). Comparison between patient with severe factor deficiency and mild factor deficiency showed statistically significant difference in blood pressure, M-mode, Doppler, and tissue Doppler parameters (P > .05).
Discussion
Improvements in hemophilia care have resulted in increases in median life expectancy in patients with hemophilia A and B. Older patients with hemophilia have the same medical conditions associated with aging in the general population, including cardiovascular disease. 12
In 1 study about risk factors for heart diseases among males with hemophilia, it was demonstrated that persons with hemophilia have risk factors (such as infection with HIV) that may predispose them to heart disease as their life expectancy increases. 6
Recent studies suggested that hemophilia does not have a preventative effect, and FVIII deficiency delays but does not eliminate the early phase of atherosclerosis. 13,14 Another recent study demonstrated that the incidence of ischemic cardiovascular disease in patients with hemophilia is increasing, despite the relative protection against ischemic heart disease mortality. 15
An association between hemophilia and HTN was described in a Dutch cohort in 1980. 16 A study in European cohort by Fransen van de Putte et al 7 showed a significantly higher prevalence of HTN in patients with hemophilia compared to normal men in national health registries. The prevalence of HTN in patients with hemophilia is higher than in the general population. The cause of this increased prevalence is unknown. In patients with hemophilia aged 30 years or older, blood pressure measurements should be part of standard care. 7
In our study, blood pressure was significantly higher in patients with hemophilia, 10% of the patients had systolic HTN for age, and 14% had diastolic HTN. Our study did not show difference in HTN in severe factor deficiency, but in a study by Drygalski et al, HTN was higher in patients with severe hemophilia than in those with milder form, similar to hemophilia A and B, associated with BMI and age, and not associated with HIV. In their study, the prevalence of HTN increased with age for the study participants. This difference may be due to small sample size for comparison between the groups.
In prolonged ischemia, myocytes are irreversibly damaged, and the cell membrane degrades, followed by the gradual release of myofibril-bound cytosolic complexes. However, it is possible that cardiac troponins can also be released into the circulation without myocyte necrosis.
In this study, we measured troponin I as a marker of myocardial damage which was in normal range in all patients. Troponin release in the absence of necrosis may occur in conditions that produce increased myocyte membrane permeability such as sepsis and other inflammatory states. With increased membrane permeability, those smaller troponin fragments could be released into the systemic circulation. In addition, in cardiomyopathy, tachycardia, left ventricular hypertrophy, pulmonary emboli, and renal dysfunction measurement of serum troponin level can be helpful. 9,17 –20
Heart function was evaluated in patients with hemophilia and compared with the control group. In M-mode echocardiography, the results show that interventricular septum in patients with hemophilia was thicker than in the control group. These findings may be due to higher blood pressure in these patients which can affect septal thickness and diastolic velocities. 7
Although Aa wave velocity of septum, S wave velocity of mitral, Aa wave velocity of mitral, and A wave velocity of tricuspid had significant difference compared with the control group (P < .05), the changes of which were within the normal range for age of the patients, and the significance of these diastolic changes require further study. Abnormal diastolic dysfunction was found in significant number of patients, which can also be explained by effect of HTN on heart and hypertrophy of ventricles, but this changes needs more investigation. Of the patients, 18% had abnormal relaxation pattern in Doppler echocardiography. An impaired relaxation pattern is characterized by a reduced E velocity, an E/A ratio < 1. Hypertension, coronary artery disease, and cardiomyopathy can impair left ventricular relaxation. Patients with impaired relaxation may be asymptomatic at rest but have reduced exercise tolerance, as tachycardia reduces the diastolic filling period leading to a rise in left atrial pressure and a reduction in stroke volume. Of our patients, 20% had restrictive filling pattern. Restrictive filling occurs when a further rise in left atrium pressure leads to an increased E/A ratio (≥2) in patients with heart failure as well as in the postmyocardial infarction setting. 21,22 No significant change was noted between factor VIII and factor IX deficiencies in echocardiography parameters.
Conclusion
Patients with hemophilia had higher blood pressure and HTN. Echocardiographic study of patients with hemophilia showed some increase in septal thickness and diastolic dysfunction of these patients which need longer and close follow-up.
Limitations of the Study
The studied patients were relatively young to study the effect of atherosclerosis and coronary ischemia on heart function.
Footnotes
Acknowledgments
We would like to thank Shiraz University of Medical Sciences for financial support. This article is relevant to the thesis of M. Fath with Project no.4950. Also, we thank Sheryl Nikpoor for editing and improving the use of English in the manuscript and Shirin Parand for preparation of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.