
Abstract
Objective:
To investigate all cases of isolated factor VII (FVII) deficiency as gathered from personal files or by a PubMed search.
Patients and Methods:
Personal files dealing with patients studied in Padua during the years 1970 to 2010 were reevaluated. The PubMed search was time unlimited and was carried on 2 occasions during 2014. Cross-checking of the references, listed in every article, was also carried out to avoid omissions. Inclusion criteria were isolated FVII defect of less than 40% of normal, negative coagulation pattern in the family, normal level of other vitamin K-dependent clotting factors, and normalization of the clotting factor after the therapeutic procedures, unless the patient died.
Results:
Twenty-nine patients met the inclusion criteria (18 male and 9 female, in 2 cases gender was unreported). This number included 1 personal case. Mean age was 37.9 (range 3-80). Underlying diseases were the following: neoplasia, infections, polytrauma, penicillin administration, nephrotic syndrome Wiskott Aldrich syndrome, and left heart failure (1 case, each); 2 patients had no underlying disease. Bleeding was variable but usually mild. There were 11 fatalities.
Conclusions:
Isolated FVII deficiency is a rare defect, which appears to be a finding associated with several morbid conditions, especially sepsis and tumors. This indicates the need for a careful investigation of even a mild prolongation of prothrombin time, especially when fibrinogen and partial thromboplastin time are normal.
Acquired bleeding conditions are often the result of deficiencies of several clotting factors. Acquired isolated defects of clotting factors are rare conditions. The most widely known is the factor X (FX) deficiency associated with amyloidosis. 1 –3 Neoplastic disorders are often associated with clotting abnormalities and bleeding or thrombosis. The most frequent changes are thrombocytopenia (acute leukemias), disseminated intravascular coagulation (promyelocytic leukemia and several solid tumors), thrombocytosis (myeloproliferative disease [MPD]), and thrombophilic state (lung and pancreas tumors). These are well-recognized conditions, and the caring physicians are aware of the possible occurrence. However, there are other conditions associated with clotting defects, which are often ignored or unrecognized. 4,5 This is due to the fact that the defect, for example, FVII deficiency, may be only mild to moderate and be reflected only by a minor prolongation of the prothrombin time (PT). The correct diagnosis may be missed if the treating physician does not request specific coagulation factor assays to investigate the isolated prolongations of the PT.
Sometimes the term paraneoplastic syndrome is used to define some of these conditions. However, the definition is not correct since it is not known whether the criteria of a paraneoplastic syndrome is always present (effect mediated by a known or unknown hormone-like substance).
Besides neoplastic diseases, there are other conditions such as sepsis or the appearance of antibodies that may be responsible for isolated FVII deficiency. 6,7 The purpose of the present study is to discuss all reported cases of acquired FVII deficiency including a personal case so that everybody may become aware of the problem. This may have a great clinical significance in view of the observation that the occurrence of an isolated FVII defect may have an important clinical significance.
Patients and Methods
Patients with an isolated acquired FVII deficiency have been gathered by a time-unlimited PubMed search using several key words. Side Tabs and MESH words supplied by PubMed were also evaluated. The search was carried out in February 2014 and again in September 2014. Personal files pertaining to patients with FVII deficiency studied in the Department of Medicine of Padua Medical School during the years 1970 to 2010 were also evaluated.
Inclusion criteria were the following: (1) lack of inheritance of the defect and normal coagulation pattern in the family; (2) lack of liver disease (including bilirubin metabolism disorders), malabsorption, or anti-vitamin K anticoagulant therapy; (3) specific FVII activity assay of less than 40% of normal together with normal levels of the other vitamin K-dependent factors; and (4) disappearance or improvement of the defect after the therapeutic procedures undertaken, unless the patient died. The evaluation of FVII antigen was not considered as an obligatory feature for inclusion. Exclusion criteria, on the contrary, were (1) cases of combined defects and (2) cases in which there was no documentation of the disappearance of the defect after therapy. Needless to say that this did not apply to fatal cases; (3) patients with an FVII level greater than 40% of normal.
Original articles were obtained through the help of the Pinali Medical Library of our University. Cross-checking of the references listed at the end of each article was carried out, independently, by 2 of us, to avoid omissions. The personal observation is the following: the propositus was a 34-year-old male who had a negative family and past medical history. Both parents had normal FVII levels. He was a light smoker (less than 10/d) and drank a moderate amount of wine (less than 2 glass of wine/d). About 3 months prior to admission to a hospital, he started complaining of palpitation, insomnia, and occasional cough or respiratory distress, especially when lying in bed. There was no sputum or hemoptysis and no fever. Routine laboratory tests, which included thyroid function studies, revealed no abnormalities, and the patient was given some bed time sedation and asked to stop drinking coffee.
The picture seemed to stabilize for a few weeks but then palpitation reappeared together with occasional shortness of breath. For the persistence of these symptoms, he was admitted to a local hospital where an electrocardiogram showed occasional polytopic extrasystole, while a chest X-ray revealed the presence of multiple nodular formations in both lungs. Still, there was no hemoptysis but a low-grade fever and a mild productive cough were now present. Cytology of sputum revealed the presence of large cells which could not be defined. Fever persisted and the patient felt fatigued. Liver and renal function tests were negative. There was no anemia but a mild neutrophilic leukocytosis was present. Prothrombin time was 18.1 (N 13-14 seconds). Partial thromboplastin time was normal. A transthoracic echocardiogram was negative. A subsequent transesophageal ecography revealed the presence of a mass in the right atrium. The mass was about 2 cm in diameter, had irregular contours, and seemed attached to the lateral-posterior wall of the atrium. The suspicion of atrial myxoma with pulmonary metastasis was formulated.
At this time, the patient was seen in consultation by one of the authors (AG). The PT was again mildly prolonged (18.5) but was corrected by the addition of even 20% of normal plasma. Specific clotting assays revealed an FVII of 10% of normal, while FII, FIX, FX, and PS were normal, and protein C was borderline low (60%). Platelet count was normal while fibrinogen was slightly elevated, and the
Results
Twenty-nine patients met the criteria for inclusion. 4 –25 This number includes the personal case (Table 1). Nine patients were excluded because of the presence of a combined defect with other clotting factors; suspicion of a congenital form; FVII levels higher than 40%; presence of abnormal liver function tests; concomitant presence of low FII, FIX, FX, protein C, or protein S; and lack of disappearance of defect after therapy.
Patients With Acquired FVII Deficiency.
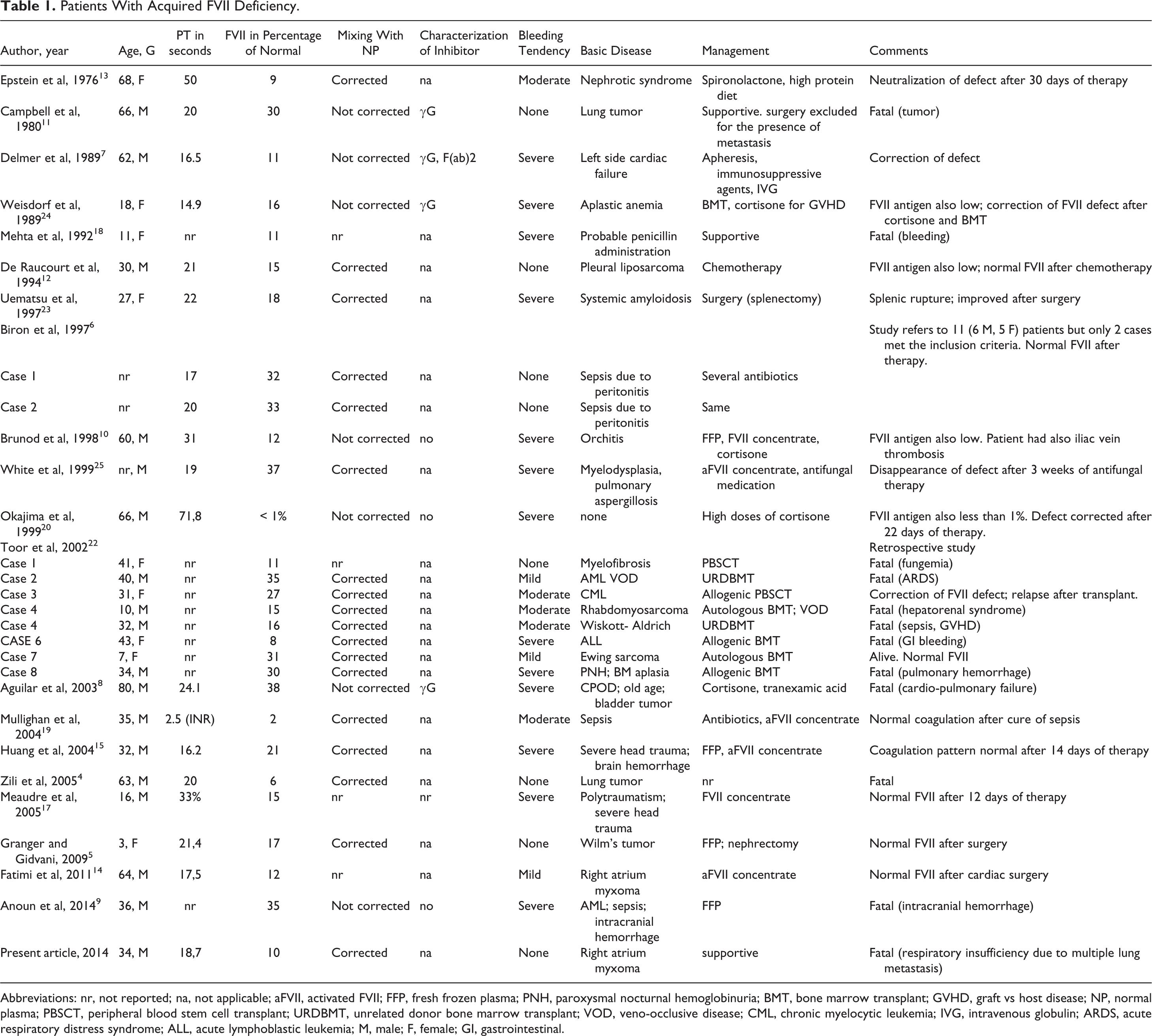
Abbreviations: nr, not reported; na, not applicable; aFVII, activated FVII; FFP, fresh frozen plasma; PNH, paroxysmal nocturnal hemoglobinuria; BMT, bone marrow transplant; GVHD, graft vs host disease; NP, normal plasma; PBSCT, peripheral blood stem cell transplant; URDBMT, unrelated donor bone marrow transplant; VOD, veno-occlusive disease; CML, chronic myelocytic leukemia; IVG, intravenous globulin; ARDS, acute respiratory distress syndrome; ALL, acute lymphoblastic leukemia; M, male; F, female; GI, gastrointestinal.
Age varied between 3 and 80 (mean age 37.9). In 3 cases, age was not reported, and 18 were male and 9 female. In 2 cases, gender was not reported. The underlying disease was neoplastic in 14 instances, infectious in 7 cases, including a case of orchitis, polytraumatism in 2 instances, penicillin administration in 1 patient, nephrotic syndrome in 1 case, and Wiskott-Aldrich syndrome (1 case) and left cardiac failure in another. In 2 cases, there was no apparent underlying disease. The tumors involved were lung or pleura, 2 hematological malignancies including amyloidosis (6 patients), kidney or bladder (2 cases), heart, 2 bone, 1 and muscle. 1 Bleeding was variable: mild or moderate in 8 cases and severe in 13 cases, respectively. Eight patients showed no bleeding tendency. Bleeding was the cause of death in 3 cases (gastrointestinal bleeding, pulmonary hemorrhage, and cerebral bleeding). In total, there were 11 fatalities. 4,8,9,11,18,22 These were due, besides bleeding, to severe sepsis with consequent multiple organ failure or to tumors, especially hematological ones.
Management tended to tackle the underlying disease and to eliminate the cause of the low FVII levels. It varied according to the etiology. Treatment of sepsis was of foremost importance and a wide range of antibiotics were used. Cortisone and other immunosuppressive agents were used in case of immunological conditions. Chemotherapy of neoplasia was also carried out with success in a few cases. Surgical removal of tumor was also carried out (cardiac myxoma, Wilms tumor).
In patients with bleeding fresh frozen plasma, FVII, or activated FVII concentrates, apheresis and bone marrow transplant were used. In occasional cases, the FVII level returned to normal, spontaneously. Unfortunately, the high rate of death precluded a complete evaluation of the therapeutic measures undertaken.
Discussion
Acquired defects of the clotting factors are common and usually multiple. Acquired defects of a single clotting factor are less frequent and deserve an extensive investigation. The most frequent are acquired hemophilia and acquired Von Willebrand disease. However, these conditions are not associated with a prolonged PT.
Acquired isolated FVII deficiency is rare since only 29 cases have been documented so far. This is in sharp contrast with congenital FVII deficiency, which seems much more frequent, being the most frequent disorder among the rare coagulation defects. 26 –29 Due to the higher prevalence of congenital forms of FVII defects when compared to acquired ones, it could be speculated that some of the probands could have a congenital defect, especially those for whom, because of death, no posttherapy disappearance of the defect could be demonstrated.
Therefore, it seems safe to state that 21 cases are definitely acquired isolated FVII deficiency, whereas 8 cases are probable but not confirmed. Despite the rarity of the event, these observations have great clinical and scientific significance. For example, a careful coagulation study is indicated in all patients with neoplastic conditions. The defect is usually mild to moderate but it may become relevant in case of surgery. Bleeding is also variable and often out of proportion with the entity of the defect.
Since we are dealing with acquired conditions, the contributing effect of a low or borderline platelet count should be kept in mind. Furthermore, the gravity of the condition is well demonstrated by the elevated number of deaths, due in most cases to the underlying malignant or infectious disease. However, bleeding was a contributory cause of death in a few instances. 9,22
The significance of the defect is also highly scientific since the mechanism underlying it is still poorly defined. In the case of amyloidosis-related FX deficiency, absorption of the clotting factor by the amyloid or an antibody-mediated process has been proposed. 3,30 However, a similar mechanism has not been proven for other clotting factors.
The mechanisms underlying an acquired defect could be due, on theoretical grounds, to: (1) decreased synthesis; (2) accelerated consumption or catabolism; (3) neutralization by an antibody; (4) abnormal adsorption by tumor mass; (5) synthesis of abnormal, hypoactive, or labile forms.
Cases with a block in the synthesis have never been suspected or reported. An accelerated consumption has been proposed, particularly in cases where a massive, sudden availability of tissue factor (TF) occurs (increased leakage into surrounding tissue in patients who have undergone extensive chemotherapy, which is known to alter capillary permeability). 22 Another example of increased catabolism or destruction may occur in cases of sepsis due to the proteases secreted by leukocytes. 6 The neutralization by an antibody has been demonstrated in a few instances. 7 The synthesis of an abnormal form characterized by a short half-life or by hypoactivity has never been proposed.
Probably more than one mechanism may act in some patients. For about 50% of cases, the immunological explanation seems the most likely. Unfortunately, the characterization of the antibodies has not been complete and therefore no sure conclusions can be carried out. Altogether, it may be stated that the mechanism underlying isolated FVII deficiency is multiple and still ill defined. This is no surprise if one takes into account that the same is true even for isolated FX deficiency, which has been known to be associated with amyloidosis since about 30 years. 30
The association with myxoma of right atrium is particularly interesting since the condition may cause both lung metastasis, like in the personal case, and pulmonary embolism. 31,32 However, myxomas of the heart involve usually the left atrium which cause, safe for the persistence of a patent foramen ovale, peripheral arterial embolisation. 33,34 In a series of 6 patients of right atrium myxomas studied by the cardiac surgery unit of our University, no case presented a prolonged PT and therefore presumably they all had a normal FVII level. 34 It is worth noting that a right atrium myxoma was removed also from a patient with congenital FVII deficiency 35 and that the potential association of myxomatous tissue with coagulation factors is demonstrated by the immunohistochemical demonstration of the presence of FXIII unit in myxomas. 36,37 The TF content of myxomas is unknown. However, since heart muscle contains high levels of TF, 38 it is plausible that myxomas, which derive from heart muscle, also contain high levels of TF This could explain the occasional association of low levels of FVII in some of these patients. Similar considerations may apply to Wilms’ tumor since kidney is also rich in TF. 38 The large availability of free TF could trap or bind FVII and cause its decrease in plasma. This interpretation is plausible but is limited by the observation that not all myxomas cause this event. 34 Needless to say that the trapping effect could vary from case to case and that minor decreases of FVII might go undetected.
It is important to note also that a decrease of FVII has been maintained to be an early indication of the occurrence of venous occlusive disease (VOD) in patients undergoing stem cells transplantation (STC) in hematological malignancies. 22 FVII, due to its short half-life, could appear decreased earlier than other clotting factors in the development of VOD.
Contrary to what seen for FX, an association with amyloidosis seems rare. Only one such case of the 29 patients showed that relation.
A final consideration is indicated. A decrease in FVII activity seemed to be associated with a poor prognosis. There were 11 fatalities and the poor prognostic sign appeared evident especially for sepsis. This finding is in contrast with what found recently for cases with nonamyloidosis-associated isolated FX deficiency. 39
This study emphasizes the importance of a careful evaluation of a prolonged PT in the management of all patients. The presence of a prolongation of this test in the absence of liver disease, coumarin intake, or malabsorption should always stimulate the interest of the physician to request specific FVII and/or FX essays, according to the circumstances. The finding of a low FVII or a low FX could also suggest some diagnostic clues since FX is low in amyloidosis, whereas FVII is usually normal in that condition. The opposite may be true in other conditions such as atrial myxoma, Wilms’ tumor, and sepsis.
Acquired single clotting factor deficiencies have received little attention in comparison with hereditary forms. The present study together with other studies concerning FX indicate the need of further investigations in this field. 39
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported in part from the “Associazione Emofilia ed altre Coagulopatie delle Tre Venezie.”