
Abstract
Background:
The alterations of the fibrinolytic components in osteoarthritic joint disease and their postsurgical modulation are not clearly understood. Preexisting hemostatic dysfunction may lead to both thrombotic and bleeding events in these patients.
Aim:
To profile fibrinolytic parameters in patients undergoing total joint arthroplasty prior to and on postoperative day 1.
Methods:
A total of 98 total joint arthroplasty patients were included in this study. Blood samples were drawn preoperatively and on postoperative day 1 status posttotal knee or total hip arthroplasty surgery.
Results:
Preoperative PAI-1,
Conclusion:
These results confirm the perturbation in the fibrinolytic system of patients undergoing total joint arthroplasty surgery. Surgical intervention may also enhance the observed changes. The alterations in the fibrinolytic system may lead to the observed hemostatic complications such as bleeding, hematoma formation, or potential need for blood transfusion.
Introduction
It is well established that major lower extremity total joint arthroplasty patients have increased risk of postoperative venous thromboembolism 1,2 and bleeding. 3 The reasons for this hemostatic dysregulation are not fully understood. Some factors have been postulated as the source for this hemostatic imbalance such as the use of tourniquet and increased endogenous fibrinolytic activity. 4 –6 The use of anticoagulant treatment protects patients from potential thrombotic complications; however, the factors contributing to bleeding complications remain to be elucidated. Decreased preoperative hemoglobin levels may reach to around 3 g/dL at postoperative day 3 and necessitate the need for blood transfusions. 3,7 It is well known that blood transfusions have potential complications, such as infectious agent contamination, allergic reactions, hemolytic complications, and transfusion related acute lung injury. 8 –10
Excessive bleeding has been attributed to increased fibrinolytic activity in orthopedic surgery. 4 Drained blood samples after total knee arthroplasty (TKA) have been analyzed and found to have increased biomarkers of fibrinolytic activity. 11 Increased fibrinolytic activity may lead to increased fibrin degradation and thus results in excessive bleeding. Some approaches to reduce the bleeding during orthopedic surgery, such as the use of fibrin sealant and/or tranexamic acid, have been used. 12,13 A clear understanding of the fibrinolytic dysregulation in these patients will help to develop adequate approaches to control bleeding. It has been reported that controlling the blood loss during surgery contributes to shorter hospital stay. 12
The aim of this study is to evaluate the fibrinolytic status of patients undergoing major lower extremity total joint arthroplasty surgery and to evaluate the effect of surgery on the fibrinolytic profile.
Methods
After approval of the institutional review board, consecutive patients were selected from 3 fellowship trained arthroplasty surgeons at this institution. No patients were excluded. Preoperative day 1 and postoperative day 1, blood samples of 98 consecutive arthroplasty patients who underwent TKA (66) or total hip arthroplasty (THA; 32) were obtained as deidentified samples. All patients received warfarin on preoperative day 1, which was continued until postoperative day 30, with a goal international normalized ratio of 2.0 to 2.5. Residual blood samples from routine preoperative and postoperative laboratory draws in tubes containing 3.2% (0.109 mol/L) sodium citrate were used. Samples were centrifuged for preparation of platelet poor plasma at 3000 rpm, at room temperature, for 20 minutes. Laboratories were drawn 1 to 2 weeks preoperatively and on postoperative day 1. Plasma samples were aliquoted to 3 different spaces to avoid repeated thawing and freezing. Samples were stored at −80°C until analysis was completed. Plasma levels of plasminogen activator inhibitor 1 (PAI-1),
The quantitative determination of PAI-1 antigen levels of plasma was measured by a commercially available enzyme-linked immunosorbent assay (ELISA) kit (Asserachrom PAI-1; Diagnostica Stago, France). The quantitative determination of
Citrated plasma samples from 50 (25 males and 25 females) nonsmoking, drug-free, 18- to 35-year-olds were obtained from George King Biomedical (Overland Park, Kansas). These samples served as the control group and analyzed for PAI-1,
Statistical Analysis
GraphPad Prism program version 4, 2003, was used for statistical analysis. Nonparametric tests were used. The Mann-Whitney U test was used to identify significant differences between patients and controls. The Wilcoxon signed rank test was used to determine significant differences between preoperative and postoperative samples in the same patient. Data were summarized by median and interquartile ranges (median [IQR]). The Spearman r test was used to demonstrate correlations between 2 variables. Significance was achieved when P < .05 (2 sided).
Results
Preoperative PAI-1 was significantly higher in the arthroplasty patients compared to healthy controls (HCs; median [IQR]: 49.92 [35.9-71.47] vs 8.9 [2.46-19.19] ng/mL [HC], P < .0001; Mann-Whitney test). Postoperative levels of PAI-1 were increased compared to preoperative values (median [IQR]: 58.24 [40.37-87.29] ng/mL, P = .023; Signed Rank test; Figure 1).
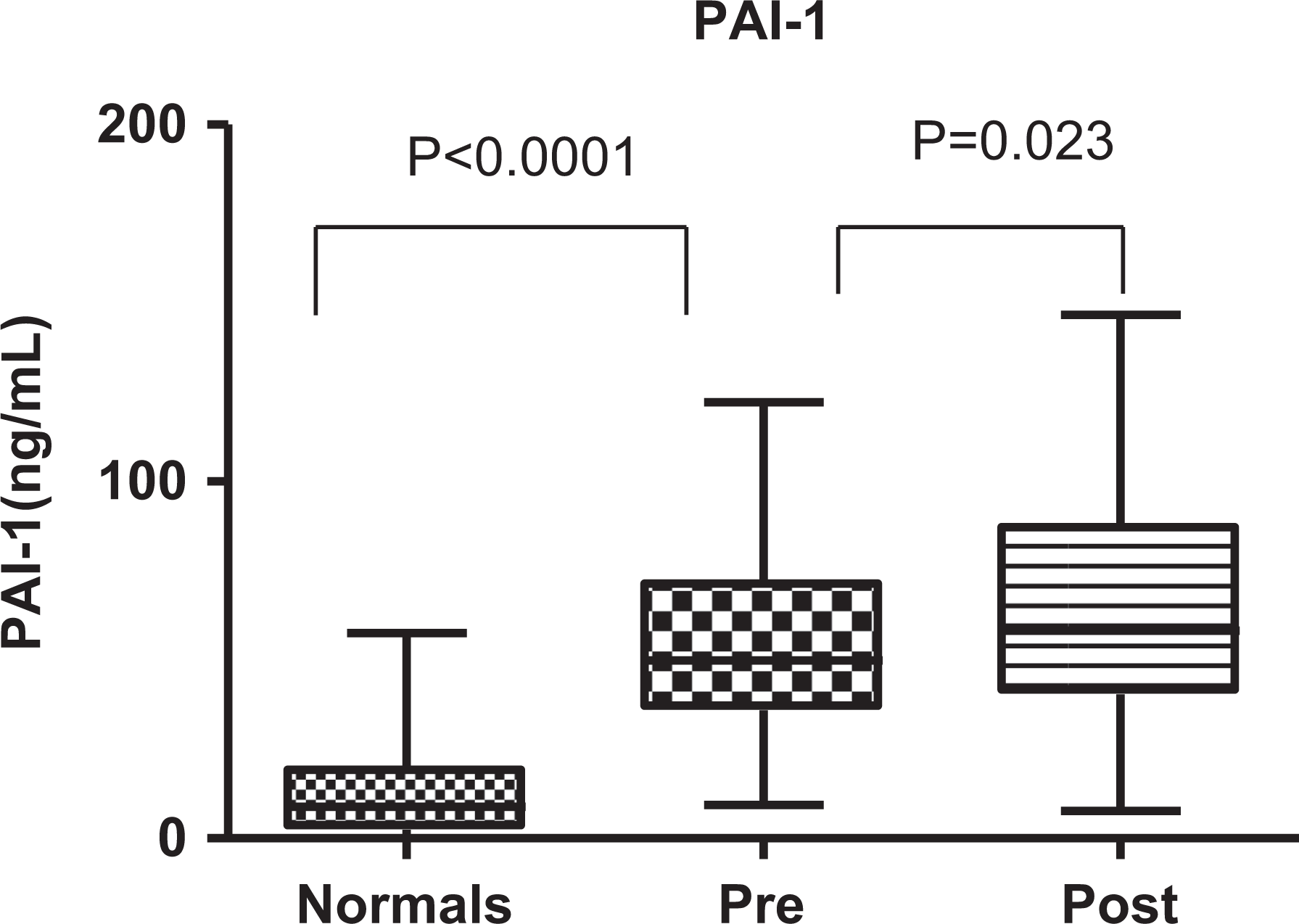
Boxplots demonstrating the plasminogen activator inhibitor 1 (PAI-1) levels in patients pre- and postoperative period compared to healthy controls. Both the pre- and postsurgical plasma samples were significantly different in comparison to the control.
Preoperative
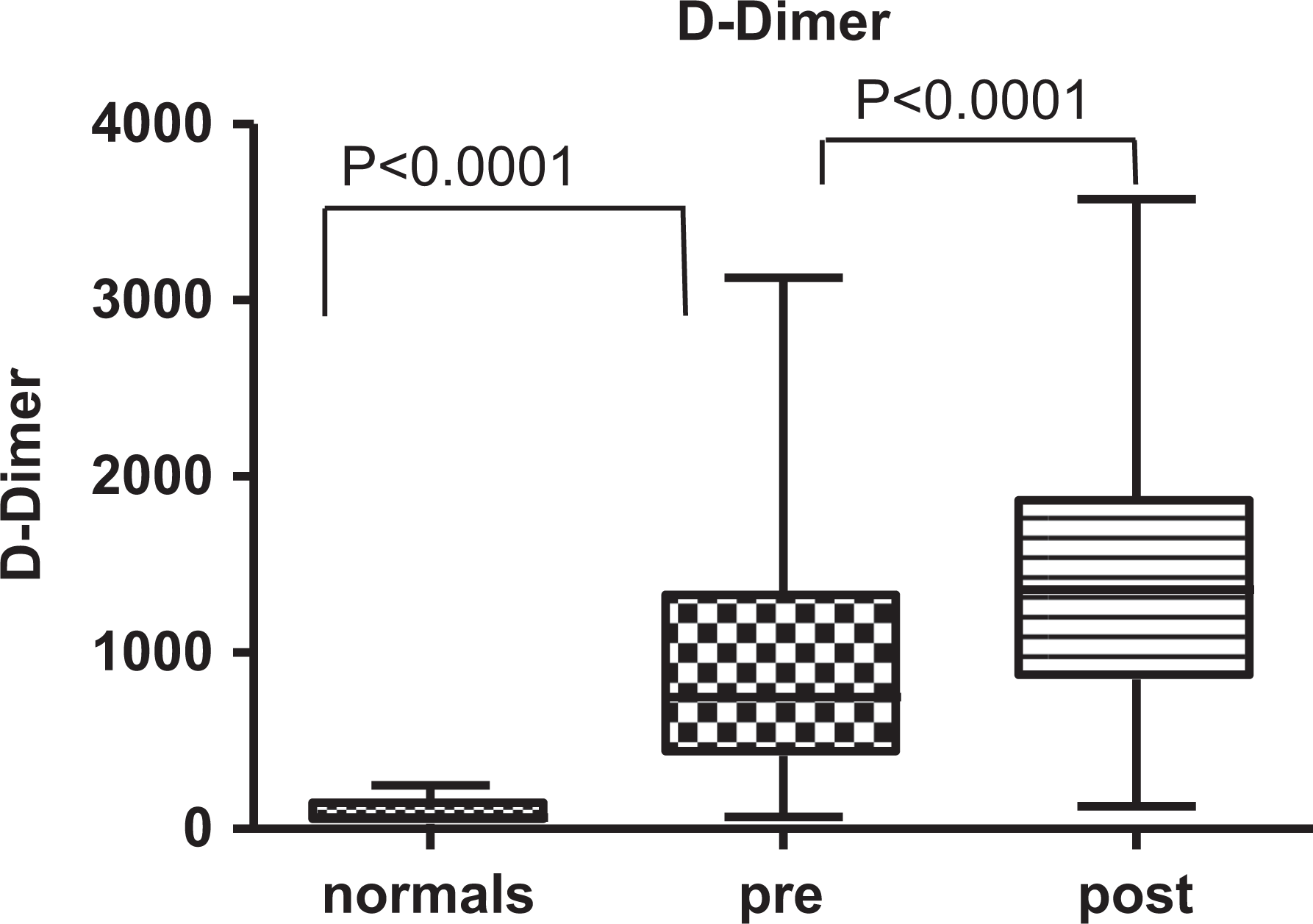
Boxplots demonstrating the
Preoperative tPA was significantly higher in arthroplasty patients compared to HCs (median [IQR]: 8.55 [6.9-10.1] vs 3.83 [3.015-5.11] ng/mL [HC], P < .0001; Mann-Whitney test). Postoperative changes in tPA were not significant (median [IQR]: 7.7 [6.1-9.9] ng/mL, P = .157; Wilcoxon signed rank test; Figure 3).
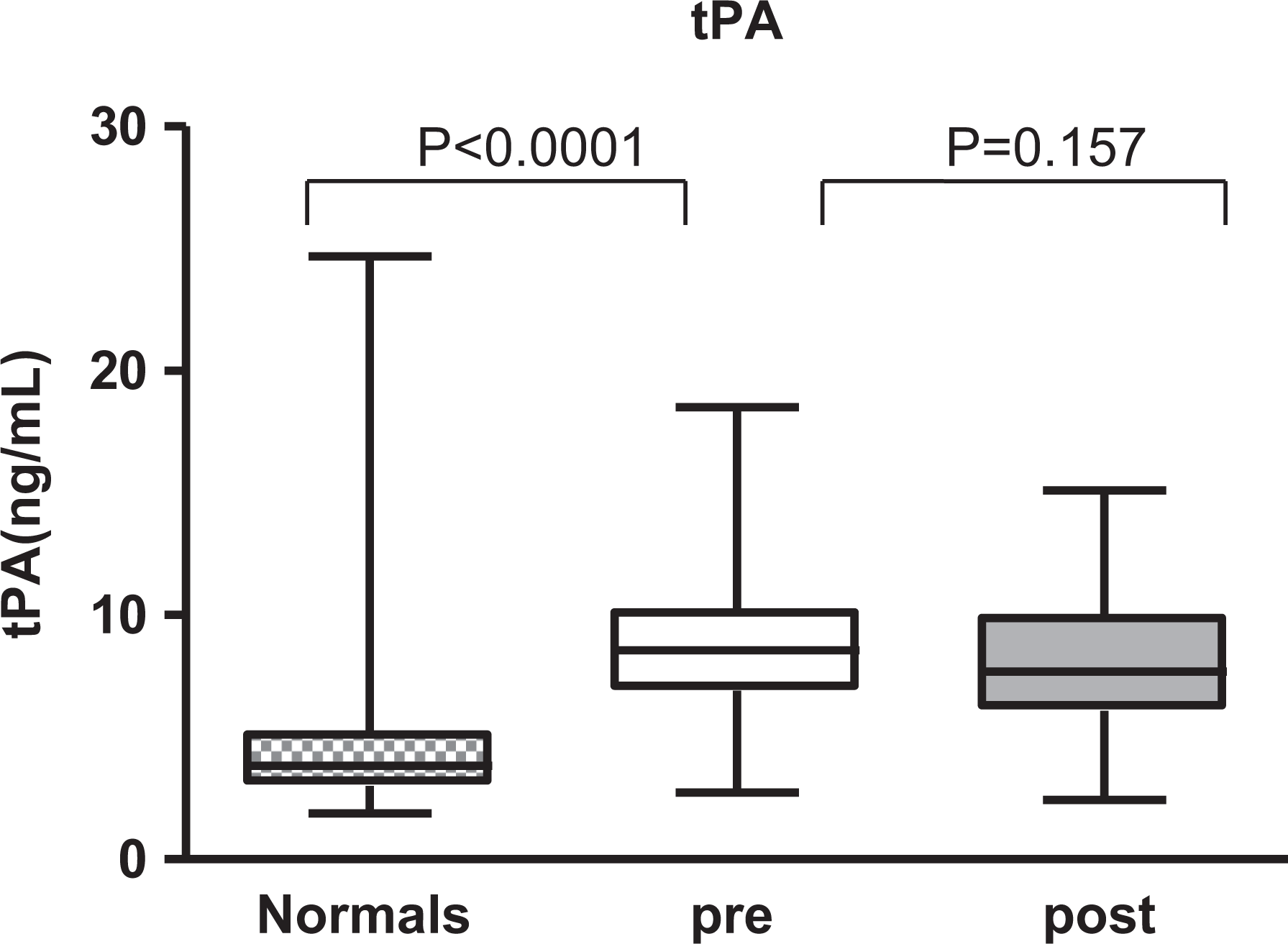
Boxplots demonstrating the tissue plasminogen activator (tPA) levels in patients pre- and postoperative period compared to healthy controls. Presurgical plasma samples was significantly different in comparison to the control, whereas postsurgical samples did not exhibit any differences compared to presurgical value.
Preoperative antiplasmin levels were lower in arthroplasty patients than in HCs (median [IQR]: 73.82 [62.87-87.37]% vs 79.63 [74.52-84.13]% [HC], P = .045; Mann-Whitney test). Postoperative antiplasmin values were lower than preoperative levels (median [IQR]: 69.13 [55.82-81.95]%, P = .024; Wilcoxon signed rank test; Figure 4).
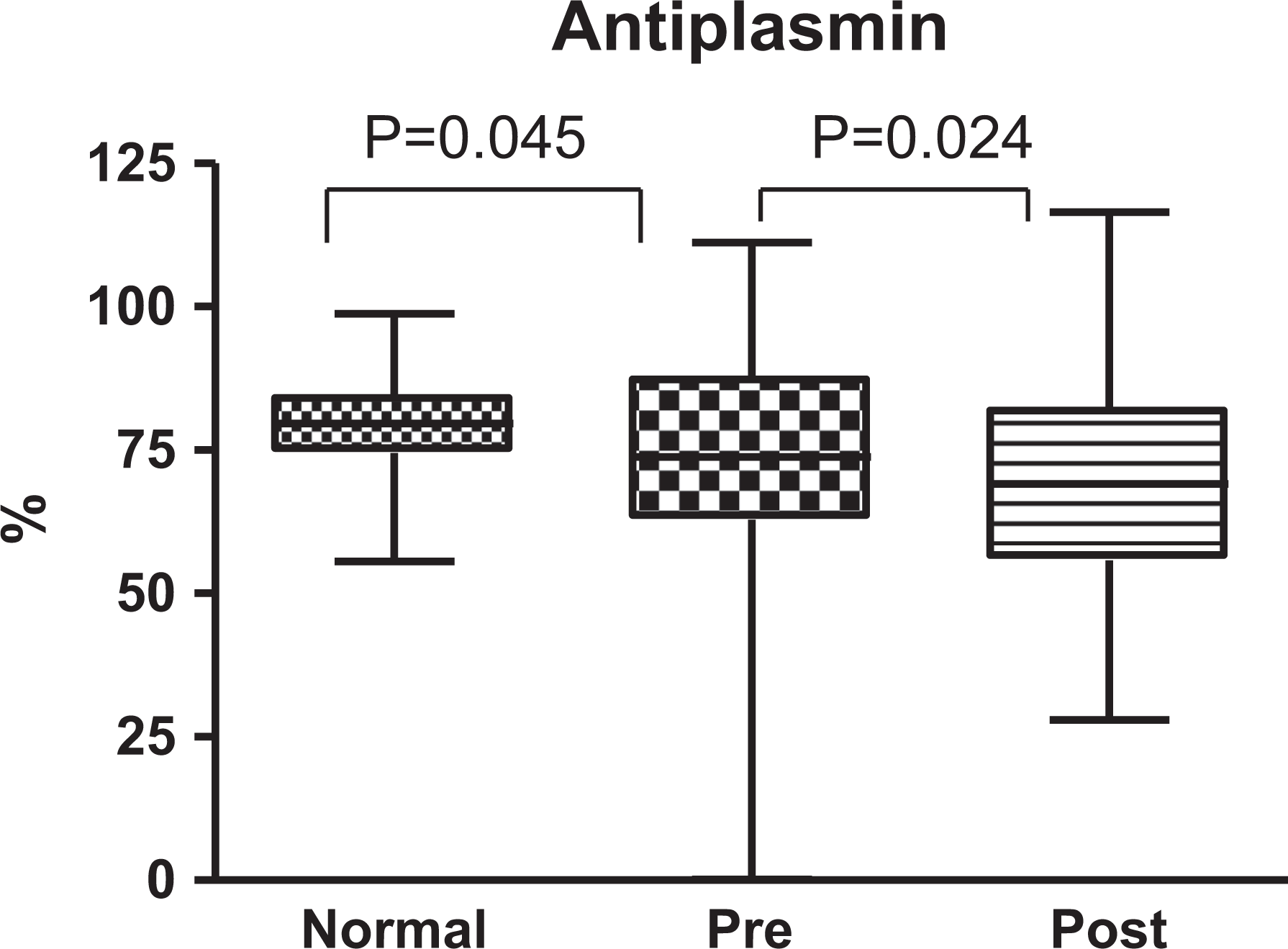
Boxplots demonstrating the antiplasmin activity in patients pre- and postoperative period compared to healthy controls. Both the pre- and postsurgical plasma samples were significantly different in comparison to the control.
There was no correlation between preoperative PAI-1 and
Pre- and postoperative percentage changes (PCs) of each individual were also calculated for PAI-1,
For PCs, Spearman correlation analysis revealed that there was a significant correlation between
Discussion
In the present study, arthroplasty patients showed increased fibrinolytic activity in the preoperative period. Their preoperative
In the postoperative period, arthroplasty patients also exhibited increased fibrinolytic activity compared to their preoperative values. Their
Previous studies have shown that there is increased thrombogenic and fibrinolytic activity during and immediately TKA and THA.
5,6,16
Blood loss has also been found to correlate with fibrinolytic markers rather than thrombogenic markers.
4
Tourniquet use has also been shown to be a factor in mediating the generation of such biomarkers as prothrombin fragment 1.2 (F1.2), plasmin–antiplasmin (PAP), and
Consistent with our studies, other investigators have also reported hemostatic dysregulation in patient who underwent TKA and THA. 18 Higher levels of factor VIIa, factor Xa (FXa)-antithrombin, F1.2, and C-reactive protein were reported in 306 patients undergoing elective TKA or THA compared to controls, while the levels of thrombin–antithrombin, tissue factor pathway inhibitor (TFPI), and FXa-TFPI were similar. The F1.2 was correlated with FXa-antithrombin in these patients. The CRP was correlated with F1.2 and soluble fibrin but not with FXa-TFPI.
Since the cumulative analysis may not represent the variations observed in each of the individual patients, PC of each patient for each fibrinolytic parameter was also calculated. This analysis showed a positive correlation between PAI-1 and
According to our results, these arthroplasty patients have preexisting increased fibrinolytic activity, which is exacerbated by surgery. This increased fibrinolytic activity represents an additional risk to this subset of patients. Increased preoperative
In this study, we did not find any significant gender-based differences in the fibrinolytic parameters among male and female patients in both the pre- and postoperative samples. One of the limitations of this study is that the controls are not age matched. The arthroplasty patient population is older, and it is difficult to find a group of older patients with no comorbidities that could alter the fibrinolytic profile. If age-matched controls were used and no increase was found in
In conclusion, these studies validate the hypothesis that the preexisting perturbation in the fibrinolytic system in patients undergoing total joint arthroplasty surgery contribute to hemostatic imbalance. The observed increase in the fibrinolytic activity can be attributed to increased thrombogenesis in these patients. Most of these patients may have age-related alterations in the hemostatic system favoring hypercoagulable state, an associated vascular complications. This preoperative reactive fibrinolytic activity may be further augmented by surgical intervention during the TKA and THA. Thus fibrinolytic dysregulation in patients undergoing joint arthroplasty may contribute significantly to the potential hemostatic abnormalities in this group.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.