
Abstract
Bone involvement is a frequent cause of acute morbidity in sickle cell disease (SCD). Tartrate-resistant acid phosphatase 5b (TRACP 5b), a bone resorption marker, is produced specifically by activated osteoclasts. We assessed bone mineral density (BMD) in 30 young patients with SCD and 17 asymptomatic patients with sickle cell trait (SCT) compared with 32 healthy controls and determined TRACP 5b levels in relation to vascular complications. Serum ferritin, alkaline phosphatase (ALP), and TRACP 5b were measured. Echocardiography was performed with assessment of BMD using dual energy X-ray absorptiometry (DXA). The BMD was decreased in patients with SCD compared with SCT and controls (P = .005), with no significant difference between the latter 2 groups. Patients with SCD had higher incidence of bone complications than SCT group and controls (P = .03). The SCD group with abnormal DXA scan had higher ferritin and ALP than normal BMD. Serum TRACP 5b was significantly higher in patients with SCD than SCT and controls (P = .003). The TRACP 5b levels were associated with severe vaso-occlusive crisis (P = .022). Patients treated with hydroxyurea and those on chelation therapy had lower TRACP 5b levels than untreated patients. The TRACP 5b level was positively correlated with lactate dehydrogenase, while there was no relation with ferritin, ALP, or BMD. We suggest that bone complications frequently occur in SCD as reflected by low BMD and high ALP and TRACP 5b. Hemolysis and iron overload may be involved in the occurrence of these complications. The lack of correlation between abnormal DXA scan and high TRACP 5b suggests that bone disease in SCD is multifactorial.
Introduction
Sickle cell disease (SCD) is a multisystem disease, associated with episodes of acute illness and progressive organ damage, and is one of the most common severe monogenic disorders worldwide. 1 Sickle cell trait (SCT) usually is not regarded as a disease state because it has complications that are either uncommon or mild. Nevertheless, under unusual circumstances, serious morbidity or mortality can result from complications related to polymerization of deoxyhemoglobin S. 2 Pathologic processes that cause hypoxia, acidosis, dehydration, hyperosmolality, and hypothermia can transform silent SCT into a syndrome resembling SCD with vaso-occlusion. 2,3
Bone involvement is a frequent cause of acute morbidity in sickle cell anemia (SCA) and some of its variant hemoglobinopathies. 4 It ranges from acute manifestations, such as painful vaso-occlusive crisis or osteomyelitis, to more chronic and debilitating complications, such as osteonecrosis, osteoporosis and osteopenia, impaired growth, and chronic infections. Although these bone complications may not contribute directly to mortality, however, they are the major source of morbidity and highly impact patients’ quality of life. 5
Published studies suggest that children with SCD often have undiagnosed osteopenia or osteoporosis. 6 –8 The causes of bone mass density abnormalities in patients with SCD are probably multifactorial. Several factors, including abnormally low body mass index (BMI), reduced hemoglobin levels, increased ferritin levels, vitamin D deficiencies, and low plasma zinc or sex steroid levels, have been previously correlated with reduced bone mineral density (BMD) in adult patients with SCD. 6 –10
Tartrate-resistant acid phosphatase (TRACP) type 5 is a metalloprotein enzyme with molecular weight of approximately 35 kD. It belongs to the acid phosphatases and is produced by bone-resorbing osteoclasts, inflammatory macrophages, and dendritic cells. Tartrate-resistant acid phosphatase 5b is the bone resorption marker that is produced specifically by activated osteoclasts. 11,12 Normal bone metabolism requires TRACP 5b expression. Adults with SCD have increased osteoclast activity and high TRACP 5b levels due to a potential role of inflammation rather than increased iron stores. Higher osteoclast activity as reflected in TRACP 5b levels was correlated with higher tricuspid regurgitation velocity. There may be common pathways underlying elevated pulmonary artery pressure and increased osteoclast activity in SCD. 13
Therefore, the aim of this study was to assess BMD in children and adolescents with SCD and asymptomatic patients with SCT, and to determine the levels of TRACP 5b and its possible relation with markers of hemolysis, iron overload, and vascular complications.
Materials and Methods
Study Population
This cross sectional case–control study included 30 (18 males and 12 females) patients with SCD recruited from the regular attendants of the Pediatric Hematology Clinic, Pediatric Hospital, Ain Shams University and 17 (10 males and 7 females) asymptomatic patients with SCT who were the siblings of patients with SCD. Thirty two age- and sex-matched healthy participants were enrolled as a control group (16 males and 16 females). The mean age of patients with SCD was 10.7 ± 3.9 years (range: 4-17.2 years) while that of SCT was 10.2 ± 3.0 years (range: 4.9-13.7 years), and the mean age of controls was 11.8 ± 3.2 years (range: 5.8-17.4 years).
An informed consent was obtained from the guardian of each patient or control before participation. The procedures applied in this study were approved by the Ethical Committee of Human Experimentation of Ain Shams University and are in accordance with the Helsinki Declaration of 1975.
The patients included were subjected to detailed medical history and thorough clinical examination with special emphasis on disease duration, anthropometric measures, evidence of renal, hepatic or cardiac disease, frequency of sickling crisis, and history of splenectomy (for patients with HbSβ-thalassemia). All of the patients with SCD were transfused. The transfusion received was calculated as the transfusion index: volume of transfused packed red cells in ml per kg body weight per year (expressed as the mean value of the last 3 years). Patients with SCD included 17 patients with SCA and 13 patients with sickle βº thalassemia, and all were at steady state at the time of sample collection. Twenty patients (66.7%) with SCD received hydroxyurea (Bristol-Meyers-Squibb, New York) as an oral daily dose ranging from 15 to 25 mg/kg/d while 20 (60%) patients received deferoxamine therapy (Desferal, DFO; Novartis Pharma AG, Basel, Switzerland) subcutaneously in a dose that ranged from 30 to -40 mg/kg/d 5 days/week.
Sample Collection
Peripheral blood samples were collected on potassium-EDTA (1.2 mg/mL) for complete blood count (CBC) and hemoglobin analysis. For chemical analysis and enzyme-linked immunosorbent assay (ELISA), clotted samples were obtained and serum was separated by centrifugation for 15 min at 1000 × g, and then stored at −80°C till subsequent use in ELISA.
Laboratory Assessment
Laboratory investigations included CBC using Sysmex XT-1800i (Sysmex, Kobe, Japan), examination of Leishman-stained smears for differential white blood cell count, hemoglobin analysis by high-performance liquid chromatography (HPLC) using D-10 (BioRad, Marnes La Coquette, France), liver and kidney function tests, markers of hemolysis (lactate dehydrogenase (LDH) and indirect bilirubin), calcium, phosphorus, alkaline phosphatase (ALP), and high-sensitivity C-reactive protein (CRP) as well as serum ferritin on Cobas Integra 800 (Roche Diagnostics, Mannheim, Germany). Patients with any clinical evidence of infection at time of the study or 1 month prior to it or those with CRP >10 mg/L were excluded. Serum ferritin level was measured at the start of the study with calculation of the mean value of the last year prior to the study in order to know the ferritin trend. The concentration of TRACP 5b in serum was measured by an ELISA format immunocapture enzyme assay kit (Cat No. MBS162352, My Biosource Corporation, San Diego, California).
Radiological Investigations
All studied patients were clinically asymptomatic for pulmonary hypertension and cardiovascular abnormalities. Screening for pulmonary hypertension and cardiovascular abnormalities was performed by the noninvasive echocardiography with different modalities (Doppler, 2-dimensional imaging, and M-mode) using Vivid E9 (GE Healthcare, Norway) to evaluate left ventricular function, pulmonary artery pressure, and tricuspid regurgitant jet velocity (TRV).
Measurement of BMD was performed by dual energy X-ray absorptiometry (DXA) using GE Lunar DPX Pro, Lunar Radiation Corp. (Madison, Wisconsin). The BMD assessment was carried on the lumbar spine L1-4, which is highly active metabolically and at the neck of the femur. Data were automatically analyzed by special software for analyzing the densities of the examined parts and were expressed in g/cm2 and as a z score value of patients compared with an age- and sex-matched normal reference population. Bone mass deficit was calculated as percentage, approximate standard deviations (z score) above, or below age-matched normal means. Osteopenia was defined as BMD z score < −1.0, while low bone density for chronological age was diagnosed if BMD z score was less than −2.0 and if there was no history of fractures. Osteoporosis was defined if BMD z score was less than −2.0 and if there was clinically significant fracture history (1 long bone fracture of the lower extremity, vertebral compression fracture, and 2 or more long-bone fractures of the upper extremities). 14,15
Diagnostic Criteria
The definition of SCD was based on complete blood picture, reticulocyte count, markers of hemolysis, as well as hemoglobin analysis using HPLC, and confirmed by genotyping based on identification of β-globin gene mutations by polymerase chain reaction implications of the DNA and subsequent reverse hybridization to immobilized allele-specific biotinylated oligonucleotide probes covering the most common Mediterranean mutations. 16 A painful crisis was defined as the occurrence of pain in the extremities, back, abdomen, chest, or head that lasted at least 2 h, led to a clinic visit, and could not be explained except by SCD, 17 while steady state was defined as a period without pain or painful crisis for at least 4 weeks. 18 The frequency of sickling crisis in the previous year was divided into mild (defined as 2 or less episodes requiring medical visits) or severe (defined as 3 or more episodes requiring medical visits). 19 The diagnosis of acute chest syndrome was defined as a new pulmonary infiltrate on chest X-ray and ≥2 of the following: chest, upper abdominal, or rib pain; dyspnea; fever; tachypnea; grunting; nasal flaring; or retractions. 20 A TRV ≥2.5 m/s was used as a proxy for patients at risk for pulmonary hypertension. 21,22
Statistical Analysis
Analysis of data was done using Statistical Program for Social Science version 15 (SPSS Inc., Chicago, Illinois). Quantitative variables were described in the form of mean and standard deviation. Qualitative variables were described as number and percentage. In order to compare quantitative parametric variables between the 3 studied groups, analysis of variance (ANOVA) test with post hoc test was used, while Student t test was applied for comparison between 2 groups. Qualitative variables were compared using χ2 test or Fischer exact test when frequencies were below 5. Correlation studies were done using Pearson’s correlation coefficient. A P value <.05 was considered significant or P value <.001 was considered highly significant in all analyses.
Results
All the 30 studied patients with SCD or 17 asymptomatic patients with SCT had normal ejection fraction (>55%) while 9 (30%) patients with SCD had elevated TRV (≥2.5 m/s) denoting pulmonary hypertension risk. The clinical and radiological data of the studied groups are listed in Table 1. Upon comparison between the 3 studied groups, a significant difference was found as regards BMI SDS. The BMI was significantly lower among SCD group compared with both controls (P = .001) and SCT group (P = .002) while no significant difference was found between the latter 2 groups (P = .214). Bone fractures and avascular necrosis were found in 13.3% and 10% of patients with SCD, respectively. The incidence of abnormal whole body BMD (WB-BMD) results was 53.3%, while that of lumbar spine BMD (LS-BMD) was 60%. Using lumbar spine DXA, patients with SCD showed higher incidence of bone complications in the form of low bone density (40.7%) and osteoporosis (7.4%) than SCT group (12.5% and 0.0%, respectively) and controls (4.8% and 0.0%, respectively); P = .03 (Table 1).
Clinical Data and Bone Mineral Density Status Among Patients With Sickle Cell Disease or Sickle Cell Trail Compared With Healthy Controls.a
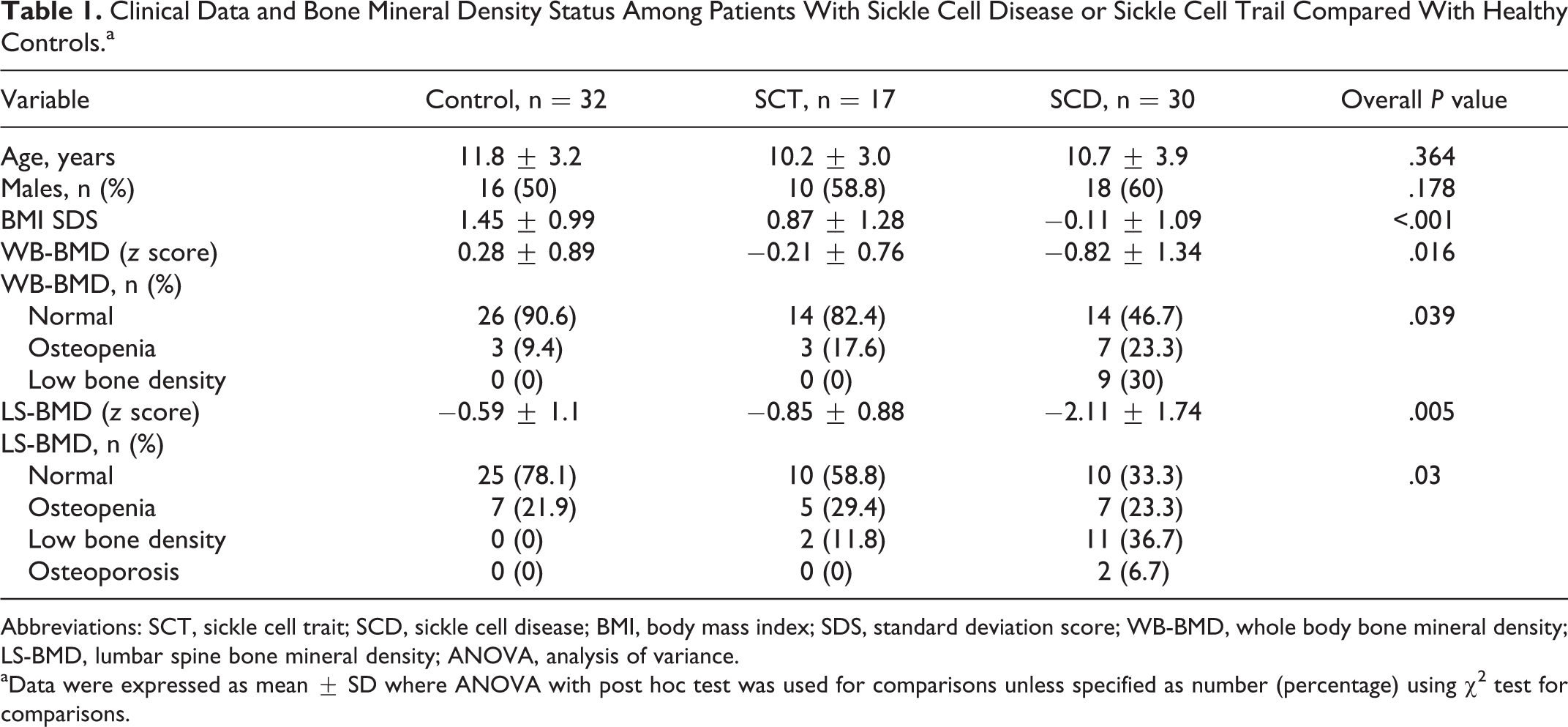
Abbreviations: SCT, sickle cell trait; SCD, sickle cell disease; BMI, body mass index; SDS, standard deviation score; WB-BMD, whole body bone mineral density; LS-BMD, lumbar spine bone mineral density; ANOVA, analysis of variance.
aData were expressed as mean ± SD where ANOVA with post hoc test was used for comparisons unless specified as number (percentage) using χ2 test for comparisons.
Patients with SCD and abnormal DXA scan (osteopenia/low bone density) had higher mean age (13.3 ± 2.8 years vs 9.3 ± 3.6 years; P = .003) with significantly lower BMI (P < .001) and higher disease duration (P = .016), platelets count (P = .007), serum ferritin (P < .001), and ALP (P = .025) compared with those having normal BMD (Table 2). The incidence of splenectomy (36.4% vs 0.0%; P = .005) and endocrine abnormalities (45.5% versus 5.3%; P = .008) was higher among SCD group with abnormal BMD (Figure 1). Endocrine disorders among the studied patients were in the form of growth failure (decreased height, weight, and BMI), delayed puberty, and low BMD.
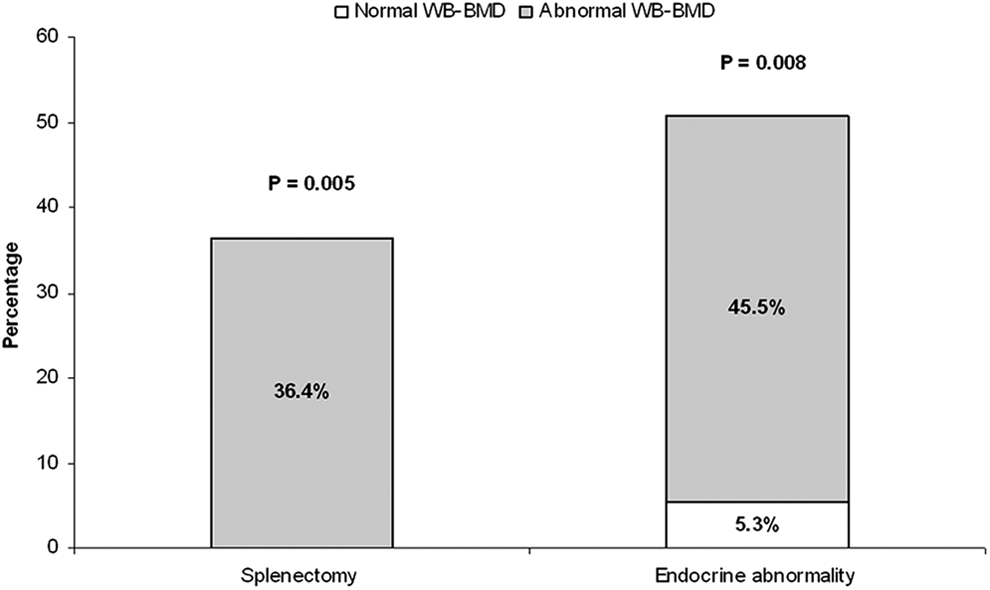
Frequency of splenectomy and endocrine abnormalities among patients having sickle cell disease (SCD) with normal and abnormal bone mineral density.
Clinical and Laboratory Characteristics of Patients With Sickle Cell Disease Having Normal and Abnormal Whole Body Bone Mineral Density (BMD) Status.
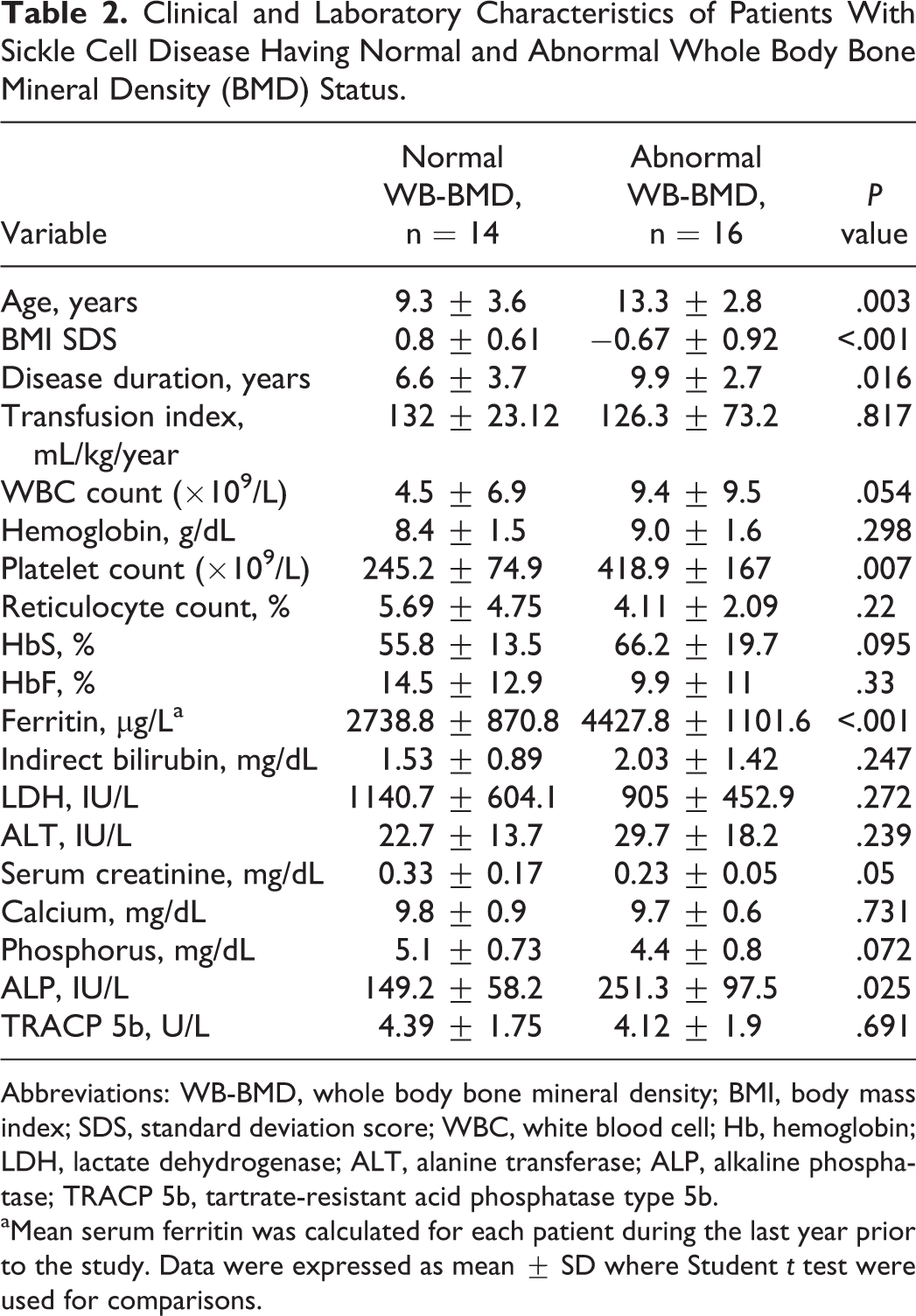
Abbreviations: WB-BMD, whole body bone mineral density; BMI, body mass index; SDS, standard deviation score; WBC, white blood cell; Hb, hemoglobin; LDH, lactate dehydrogenase; ALT, alanine transferase; ALP, alkaline phosphatase; TRACP 5b, tartrate-resistant acid phosphatase type 5b.
aMean serum ferritin was calculated for each patient during the last year prior to the study. Data were expressed as mean ± SD where Student t test were used for comparisons.
Serum TRACP 5b was significantly higher in patients with SCD (4.10
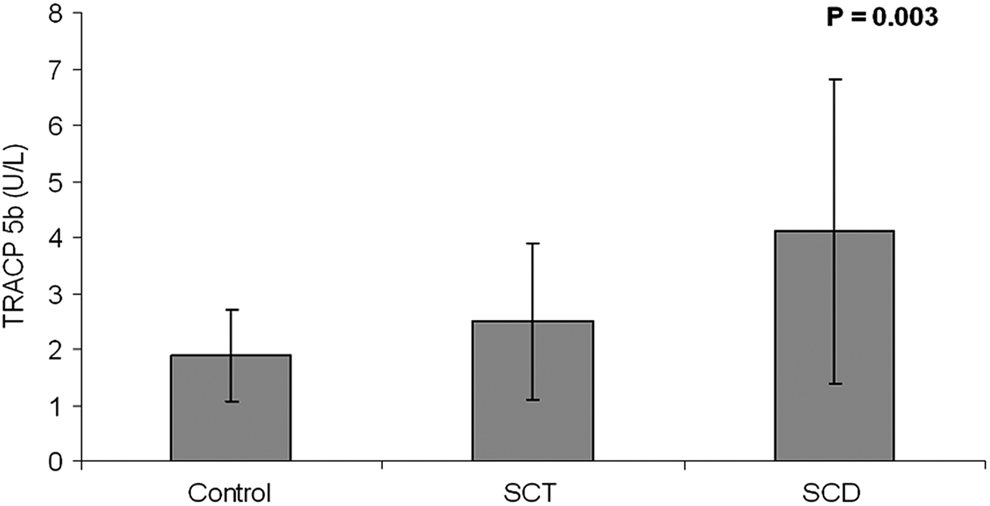
Tartrate-resistant acid phosphatase 5b (TRACP 5b) levels among patients with sickle cell disease or sickle cell trait compared with healthy controls.
Serum TRACP 5b Levels Among Patients with Sickle Cell Disease (SCD) in Relation to Some Disease Complications and Therapy.
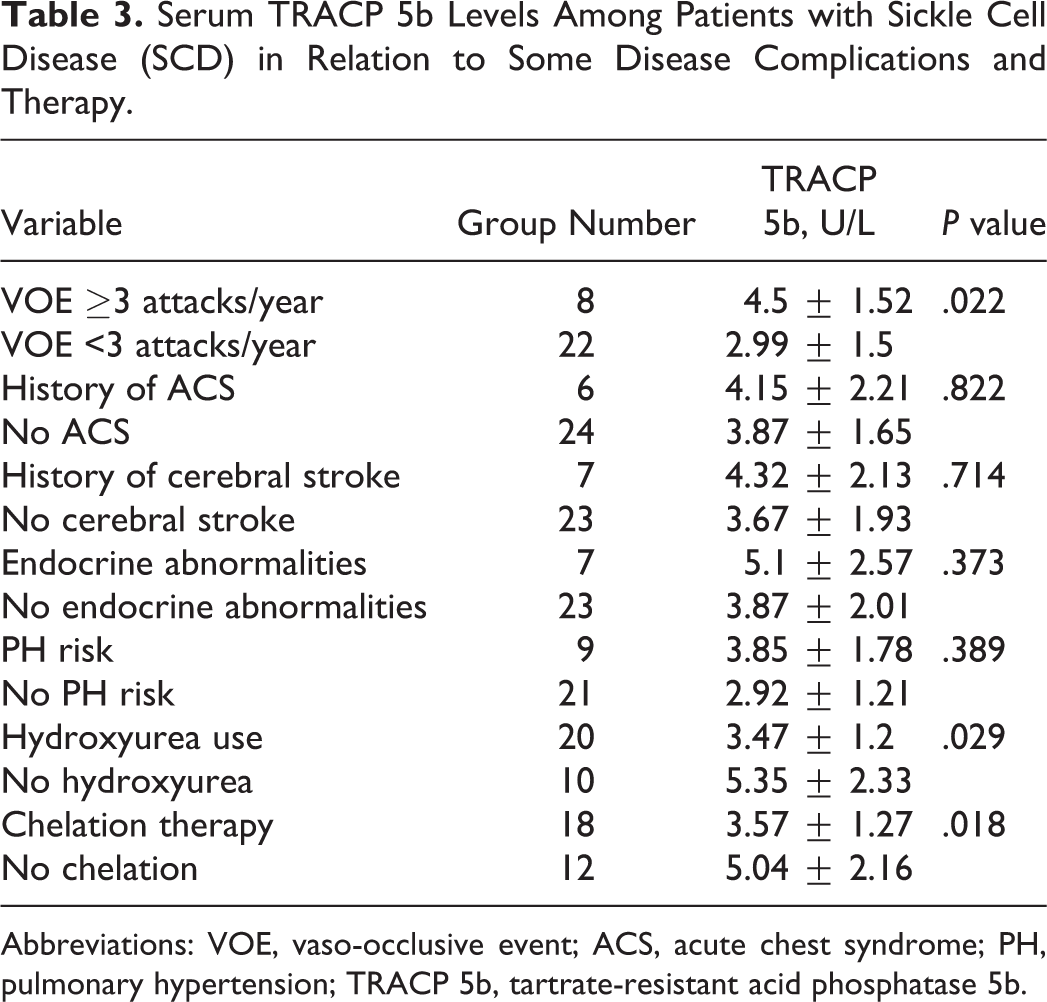
Abbreviations: VOE, vaso-occlusive event; ACS, acute chest syndrome; PH, pulmonary hypertension; TRACP 5b, tartrate-resistant acid phosphatase 5b.
No significant difference was found between patients with SCA or those with sickle-thalassemia as regards any of the studied markers of osteoclastic activity (Table 4). The TRACP 5b level was positively correlated with LDH (r = .563, P = .045) while there was no relation with other variables including transfusion index, serum ferritin, ALP, TRV, or BMD. Both WB-BMD and LS-BMD were positively correlated (r = .919, P < .001). The WB-BMD and LS-BMD were positively correlated with BMI (r = .624, P < .001) while negatively correlated with platelet count (r = −0.686, P < .001) and ALP (r = −.402, P < .001).
The Studied Markers of Osteoclastic Activity in Relation to Sickle Cell Disease (SCD) Genotypes.a
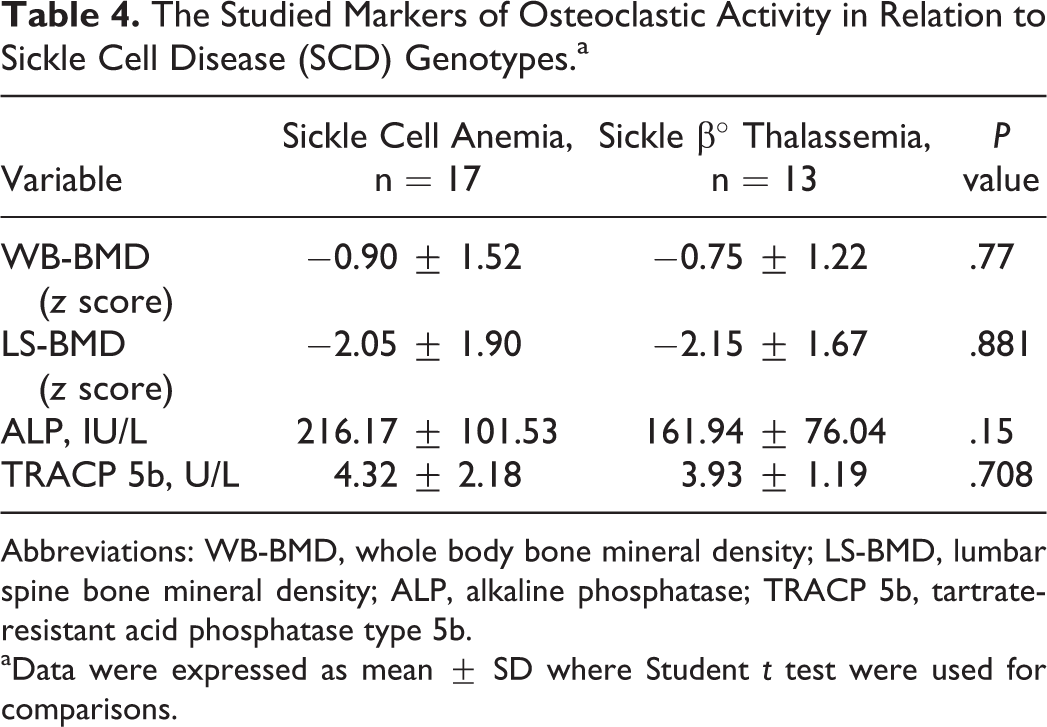
Abbreviations: WB-BMD, whole body bone mineral density; LS-BMD, lumbar spine bone mineral density; ALP, alkaline phosphatase; TRACP 5b, tartrate-resistant acid phosphatase type 5b.
aData were expressed as mean ± SD where Student t test were used for comparisons.
Discussion
Complications of SCD are numerous and affect every organ in the body. 23 Osteoporosis may be one of the major public health problems in patients with SCD, particularly if the onset takes place at an early age. 24 DXA is a widely available, precise, and safe method for measuring BMD and has now become the preferred clinical instrument to assess bone mass in children. 25 The TRACP 5b is a bone resorption marker used for prediction of high bone turnover. 11,12,26
In this study, patients with SCD had lower BMI as compared to both SCT and control groups. Children with SCD are known to have normal weight and length at birth, and then around 6 months of age, their growth patterns begin to diverge from the norm. The growth deficits experienced by these children remain a problem with clinical significance and diverse consequences. 27 Poor growth in children with SCD is linked to hematological factors, endocrine dysfunction, metabolic derangement, specific nutrient deficiencies, chronic inflammation, and increased total energy expenditure. 28 –31
In the current study, patients with SCD had significantly lower BMD as evidenced on both whole body and lumbar spine DXA when compared with SCT and control groups. The WB-BMD z scores were positively correlated with LS-BMD z scores among patients with SCD. Decreased BMD has long been described in adult patients with SCD; however, BMD has not been widely studied in children with SCD. Several pathogenic factors are known to contribute to the etiology of low BMD in patients with SCD, including reduced physical activity, 32 decreased circulating growth hormone (GH), 33 poor dietary intake of bone-forming nutrients, 34,35 abnormally low BMI, reduced hemoglobin levels, increased serum ferritin levels, vitamin D deficiencies, and low plasma zinc or sex steroid levels. 6 –10 Moreover, decreased BMD has been reported in other forms of chronic hemolytic anemia like thalassemia and has been linked to many factors as follows: delayed sexual maturation, deficiency of GH, or insulin growth factor I, presence of diabetes, parathyroid gland dysfunction, marrow expansion, and direct iron toxicity. 36
In this study, we found a higher incidence of splenectomy among patients with low WB-BMD. Although the prominent feature of SCD is autosplenectomy, a possible explanation to patients who underwent splenectomy is the presence of sickle thalassemia with hypersplenism. 37 It is speculated that the loss of the spleen increases the circulation of platelet mediators and senescent erythrocytes that result in platelet activation, and possibly stimulates the increase in the intravascular hemolysis rate. 38 Increased intravascular hemolysis has been linked to decreased BMD. 39 Gurevitch and Slavin 40 suggested that overexertion of the hematopoietic system resulting from constant excessive need for blood cell production plays an important role in the etiology of osteoporosis. However, our results showed no significant relationship between BMD and markers of hemolysis including reticulocytic count, indirect bilirubin, and LDH.
Interestingly, we found a negative correlation between BMD and platelet count. Sickle cell disease is a chronic inflammatory disease, 41 and individuals with SCD demonstrate increased levels of numerous cytokines and pro-inflammatory proteins in their circulation including interleukin (IL) 8, tumor necrosis factor α, CRP, IL-6, and soluble adhesion molecules. 41 –44 Multiple cell types contribute to the production of inflammatory mediators, including activated endothelial cells, leucocytes, and platelets. Several platelet-derived cytokines may contribute to vascular inflammation in SCD. 45 A relationship between inflammation and bone disease has been established. An inflammatory disease can increase bone resorption, decrease bone formation but, most commonly, impact both of these processes resulting in an uncoupling of bone formation from resorption in favor of excess resorption. 46 Even low level subclinical inflammation has been reported to affect bone remodeling and increase fracture risk. 47
Recent research data in SCD have shown a direct correlation between bone turnover markers (TRACP 5b) and inflammatory mediators (IL-8 and chemokine C-C motif ligand 5 [CCL5]), suggesting a potential role of inflammation in stimulating osteoclast activity and hence increasing the risk of osteoporosis among patients with SCD. 13 In agreement with our results, Brinker et al 48 found low BMD values in the proximal femora and lumbar spines of 25 black children and adolescents with SCA, and these differences in the LS-BMD were significant for both girls and boys. When normal black individuals were compared with the general population, the girls with SCA exhibited significantly lower LS-BMD, and the boys with SCA exhibited significantly lower BMD in the femoral neck and Ward’s triangle. They reported no consistent or significant correlations between BMD data and the patients’ hematologic indices.
Among the published data, the highest prevalence of decreased BMD among population (79.6%) with SCD was reported by Sarrai et al 7 with a predilection for the lumbar spine. Abnormal BMD was associated with lower BMI, lower hemoglobin level, and higher serum ferritin. Patients with low BMD were more likely to be SCA, sickle hemoglobin C disease, sickle β° thalassemia than sickle β+ thalassemia. Buison et al 49 reported significant deficits in WB-BMD that persist despite adjustment for poor growth and decreased lean mass in children with SCA. Moreover, the high prevalence of low BMD among SCA children has been reported with no significant correlation between reduced BMD and gender, calcium intake, chronic transfusions, growth delay, or serum ferritin level. 24
Bone turnover markers have advanced significantly such that they are now used to assist with the diagnosis and monitoring of osteoporosis therapy in adults. However, some researchers have suggested that the usefulness of these markers in children is not in the clinical diagnosis of low bone mass but rather in the longitudinal assessment of interventions on bone and growth, 50 and that they appear to reflect changes in growth and pubertal status rather than changes in bone indices. 51
Few studies have assessed bone turnover in patients with SCA and explored its relation to DXA, 24 ultrasound, 52 or protein metabolism. 53 Some authors 53,54 but not all 24,52 reported elevations in markers of bone formation (bone ALP [bALP] and procollagen type-I C-terminal peptide [PICP]) in SCA compared with controls. Reports of markers of bone resorption in pediatric patients with SCA are equally divided: one reported increased urinary pyridinium 50 and the other reported decreased N-terminal telopeptide of collagen type-I (NTX) in serum compared to controls. 52
In addition, Voskaridou et al 55 assessed the prevalence of osteopenia/osteoporosis and osteosclerosis among patients with HbS/β-thalassemia, and they reported higher levels of serum osteoprotegrin, bALP, and PICP in patients with HbS/β-thalassemia as compared with controls, independent of their BMD status. Similar studies assessing BMD and its relation to bone turnover markers have been done in patients with thalassemia, and found reduced BMD among children with β-thalassemia, with significantly higher levels of urinary deoxypyridinoline and lower serum osteocalcin (OC) and PICP in comparison to healthy controls. 56
In the present study, serum TRACP 5b levels were significantly higher in patients with SCD than SCT and control groups. This difference in serum TRACP 5b was postulated to be due to higher osteoclastic activity and resultant lower BMD (as BMD was found to be significantly lower in patients with SCD compared with both SCT and control groups). However, we could not find a significant relationship between BMD and serum TRACP 5b levels.
Very few studies have assessed serum TRACP levels in population with SCD. Nouraie et al. 13 reported increased serum TRACP in adults with SCD in comparison with controls which was not related to serum ferritin concentration but directly correlated with the inflammatory markers IL-8 and CCL5 as well as TRV (as a risk factor for pulmonary hypertension). This may support a potential role of inflammation, rather than increased iron stores, in stimulating osteoclast activity in patients with SCD. The authors suggested the possibility of a common pathway in the pathogenesis of pulmonary hypertension and bone complications of SCD.
The 2 main pathophysiological processes in the crisis state are ischemia and inflammatory process. 23 Increase in markers of oxidative stress in sickle crisis leads to increase in inflammatory markers. 57 We found significantly increased TRACP 5b levels among our patients having SCD with frequent vasco-occlusive crisis and slight elevation among patients with elevated TRV. The relation between TRACP 5b and pulmonary hypertension may be evident in adult life. On the other hand, Voskaridou et al 55 found no difference as regards serum TRACP 5b among patients with SCD and osteopenia/osteoporosis or those with osteosclerosis versus healthy controls.
Increased serum TRACT 5b in patients with other erythroid disorders like patients with thalassemia has been reported. Voskaridou et al 58 reported increased NTX, TRACP 5b, bALP, and OC levels in patients with thalassemia compared with controls; and followed-up the patients during a 12-month duration of pamidronate therapy. Therapy was followed by a clear decrease in NTX, TRACP 5b, and OC, and by a significant increase in the BMD of the lumbar spine.
In this study, patients treated with hydroxyurea and those on chelation therapy showed lower TRACP 5b levels than untreated patients. This is may be because hydroxyurea is associated with decreased sickle red blood cell-derived hemoglobin and heme-derived oxidants that could activate inflammatory responses. The decrease in neutrophils, monocytes, reticulocytes, and platelet counts with hydroxyurea therapy was directly associated with decreases in 3-month crisis rates. 59 To the best of our knowledge, no previous studies examined the role of TRACP 5b in monitoring the response to therapy among patients with SCD; therefore, determining the true value of this marker will require a prospective study over a longer period including more patients to allow a more refined stratification.
In conclusion, bone complications frequently occur in patients with SCD as reflected by decreased BMD and high ALP and TRACP 5b levels. Elevated TRACP 5b levels among patients having SCD with frequent vasco-occlusive crisis denote bone involvement during crisis and suggest its potential use as a marker of disease severity. The TRACP 5b level may help in monitoring the response to hydroxyurea therapy. The lack of correlation between abnormal DXA scan and high TRACP 5b levels suggests that bone disease in SCD is multifactorial. Hemolysis and iron overload may be contributing factors in the occurrence of these complications. However, longitudinal studies with large number of patients could identify the interaction between different factors contributing to decreased bone density in SCD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.