
Abstract
Objective:
In a prospective setting, we aimed to find associations between biomarkers of the hemostatic system and the occurrence of central venous catheter (CVC)-related thrombosis in patients with hematological malignancies undergoing intensive chemotherapy.
Methods:
The study was conducted between July 2006 and August 2010 at the University Hospital Maastricht, the Netherlands. Consecutive adult patients with hematological malignancies who were going to receive a CVC for intensive chemotherapy were included. The primary end points were (a) symptomatic CVC-related thrombosis and (b) CVC-related infections. Blood samples were taken directly after catheterization, and easy to determine biomarkers (platelet count, leukocyte count, and hemoglobin level) in combination with blood group, factor VIII (FVIII), plasminogen activator inhibitor 1 (PAI-1), activated protein C (APC) resistance, and free protein S antigen were determined.
Results:
Blood was collected and analyzed from 168 patients. The incidence of symptomatic CVC-related thrombosis was 9%. In univariate analysis, white blood cell count >10.6 × 109/L, mean FVIII activity, and PAI-1 >12.2 IU/mL were found to be associated with the development of symptomatic CVC-related thrombosis.
Conclusion:
Elevated leukocyte count, high PAI-1, and high FVIII were associated with an increased incidence of symptomatic CVC-related thrombosis. We hope in future that simple, easy to determine laboratory tests that reflect the hemostatic and fibrinolytic activity in combination with clinical parameters may help to identify hematological patients at highest risk of CVC-related thrombosis and help to tailor the management of thromboprophylaxis in hematological patients undergoing CVC placement.
Introduction
Venous thromboembolism (VTE) occurs commonly in patients with cancer and is the second leading cause of death in these patients. Compared to persons without cancer, the risk of symptomatic VTE in patients with cancer is increased 4- to 7-fold. 1,2 The occurrence of VTE in patients with cancer depends on various patient-, tumor-, and treatment-related risk factors. 3 The incidence of VTE in patients with a hematological malignancy is comparable to the incidence in patients with “high-risk” solid tumors, such as colon, pancreatic, and ovarian cancers. 4 –7 Central venous catheters (CVCs) are frequently used in patients with hematological malignancies in order to administer chemotherapy, stem cell infusions, blood products, medication, and parenteral hyperalimentation, as well as for blood sampling. The benefit derived from CVCs can be offset by complications. Reported complications consist of mechanical complications during or directly after the insertion (arterial puncture, hematoma, and pneumothorax) and long-term complications like CVC-related infections and thrombosis. 8 The incidence of symptomatic CVC-related thrombosis in hematological adult patients varies between 1.2% and 13.0%. 9 Central venous catheter-related thrombosis results in patient morbidity, significant increases in the length of hospitalization, and medical care costs.
The guidelines for the treatment and prophylaxis of CVC-related thrombosis recommend against the routine administration of pharmacologic prophylaxis to prevent CVC-related thrombosis. 10,11 There is no clear consensus regarding the role of either inherited or acquired thrombophilic states in the pathogenesis of CVC-related thrombosis, 12 nor is there a clear recommendation on the use of prophylactic measures in this population. 11
The ability to stratify risk would permit appropriate use of VTE prophylaxis, if effective, only in patients at the highest risk. A model-based approach incorporating biomarkers may be the most efficient way to identify patients with cancer at highest risk of CVC-related thrombosis and to study prophylaxis strategies in these patients.
It has been shown that risk-scoring models that incorporate clinical and laboratory biomarkers are able to stratify patients with cancer into groups at high- or low risk of developing VTE. 13 –16 Data about markers for the prediction of VTE in patients with hematological malignancies are scarce because most studies are performed in patients with solid cancer.
A number of laboratory parameters or biomarkers, which are predictive for cancer-associated VTE, have been recently identified. They encompass biomarkers reflecting activation of the blood clotting system such as
In contrast to a number of studies on the association of biomarkers and cancer-associated deep vein thrombosis or pulmonary embolism, studies investigating the association between biomarkers and symptomatic CVC-related thrombosis in patients with hematological malignancies are very scarce.
In a prospective setting, we aimed to assess associations between biomarkers of the hemostatic system and the occurrence of CVC-related thrombosis in patients with hematological malignancies. We have chosen well-documented, easy-to-determine, and available biomarkers as described in the risk model of Khorana et al (prechemotherapy platelet count, leukocyte count, and hemoglobin level) 6,13 and combined these with blood group, FVIII, plasminogen activator inhibitor 1 (PAI-1), activated protein C (APC) resistance, and free protein S antigen.
Methods
Study Design and Population
This study was embedded in a prospective randomized study with the aim to compare the occurrence of CVC-related thrombosis between 2 locking solutions (Trial registration: NCT 01820962). The study was conducted between July 2006 and August 2010 at the University Hospital Maastricht, the Netherlands. Rationale, study design, and selection of the study population have been described in detail previously. 21 The main end points of the study were (a)symptomatic thrombosis and/or CVC-related infections.
Consecutive adult patients with hematological malignancies who were going to receive a CVC for intensive chemotherapy, including patients for stem cell transplantation, were included. Exclusion criteria were the presence of a CVC at admission, history of CVC-related thrombosis and/or infection, indication for anticoagulant treatment or prophylaxis, patients with totally implanted catheters, and CVCs impregnated with antimicrobial agents. Patients could only be randomized once. The study protocol was approved by the medical ethical committees and all participating patients gave written informed consent.
Central venous catheters were tunneled polyurethane double-lumen catheters (Hickman catheter or Hemoglide, Bard, Salt Lake City, Utah, USA) and were inserted in the right jugular vein by an experienced surgeon in the operating room. Catheters were inserted percutaneously by using the Seldinger technique and most CVCs were placed with the guidance of ultrasound.
The CVC tip was confirmed radiographically to lie in the distal superior vena cava/right atrium. Patients were randomized between locking the catheter lumen with either heparin 5000 IU/mL (Heparin Leo, LEO Pharma B.V., Amsterdam, The Netherlands) or 46.7% trisodium citrate (Citra-lock, Dirinco, Bern, Switzerland) using a volume exactly equivalent to the internal volume noted on each catheter. Since there were no differences in the occurrence of CVC-related thrombosis between the heparin group and the citrate group, we have included all patients in the current study regardless of the locking solution used. 21
Patients were seen at least daily on the ward and at least weekly on the outpatient department after discharge. In case of a clinical suspicion of a symptomatic CVC-related thrombosis, patients were referred to the department of Radiology for Doppler ultrasound. A diagnosis of CVC-related thrombosis was made in case of noncompressibility of the vein, visualization of an echogenic intraluminal mass, and absence of respiratory variation or monophasic flow. 22
Biomarkers
Blood samples were taken from all patients directly after catheterization and were collected in K3-EDTA tubes or citrated tubes. Hemoglobin level, platelet count, leukocyte count, and blood group were measured immediately after blood collection.
After centrifugation, aliquots of plasma samples were frozen at −80°C and stored until analysis. Factor VIII activity (ca7000, Siemens, Den Haag, The Netherlands), PAI-1 activity (TrinilizePai-1, Stago BNL, Co. Wicklow, Ireland), APC resistance (Coatest APCresistance, Chromogenix, Bedford, USA), and free protein S antigen (HemosIL, Instrumention Laboratory) were measured in citrated plasma according to the manufacturers instruction.
Statistical Analyses
After assessment of data distribution, patient characteristics and levels of biomarkers were compared between patients with and without symptomatic CVC-related thrombosis using the independent t test, Mann-Whitney U test, or Chi-square test where appropriate. Results were tested against an α of .05. All analyses were performed using SPSS 20.0 for Windows (SPSS Inc., Chicago, Illinois).
Results
Between July 2006 and August 2010, 248 patients were assessed for eligibility. Thirty-one patients declined to participate and 5 patients could not be randomized due to other reasons. Two hundred and twelve patients receiving a CVC were randomly assigned 1:1 to either locking the CVC with heparin or with citrate. Five patients were excluded (2 patients had a solid tumor, 1 patient was lost to follow-up, 1 patient eventually did not receive a CVC, and 1 patient started systemic anticoagulation). From 39 patients, no blood was collected for mainly logistical reasons (CVC placement at night or during weekend). Blood was collected and analyzed from 168 patients in the current study.
Characteristics of the study population are described in Table 1. Overall 9% (15 of 168) of patients developed a symptomatic CVC-related thrombosis and one of them developed a pulmonary embolism.
Baseline Characteristics.a
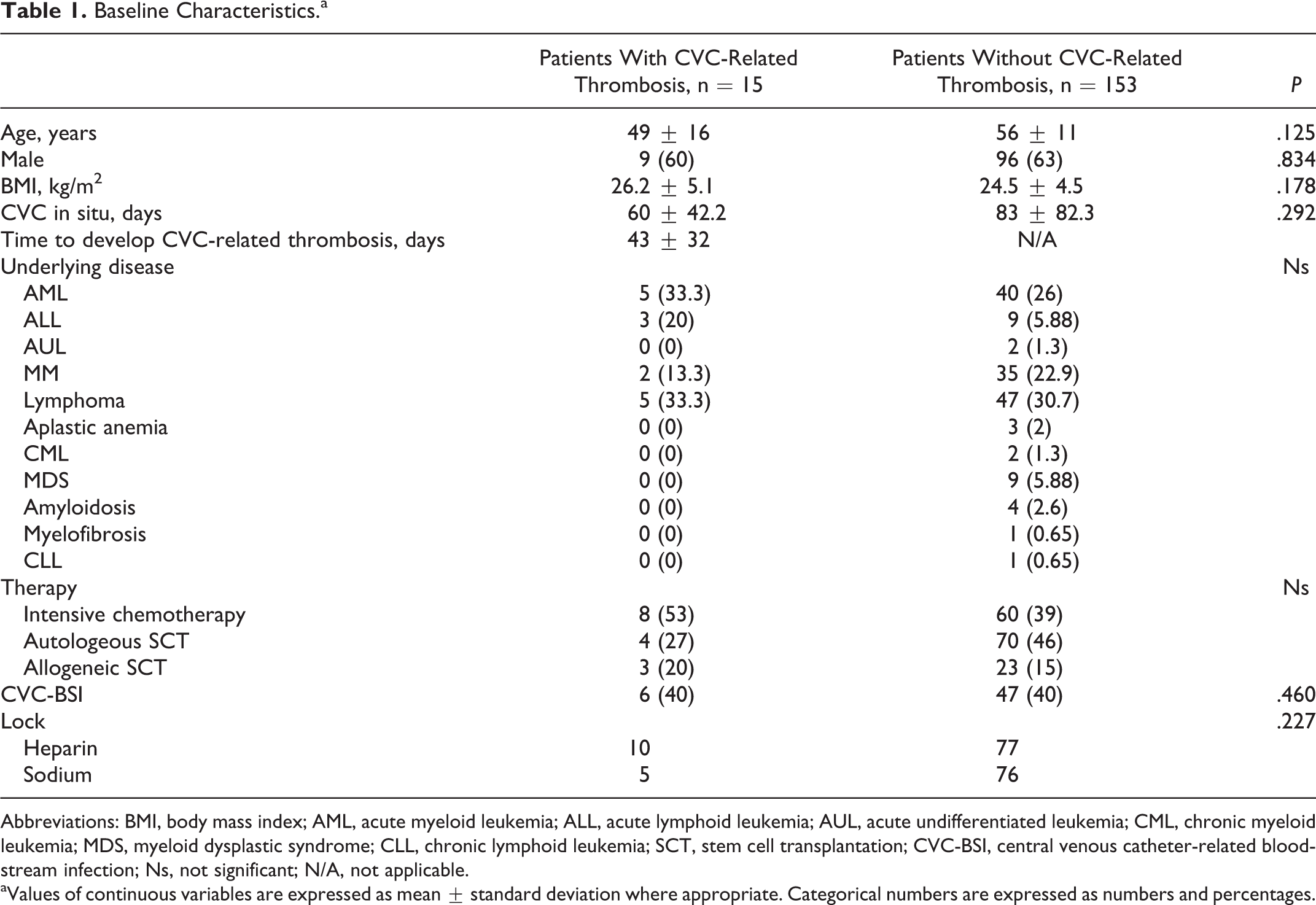
Abbreviations: BMI, body mass index; AML, acute myeloid leukemia; ALL, acute lymphoid leukemia; AUL, acute undifferentiated leukemia; CML, chronic myeloid leukemia; MDS, myeloid dysplastic syndrome; CLL, chronic lymphoid leukemia; SCT, stem cell transplantation; CVC-BSI, central venous catheter-related bloodstream infection; Ns, not significant; N/A, not applicable.
aValues of continuous variables are expressed as mean ± standard deviation where appropriate. Categorical numbers are expressed as numbers and percentages.
Of the biomarkers studied, white blood cell count > 10.6 × 109/L, mean FVIII activity, and PAI-1 > 12.2 IU/mL were found to be associated with the development of symptomatic CVC-related thrombosis in patients with hematological malignancies (Table 2). Factor VIII did not differ according to the type of malignancy (Figure 1).
Biomarkers and CVC-Related Thrombosis.a
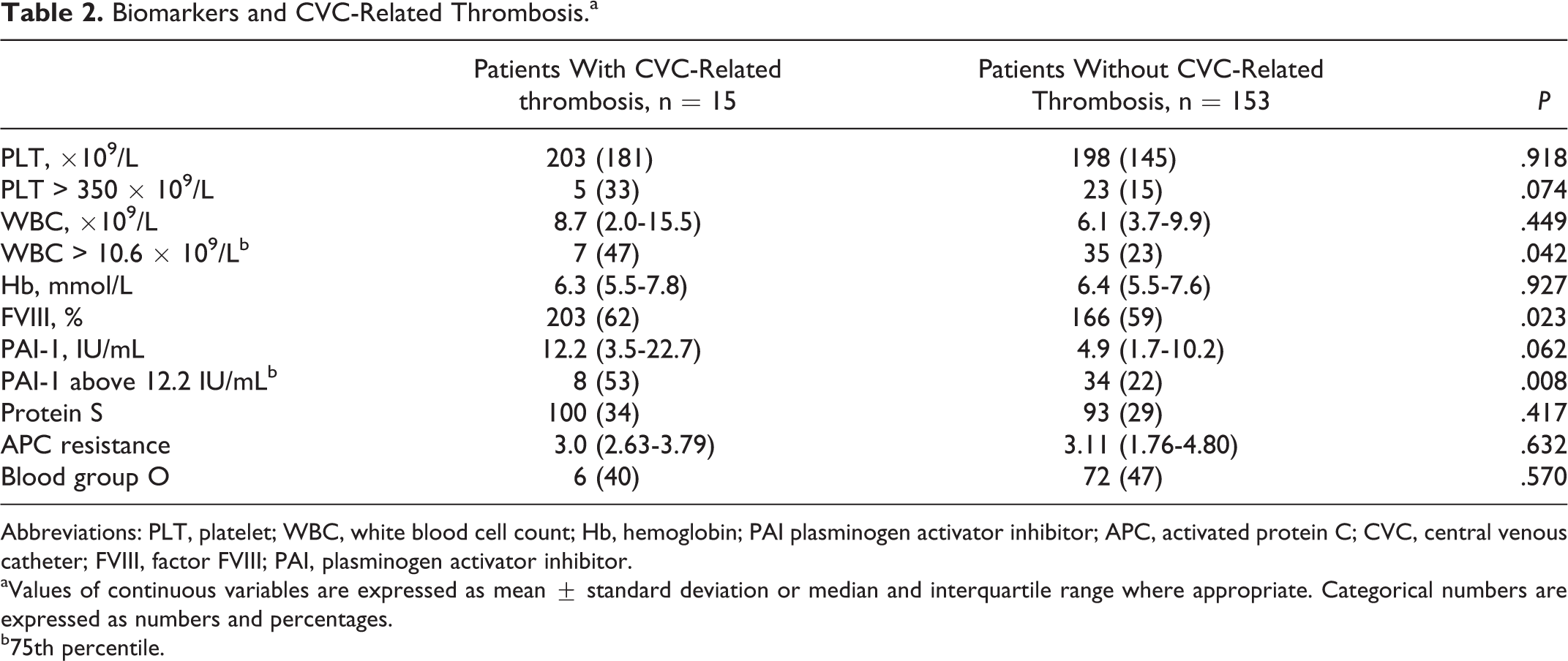
Abbreviations: PLT, platelet; WBC, white blood cell count; Hb, hemoglobin; PAI plasminogen activator inhibitor; APC, activated protein C; CVC, central venous catheter; FVIII, factor FVIII; PAI, plasminogen activator inhibitor.
aValues of continuous variables are expressed as mean ± standard deviation or median and interquartile range where appropriate. Categorical numbers are expressed as numbers and percentages.
b75th percentile.
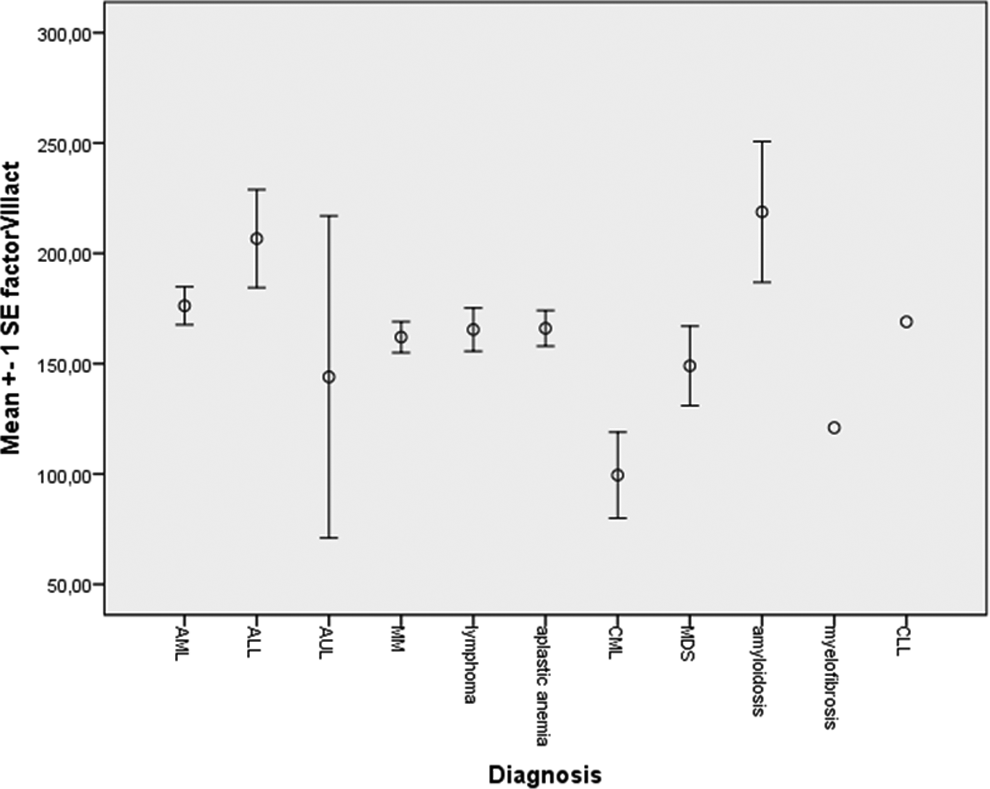
Distribution of factor VIII levels according to type of hematological malignancy. Factor VIII levels did not differ statistically significant (P = .214).
The mean platelet level at the moment of inserting the CVC did not differ between patients with and without a CVC-related thrombosis. When we limited our analysis to patients with acute leukemia, we found the mean platelet level at the moment of inserting the CVC to be 178 × 109/L (standard deviation (SD) 204) in the patients with acute leukemia developing a CVC-related thrombosis compared to 89 × 109/L (SD 89) in the patients with acute leukemia not developing a CVC-related thrombosis (P = .019).
Discussion
This is the first prospective study evaluating associations between laboratory biomarkers and the occurrence of symptomatic CVC-related thrombosis in patients with hematological malignancies undergoing intensive chemotherapy. The observed incidence of symptomatic CVC-related thrombosis in our study is 9% which is clinically relevant and consistent to incidences reported in other studies. 9
In univariate analysis, white blood cell count > 10.6 × 109/L, mean FVIII activity, and PAI-1 > 12.2 IU/mL were found to be associated with the development of symptomatic CVC-related thrombosis in patients with hematological malignancies.
Plasminogen activator inhibitor 1 inactivates tissue-type plasminogen activator (tPA) and urokinase-type plasminogen activator (uPA). As a consequence of elevated PAI-1 levels, less plasminogen is converted into plasmin thereby reducing fibrinolysis. This process favors tumor cell invasion and metastasis. 23 Reduced plasma fibrinolytic activity due to elevated plasma levels of PAI-1 has been observed in various severity of arterial thrombosis. 24 –26 The role of PAI-1 in venous thrombosis remains controversial. Although the authors of several studies have found a positive relation with venous thrombosis, others have not. 27 –29 In our study population, 53% of patients with a CVC-related thrombosis had a PAI-1 above the 75th percentile of the study population compared to only 22% in the patients without a CVC-related thrombosis (P = .008). We have not tested the frequencies of heterozygous and homozygous PAI-1 4G polymorphisms. To the best of our knowledge, no other studies have been published describing the relationship between PAI-1 and CVC-related thrombosis in hematological patients.
Elevated white blood cell count has been established as an independent risk factor for venous thromboembolic events in patients undergoing stem cell transplantation or intensive chemotherapy 20 . In our study population, we established a baseline white blood cell count above the 75th percentile of the study population to be a risk factor for CVC-related thrombosis.
Whether leukocytes themselves are causative or rather act as a surrogate marker for an underlying inflammatory process has not been conclusively established. A pathogenetic mechanism is not definitely elucidated. Neutrophil granulocytes have been implicated to play a central role as substrate for platelets. The latter can use adhesion molecules on their membranes and find ligands on the neutrophil surface causing mutual activation and procoagulant conditions. 30
In addition, we detected high levels of FVIII in our population of patients with hematological malignancies (Figure 1), probably reflecting the acute phase reactive nature of this procoagulant factor. Here also, our data are in accordance with the few available studies that reported increased FVIII levels in patients with solid tumors and hematological malignancies. 19,31 –33 High FVIII levels constitute a prevalent, dose-dependent risk factor for VTE. 19 We demonstrated that patients with a hematological malignancy with a CVC-related thrombosis have a significantly higher FVIII level compared to patients without a CVC-related thrombosis. In the group without a CVC-related thrombosis, 1 patient had a FVIII level of 8%. When this patient was excluded from the analysis, the difference between the 2 groups remained significantly different.
Reports about the thrombosis risk according to FVIII in patients with cancer are rare. Vormittag et al showed in 2009 that a high FVIII plasma level is a significant risk factor for symptomatic VTE in patients with cancer. 19 In a prospective study, Van Marion et al showed higher baseline FVIII levels in 135 patients with multiple myeloma compared to 124 age- and sex-matched healthy controls but were not able to demonstrate an increased risk of thrombosis. 34 Van Rooden et al found patients with the highest levels of FVIII to be at a not statistically significant higher risk of asymptomatic CVC-related thrombosis. 32
In general, we could not demonstrate a role for high platelet count in developing CVC-related thrombosis in our population. Only when we limited our analysis to patients with acute leukemia, we found a significant higher mean platelet count in the patients with CVC-related thrombosis. Del Principe et al also demonstrated a significant correlation between CVC-related thrombosis and a higher median platelet count in a population with patients with acute leukemia. 4 A possible explanation of this relationship in acute leukemia might be the severe hypercoagulable state due to the expression of tissue factor by the leukemic blasts or the release of procoagulant factors from the blast granular fraction. 4
Thrombocytosis is not uncommon in patients with cancer and evidence exists that platelets play an important role in tumor angiogenesis. 35 Mandala et al showed a strong association between elevated basal platelet counts and the risk of VTE during adjuvant chemotherapy. 36 Simanek et al demonstrated a high platelet count to be strongly associated with the occurrence of VTE in patients with cancer having active disease, exceeding an at least 3-fold increased risk at a cutoff at the 95th percentile of their patient cohort (443 × 109/L). 18 These results are in agreement with the retrospective study of Zakai and the prospective study of Khorana that used a cutoff of 350 × 109/L. 6 Only a few patients with hematological malignancies were included in these analyses.
The reason why platelet count in our study was not a strong risk factor as reported in other malignancies may be the relatively low platelet count patients with a hematological malignancy often present with.
Some limitations of this study have to be considered. Our study had a limited sample size and therefore only a limited number of events. Only univariate analyses were performed. The biomarkers were measured only once at study inclusion. We cannot exclude that biomarker levels might have changed during the course of disease and under treatment.
In conclusion, CVC-related thrombosis in patients with a hematological malignancy is prevalent. Simple, easy-to-determine laboratory tests such as white blood cell count, factor VIII, and PAI-1 in combination with clinical parameters may help to identify hematological patients at highest risk of CVC-related thrombosis and help to tailor the management of thromboprophylaxis
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received financial support for the research from Dirinco B.V., Bern, Switzerland. They received no financial support for the authorship, and/or publication of this article.