
Abstract
Hemorheology, a measure of rheological properties of blood, is often correlated with cerebral blood flow and cardiac output; an increased blood viscosity may increase the risk of thrombosis or thromboembolic events. Previous studies have reported a large variation in hemorheological properties of blood among smokers. This prompted us to conduct coagulation experiments to evaluate the effect of cigarette smoking on hematological parameters, like cell counts, and coagulation parameters among young males in Al-Jouf region, Saudi Arabia. The hematological and coagulation parameters were used to relate the changes in viscosity and coagulation to smoking. A total of 321 male participants (126 nonsmokers and 195 smokers) were enrolled into the study as randomized sample. Complete blood count was measured by hematology analyzer, and coagulation tests were performed by coagulation analyzer. The t test analysis was performed to compare the relationships of variables between the 2 groups. The results confirmed that smoking alters some hematology parameters leading to significant deterioration in blood flow properties. Smoking also increased the hematocrit (HCT), whole blood viscosity (WBV), and plasma viscosity (PV) but decreased the international normalized ratio (INR). The decrease in INR was found to be associated with the increase in WBV, PV, and HCT. Further investigations are necessary to assess the reversibility of such changes in cessation of smoking or other elements of influence.
Introduction
The study of blood rheology has been the subject of continuing interest in the clinical field as well as for biomedical research for many years. Both blood and plasma as biofluids have the property that describes a fluid’s resistance to flow. In a previous study, hematological and rheological properties showed correlation between hematocrit (HCT), whole blood viscosity (WBV), plasma viscosity (PV), and number of cigarette smoked per day. 1 The relative viscosity of plasma (compared to water) is about 1.8 times at 37°C and is connected to the protein composition of the plasma. 2 The blood has a relative viscosity of 3 to 4 depending upon HCT, temperature, flow rate, vessel diameter, and other factors. Hematocrit is the most important determinant of the viscosity of blood. 3,4 As HCT increases, there is a disproportionate increase in viscosity. For example, at a HCT of 40%, the relative viscosity is 4 when measured in vitro in a viscometer. At an HCT of 60%, the relative viscosity is about 8. Therefore, a 50% increase in HCT from a normal value increases blood viscosity by about 100%. 5 Such changes in HCT and blood viscosity occur in patients with polycythemia. Temperature is another factor affecting the blood rheological properties. As body temperature increases, there is an increase in blood viscosity. In addition to HCT and temperature, other factors have associations with blood viscosity including body mass index and high blood pressure that could theoretically cause high HCT. 3,4 Any increase in blood viscosity will cause decrease in the blood flow, while a decrease in vessel diameter will decrease the blood flow and the circulation in the human body. Hemorheology plays an important role in atherosclerosis. 6 There is increasing evidence indicating that flow properties of blood are among the main determinants of proper tissue perfusion and alterations in these properties play significant roles in disease processes. 7 A strong correlation has been found between cigarette smoking and atherosclerosis and cardiovascular disease. Various epidemiological studies have investigated the possible associations between blood rheology (ie, hematological characteristics that could influence blood flow) and coronary heart disease rates. 8,9
The World Health Organization (WHO) has described tobacco smoking as an epidemic. 10 The worldwide smoking epidemic is expected to remain as one of the highest causes of premature death and diseases. The WHO has estimated that the number of deaths each year from smoking-related disease will increase to 10 million within the next 30 years or so, of which 70% will occur in developing countries. 11 Smoking is socially not accepted in Saudi Arabia and the country does not allow to grow tobacco or manufacture cigarettes, although they do not restrict the sale of cigarettes for more than 50 years. Cigarette sales have increased dramatically over the years, and an average of 600 million Saudi Riyals (about US$160 million) are spent annually on tobacco. 12
The number of nationwide studies on the hematological and viscosity changes with smoking is limited. The present study was useful to determine the changes in blood coagulation, viscosity, and other hematological factors due to smoking among the male participants in Al Jouf region, Kingdom of Saudi Arabia. The study samples consisted of male only because smoking was not socially accepted, especially for females in Saudi Arabia, and also because of the difficulties in obtaining samples from female smokers in Saudi Arabia. Besides, physiological parameters of females change according to menstruation periods every month. Therefore, it will be difficult to distinguish between the changes due to smoking and regular hormonal changes in the menstrual cycle.
Materials and Methods
A total of 321 male participants (126 nonsmokers and 195 smokers) were enrolled into the study as a randomized sample set. Informed consents were obtained from the participants invited to participate in the study from the premarital counseling clinic in Abdelrahman Elsidarri Hospital, Al Jouf, Saudi Arabia. Consents and all ethical relevant procedures were designed according to The National Committee Of Medical & Bioethics - King Abdulaziz City For Science and Technology (NCBE-KACST) and Al Jouf University bioethics committee guidelines. The age of the participants ranged from 17 to 40 years. The rate of cigarette consumption of the smoker group ranged between 10 and 50 cigarettes/d. One tube of venous blood was collected from each participant (one tube: 2 mL) for blood count assessment and the other 2 tubes (2 and 4 mL) for WBV and PV assessments, respectively. For coagulation, (Becton Dickinson, New Jersy, USA) tubes with citrate plasma (1:9) were used. While K2-EDTA 3.6 mg/2 mL and 7.2 mg/4 mL were used for CBC. The complete blood count (CBC) was measured by SYSMEX SE-9500 in the hematology laboratory of Abdelrahman Elsidarri Hospital, and the blood viscosity was measured by U-tube viscometer (Pisco Brand Precision Scientific Glass Apparatus, India; capillary U tube) at room temperature in the hematology laboratory of the College of Health Sciences, Al Jouf University. The coagulation tests were performed by coagulation analyzer (Bio Solea 4, Biolabo Maizy, France) at the same laboratory. Data of variables were analyzed by SPSS 17.0, Graphpad QuickCalcs ©2012, and Microsoft Office Excel 2007 software. A 2-tailed P value <.05 was considered statistically significant.
Results
Hematological Parameters
The results of the blood count showed variations in the hematological parameters as depicted in Table 1. The variations in the blood cell count between smokers and nonsmokers were found to be statistically significant in certain parameters including hemoglobin (Hb), mean corpuscular hemoglobin (MCH), MCH concentration, platelet (PLT), monocyte, and eosinophil counts.
Mean Level of the Blood Count for Smokers and Nonsmokers.
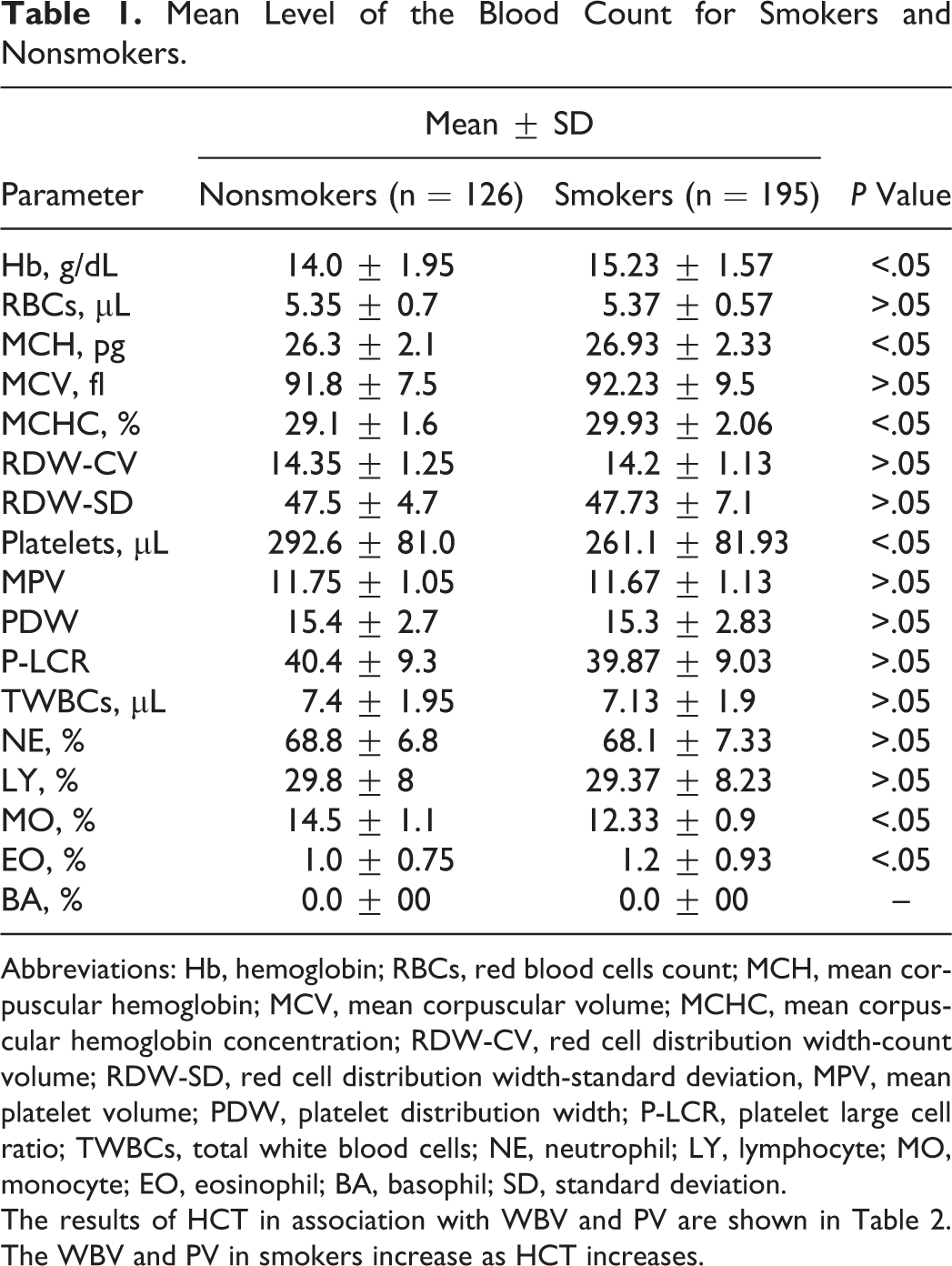
Abbreviations: Hb, hemoglobin; RBCs, red blood cells count; MCH, mean corpuscular hemoglobin; MCV, mean corpuscular volume; MCHC, mean corpuscular hemoglobin concentration; RDW-CV, red cell distribution width-count volume; RDW-SD, red cell distribution width-standard deviation, MPV, mean platelet volume; PDW, platelet distribution width; P-LCR, platelet large cell ratio; TWBCs, total white blood cells; NE, neutrophil; LY, lymphocyte; MO, monocyte; EO, eosinophil; BA, basophil; SD, standard deviation.
The results of HCT in association with WBV and PV are shown in Table 2. The WBV and PV in smokers increase as HCT increases.
Mean Level of HCT, WBV, and PV Levels in Nonsmokers and Smokers, Al Jouf Region.
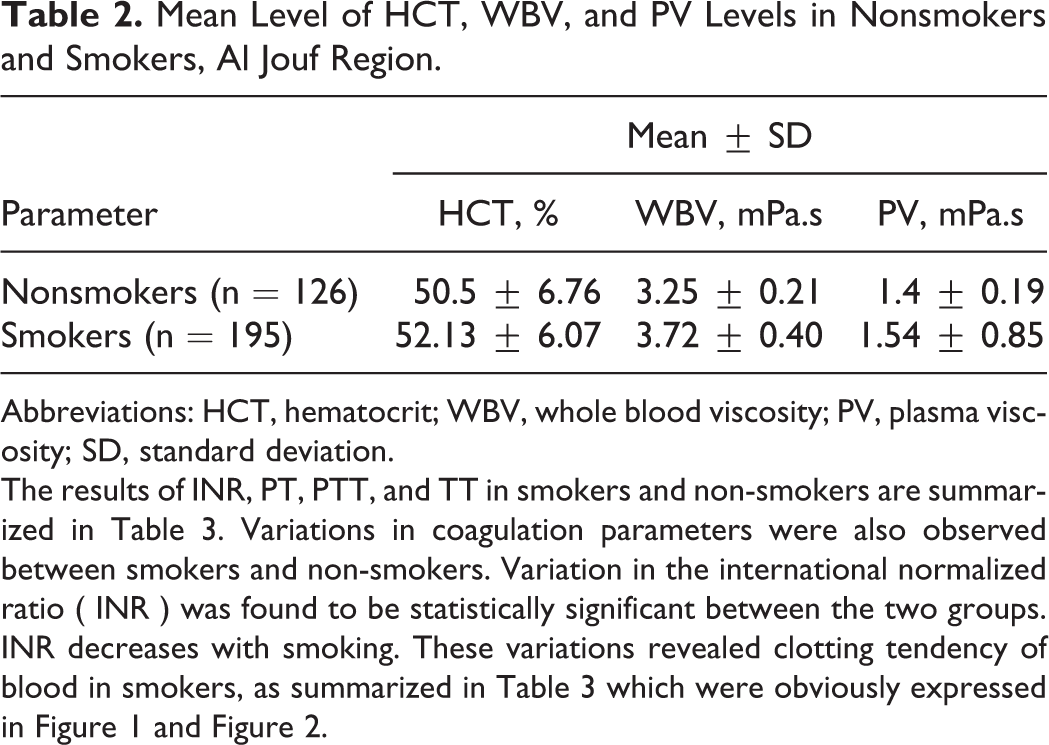
Abbreviations: HCT, hematocrit; WBV, whole blood viscosity; PV, plasma viscosity; SD, standard deviation.
The results of INR, PT, PTT, and TT in smokers and non-smokers are summarized in Table 3. Variations in coagulation parameters were also observed between smokers and non-smokers. Variation in the international normalized ratio ( INR ) was found to be statistically significant between the two groups. INR decreases with smoking. These variations revealed clotting tendency of blood in smokers, as summarized in Table 3 which were obviously expressed in Figure 1 and Figure 2.
Mean Level of INR, PT, PTT, and TT Levels in Nonsmokers and Smokers, Al Jouf Region.
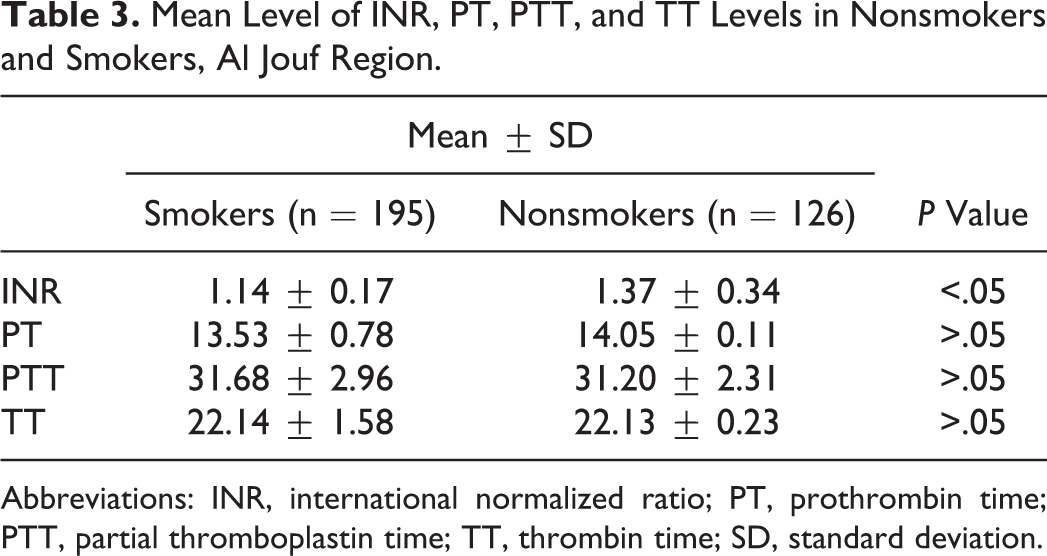
Abbreviations: INR, international normalized ratio; PT, prothrombin time; PTT, partial thromboplastin time; TT, thrombin time; SD, standard deviation.
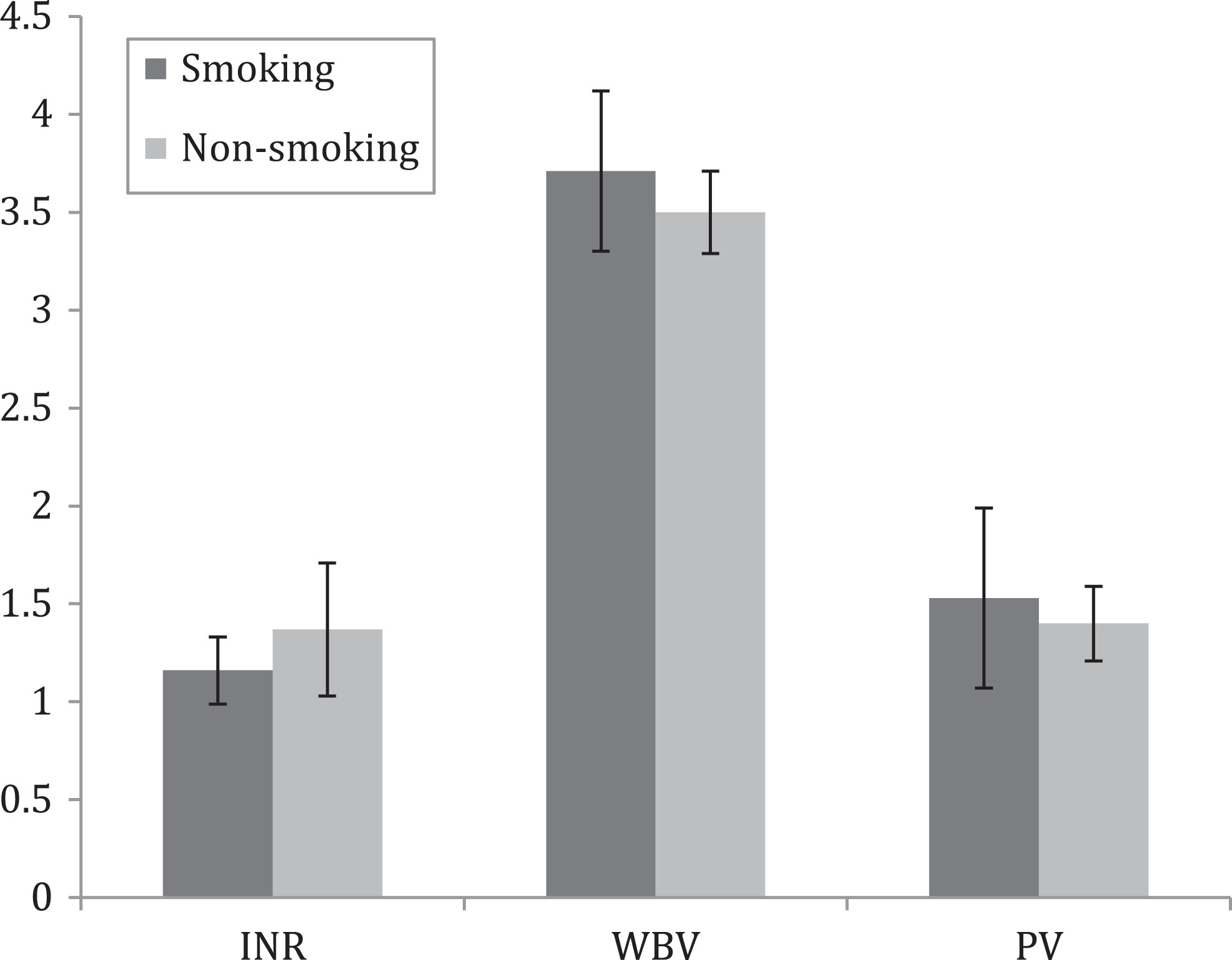
International normalized ratio (INR) with smoking proportional to whole viscosity (WBV) and plasma viscosity (PV). (Smoking n = 195, Non-smoking n = 126).
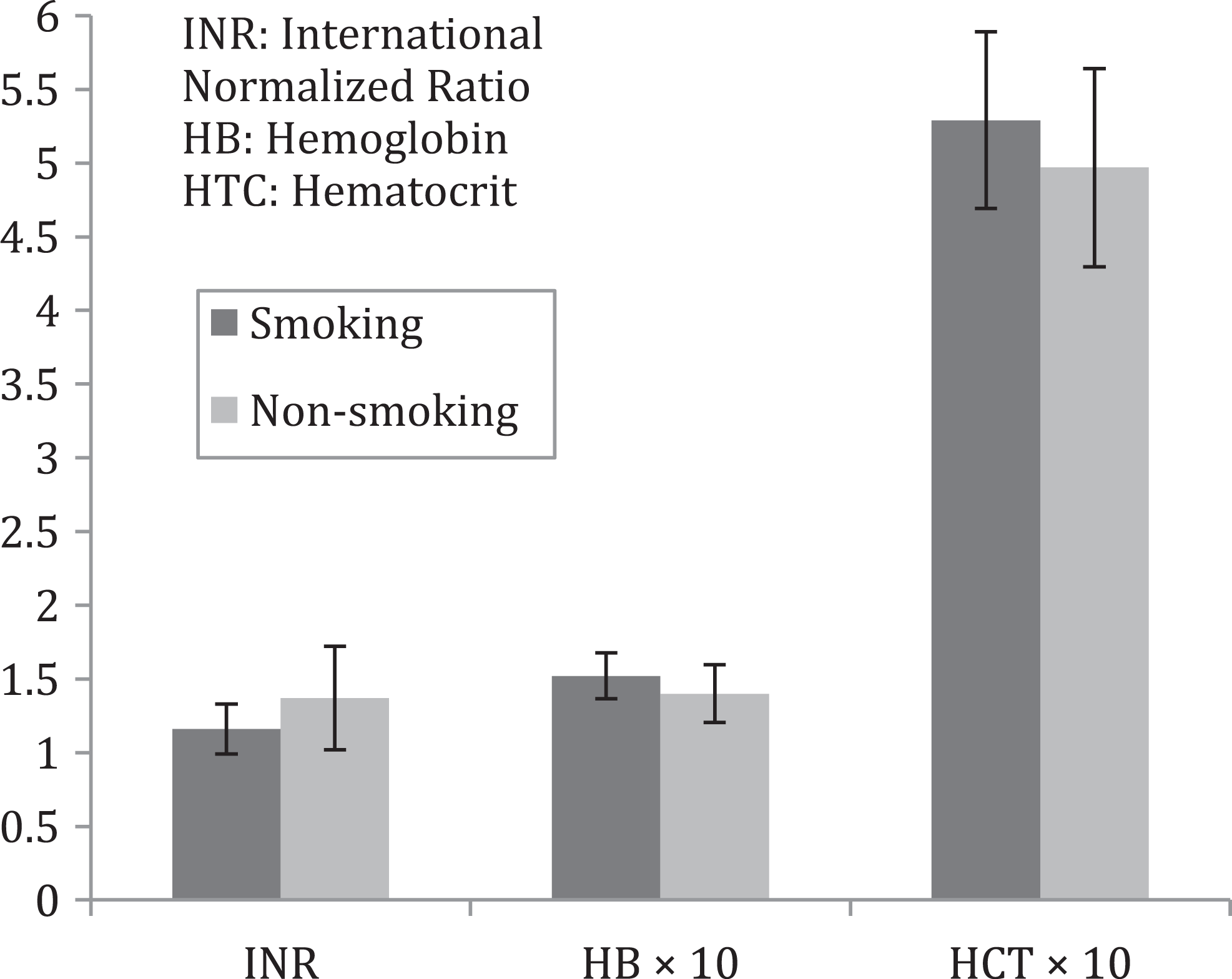
International normalized ratio (INR) with smoking proportional to hemoglobin (Hb) and hematocrit (HCT). (Smoking n = 195, Non-smoking n = 126).
Discussion
Rheology and cell count were used as a means to obtain information about changes in blood and related it to smoking. Conducting hematorheological experiments might answer some questions in the area of hematology and cardiovascular diseases. It was evident that the smoking increases the HCT, WBV, and PV, while the international normalized ratio (INR) decreases with smoking. The decrease in INR was found to be associated with the increase in WBV, PV, and HCT. Research in this area suggests the significance of the influence of smoking on alterating properties of the blood including viscosity. The present work confirms the mentioned influence and suggests the influence of coagulation parameters in combination.
Erythrocytes count in smokers showed no statistical significance compared with nonsmokers, but this may reflect differences in methodology or populations studied. Similar observations were also made earlier. For example, Grigoleit et al 13 found a reduced red cell filtration in men but not in women while Landgraf and Ehryl recorded a slight but not significant reduction in red cell filtration in both sexes. 14 Additionally, Lagrue et al and Lowe and coworkers showed a significant reduction in red cell filtration after smoking of 2 or 3 cigarettes. 15,16 This is also in agreement with another study reported by Ehrly and Schumpf 17 who found no significant alteration in red cell parameters counts after cigarette smoking. 17,18
It has been confirmed that there is no significant effects of carbon monoxide on the physicochemical state of Hb. 19 The main concern is about the exposure to carbon monoxide (carbon monoxide reduces plasma volume) and how it affects the circulating catecholamines. Mean of all red cell parameters was normal in the both smokers and control group of nonsmokers. Further investigations would be required to assess whether hematorheological changes were reversible in smoking cessation and to investigate their elements of influence. Hematorheological studies for smokers, both physiologically and pathologically, are suggested based on in vitro and in vivo and exposure criteria.
Conclusion
In conclusion, the present study clearly demonstrated that CBC, viscosity, and coagulation parameters for smokers are slightly different from those of nonsmokers. This study has also documented different red blood cell, white blood cell, WBV, PV, INR, and PLT parameters. We suggest that our results should be considered as reference values in Al Jouf region. Smoking not only leads to a rise in HCT concentration but also alters the rheological properties by increasing WBV and PV levels, and most importantly, it decreases blood coagulation as evident from INR which directly affects the cardiovascular health. Further prospective studies would be required to establish the influence of the blood rheological changes in the overall health. It is equally important to investigate whether the hematological and hemorheological changes associated with cigarette smoking were reversible after smoking cessation.
Footnotes
Acknowledgments
The authors wish to thank Mr Abdelgader Abdulgader for excellent technical assistance in this project. The authors would also like to acknowledge the Department of Medical Laboratory Science, College of Health Science in Al Jouf University, for the help provided to complete this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Al Jouf University through the Research Vice-Presidency.