
Abstract
Background and Aim:
Hepcidin has been shown to be an acute phase reactant, induced by infection and inflammation. Ongoing inflammation was shown in rheumatic valve disease (RVD). In this study we want to investigate whether there is a relationship between inflammation and impaired iron metabolism and the role of hepcidin on serum iron levels.
Methods and Results:
Fourty-six patients with RVD and 34 healthy individuals were included in the study. Serum hepcidin, high-sensitive C-reactive protein (hs-CRP), hemoglobin, hematocrit, iron, iron-binding capacity, ferritin levels were measured. Serum hepcidin levels were significantly increased in patients with RVD than in control group (316 ± 121 ng/mL vs 435 ± 126 ng/mL; P < .001). Serum hs-CRP levels were no significantly higher in the patient group in than in the control group (3.9 ± 3.6 mg/L vs 3.5 ± 3.7 mg/L; P = .521).
Conclusion:
Hepcidin levels are decreased independently from hs-CRP levels as a compensatory mechanism to increase the iron absorption in response to decreased serum iron levels in patients with RVD.
Introduction
Hepcidin is a peptide hormone consisting of 25 amino acids, which is rich in disulphides and primarily synthesized in the liver. In the body, it regulates iron absorption from the intestines and iron transfer from tissues that release iron to plasma. It is a negative regulator hormone that reduces intestinal iron absorption in iron overload. 1 Serum hepcidin levels are also significantly reduced in conditions such as anemia and hypoxia so that iron absorption from the intestines may increase. 2 –4 Apart from its negative regulator involvement in iron metabolism, hepcidin plays a regulator role in iron metabolism of the body during inflammation, both acute and chronic. Hepcidin exerts this activity via interleukin 6 (IL-6). Released in response to inflammation, IL-6 stimulates hepcidin production in the liver. 5,6 Increased levels of hepcidin, on the other hand, inhibits iron absorption from the intestines and release of iron from the reticuloendothelial system to circulation, thereby resulting in reduced levels of iron in blood. Recent studies have suggested that increased hepcidin levels secondary to chronic inflammation was responsible for the hematologic picture in anemia associated with chronic diseases. 7,8
Rheumatic valve disease (RVD) is a chronic process with ongoing inflammation and there are limited studies investigating iron metabolism. The objective of the present study is to investigate the correlations between hepcidin, which is believed to have an important involvement in iron metabolism in RVD, and levels of high-sensitive C-reactive protein (hs-CRP), a marker of progressing inflammation, as well as the correlations between these two and other agents involved in iron metabolism.
Methods
The present study included 46 patients (34 females and 12 males; mean age 46.7 ± 10.7) diagnosed with RVD and 34 healthy individuals (24 females, 14 males; mean age 44.5 ± 10.6) with no RVD established by echocardiography as the control group. Individuals with focal or systemic inflammation, cardiac conditions other than valve disease, those with mechanical valve, respiratory conditions and malignancies or hematological diseases were excluded from the study. The study was approved by the ethics board of the hospital where the study was conducted. Informed consents were obtained from each subject.
Echocardiography Assessments
Transthoracic echocardiographic studies were performed with the patients in the left lateral decubitus position using a Vivid 7 system (Vingmed Ultrasound, Horten, 1”Norway). Two-dimensional echocardiography was performed and measurements were obtained in accordance with the recommendations of the American Society of Echocardiography. 9 The mitral valve area was measured using planimetry or pressure half-time methods. Mitral regurgitation was defined as mild, moderate, or severe on the basis of whether the regurgitate signals were localized only up to the proximal third of the left atrium. 10 –12 Aortic regurgitation was considered mild if the signals were recorded only from localized area in the left ventricular outflow just below the aortic valve; aortic regurgitation was considered moderate when the signals extended to the level of the tip of the anterior leaflet of the mitral valve; it was severe when the signals extended well into the apical portion of the left ventricular cavity. 13 –15 Aortic valve regurgitation was assessed from the ratio of aortic regurgitate width to left ventricular outflow tract width. Valve regurgitation including the mitral, aortic and tricuspid valves was graded as 1 (mild), 2 (moderate) or 3 (severe). Aortic stenosis was classified according to gradient as follows: < 25 mm Hg as mild, 25 to 40 mm Hg moderate and > 40 mm Hg severe. 16
Venous blood samples were drawn, when patients were admitted to the coronary care unit. Iron, total iron-binding capacity (TIBC), ferritin and other biochemical characteristics were assayed by standard laboratory methods. Serum samples were stored at −20°C for a short period of time. Plasma hepcidin levels were measured with Hepcidin enzyme-linked immunosorbent assay (ELISA; Solid Phase ELISA) kits manufactured by DRG International Inc (USA), hs-CRP levels were obtained with kits from American Diagnostica (Greenwich, conn), and serum ferritin levels were measured by Electrochemiluminescence method by a Roche Elecsys 2010 device.
Statistical Analysis
Data are expressed as means + SD or median with interquartile range as appropriate. Unpaired data were compared using the Fishers’ Exact test (for categorical variables), and the unpaired t-test or Mann-Whitney U test (for continuous variables). Paired data were compared with the use of the paired t-test or Wilcoxon rank sum test. Correlations were calculated using Pearson’s correlation test. Skewed data were log-transformed before correlations and linear regression analyses were calculated. P values, .05 were considered to represent statistical significance. The Statistical Package for Social Sciences (SPSS, Chicago, IL) version 17 was employed for all statistical analysis.
Results
There were no significant differences between patients and controls in terms of age and gender (P = .361 and P = .175, respectively). The basal clinical characteristics and echocardiographic data of patients with RVD are presented in Tables 1 and 2. Plasma levels of hepcidin were significantly increased in patients with RVD than in controls (435 ± 126 vs 316 ± 121; P < .0001). Serum hs-CRP levels were nonsignificantly increased in patients with RVD (3.9 ± 3.6 vs 3.5 ± 3.7; P = .643). However plasma iron levels were significantly lower in patients with RVD (60 ± 28 vs 82 ± 32; P = .002; Tables 1 and 2). Hemoglobin, TIBC, and ferritin levels were similar between two groups. In multivariate linear regression analyses that iron, TIBC, ferritin and hs-CRP had significant effect on hepcidin (P = .012). Correlation among plasma hepcidin and echocardiographic parameters are detailed in Table 3. There was no correlation between hepcidin levels and, severity of mitral stenosis, mitral regurgitation, aortic regurgitation, aortic stenosis, plasma hsCRP, iron, TIBC and ferritin levels.
The Demographics and Clinical Laboratory Parameters of the Patients and the Control Group.a
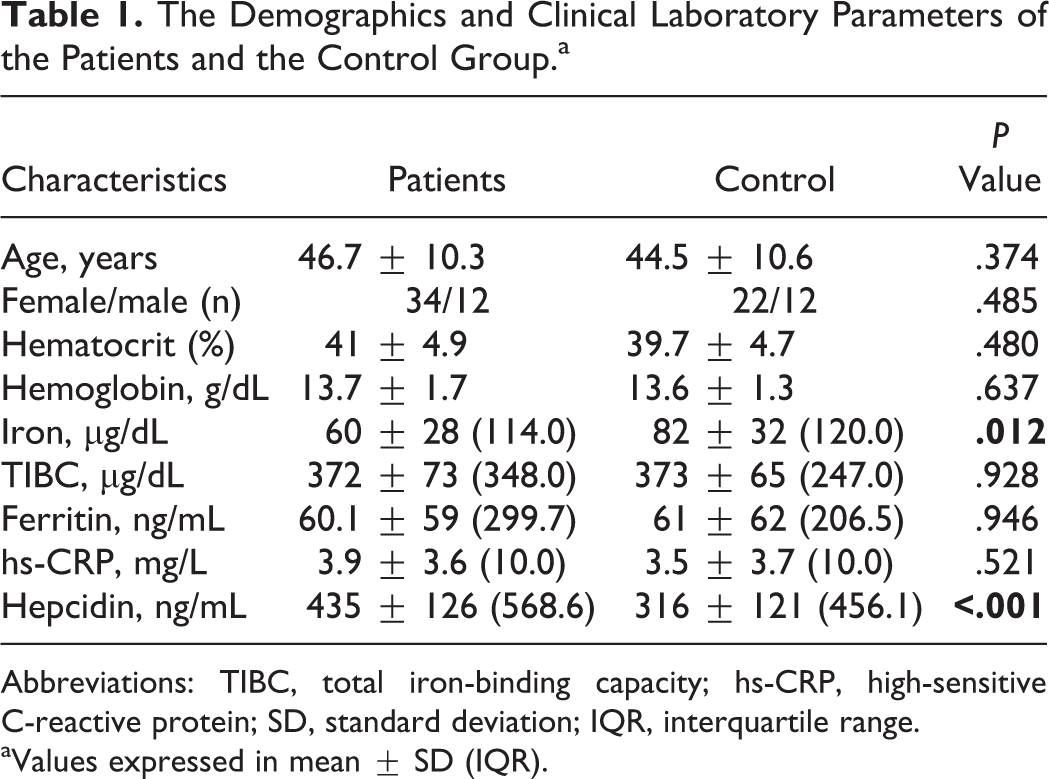
Abbreviations: TIBC, total iron-binding capacity; hs-CRP, high-sensitive C-reactive protein; SD, standard deviation; IQR, interquartile range.
aValues expressed in mean ± SD (IQR).
Echocardiography Characteristics of Patients.
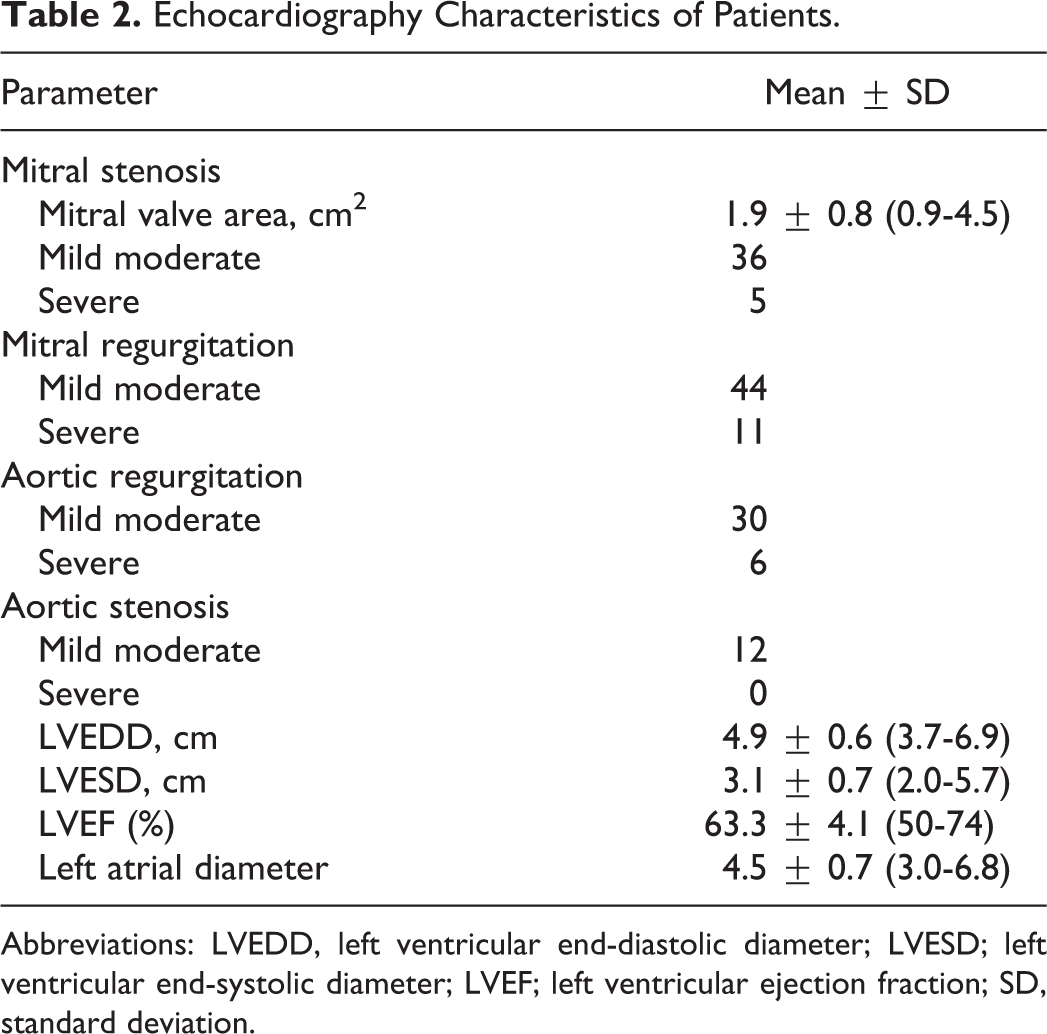
Abbreviations: LVEDD, left ventricular end-diastolic diameter; LVESD; left ventricular end-systolic diameter; LVEF; left ventricular ejection fraction; SD, standard deviation.
Correlations Between hs-CRP, Hepcidin Levels, and Clinical and Echocardiographic Parameters.
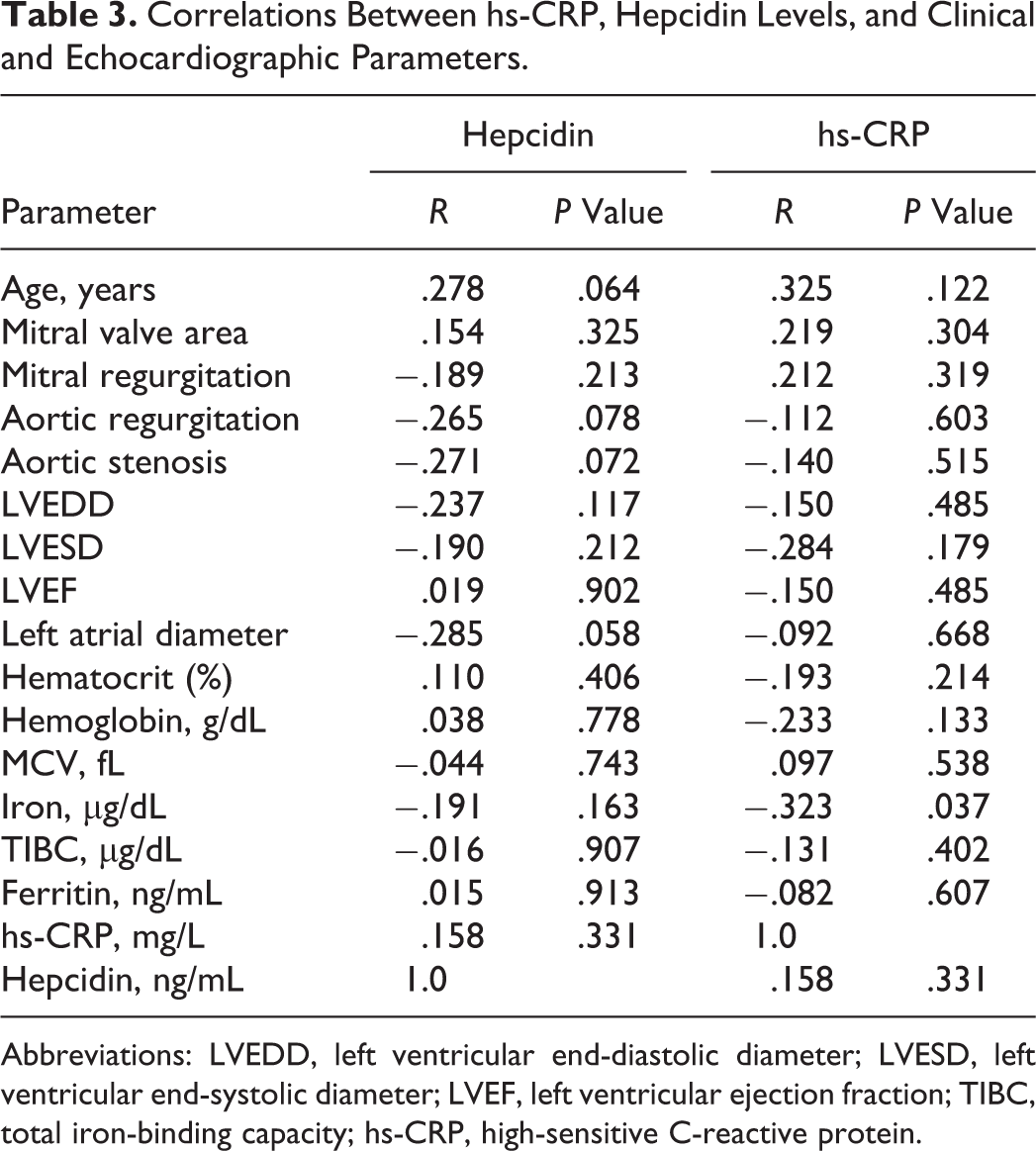
Abbreviations: LVEDD, left ventricular end-diastolic diameter; LVESD, left ventricular end-systolic diameter; LVEF, left ventricular ejection fraction; TIBC, total iron-binding capacity; hs-CRP, high-sensitive C-reactive protein.
Discussion
Serum iron levels were significantly decreased and hepcidin, which has significant roles in iron metabolism, was increased despite the absence of anemia in patients with RVD in our study. Levels of hsCRP, a marker of an ongoing inflammation, were also no significantly higher in subjects with RVD. This slow-progressing inflammation results in subclinical impairment in iron metabolism in RVD and such patients should be monitored closely for occurrence of future problems similar to chronic disease anemia.
Hepcidin is a peptide hormone with an established significant role in the iron metabolism of the body which can be detected both in the urine and blood. The major hepcidin form was a cationic peptide with 25 amino acid residues and 4 disulfide bridges. This hormone is primarily synthesized in the liver to prevent iron absorption from the intestine and it has also been shown that it is synthesized in other tissues than the liver, for example in the kidneys. 18 –22 However, hepcidin synthesized in tissues other than the liver is believed to have paracrine effects rather than systemic activity. In iron overload, hepcidin levels increase significantly while, in anemia and in conditions associated with increased oxygen need in the tissues such as hypoxia, hepcidin synthesis is decreased, resulting in increased iron absorption from and iron storage in the intestines. 1 –3 Hepcidin is also elevated in conditions associated with chronic inflammation such as Systemic lupus erythematosus and Rheumatoid arthritis, and it is currently believed that the occurrence the hematologic picture described for chronic disease anemia characterized by low serum iron but normal TIBC and ferritin levels is mainly attributable to hepcidin. 23,24
A significant role of hepcidin has been demonstrated in excessive iron storage in the tissues in conditions such as hemochromatosis and, thus, in conditions associated with tissue damage. 17 –20 Recent publications have suggested that hepcidin levels were altered in acute myocardial infarction and heart failure. 25 –27 Studies investigating levels of iron and agents involved in iron metabolism in rheumatic valve disease are very limited. A study by Brodeur et al described a shortened erythrocyte life span in patients with aortic valve disease despite the absence of anemia, which was not found to be linked with aortic gradient, aortic valve area, cardiac output and valve calcification. Similarly, in a study by Roeser et al, iron deficiency was noted in only 2 of 15 patients with valve disease, while bone marrow assays demonstrated reduced iron depot in 8 patients. 28 –30 High-sensitive CRP is an important marker of an ongoing inflammation in RVD. Gölbasi et al have also observed increased levels of hsCRP in RVD. 32 Similarly, Davutoglu et al noted increased levels of hsCRP and other markers of inflammation. 33 The same study identified a strong correlation between inflammatory markers and patient’s functional capacity and degree of valve involvement.
In our study, neither hepcidin nor hsCRP levels correlated with the degree of valve involvement. Absence of a correlation between hepcidin levels and iron metabolism–related parameters or severity of valve involvement may be associated with the fact that the tested prohepcidin does not optimally reflect physiological or pathological changes in mature hepcidin concentrations like in other assays.
We therefore believe that more dependable results may be obtained after more reliable tests are made available commercially. The absence of a correlation between hsCRP levels and valve involvement may be associated with the less severity of valve involvement in our patient group compared to the study by Davutoglu et al, where hsCRP levels were more than 10-fold higher than that in the control group, indicating more severe inflammation compared to our study, which demonstrated that inflammation in the patient group was about twice higher than that in the control group. In a study by Nemeth et al, hepcidin excretion in chronic inflammation or in significant inflammatory disease was increased by approximately 100-fold, whereas the increase was much more modest in less severe inflammatory conditions. 6 In our study, approximately 3-fold increased hepcidin levels and 2-fold increased hsCRP levels indicate that the ongoing inflammation in the patients included was not very severe. In the patient group with more severe inflammation in the study by Davutoglu et al, a significantly higher increase can be expected based on the severity of inflammation.
In conclusion, the levels of hepcidin as an important component of iron metabolism were found to be increased in RVD with a slow ongoing inflammatory process, and serum iron levels were also increased, though without clinical relevance, indicating that a potential subsequent clinical condition similar to chronic anemia may be problematic in RVD, particularly in patients with more severe course of inflammation. Clinicians should therefore bear this possibility in mind in the long-term monitoring of such patients.
Limitations
Because prohepcidin kit was commercially available for hepcidin-level investigations at the time the study was initiated, this test was used. However, later studies have reported some limitations for this assay. Ganz et al asserted that they were unable to attain sufficient correspondence with actual clinical practice due to some factors associated with the instability of prohepcidin. 31 The fact that the anticipated correlation could not be established between clinical and laboratory parameters demonstrated by Kulaksiz et al supports this assertion. 22 Currently, kits that can detect hepcidin (known to be better correlated with clinical results) with high sensitivity and specificity in blood are under development, and we believe that the results with higher clinical relevance can be obtained with this assay. 31
Another limitation was that levels of IL-6, which is believed to be responsible for the mechanism of action of hepcidin, could not be studied due to financial limitations. Hepcidin synthesis occurs via IL-6 and therefore analyses of IL-6 level in future studies will provide an opportunity for better understanding of iron metabolism in chronic inflammation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.