
Abstract
Our aim is to present the etiology and risk factors for cerebral sinovenous thrombosis (CSVT) and the radiological findings, anticoagulant therapy used, and treatment outcome of patients with CSVT. This study included 12 patients who were treated for CSVT at the Ankara University, School of Medicine, Department of Pediatric Neurology. This study included 5 girls (41.7%) and 7 boys (58.3%) with a mean age of symptom onset of 5.2 ± 6.29 years (range: 0-18 years), who were followed at our institution for a mean of 1.8 ± 1.73 years (range: 0-6.5 years). Among the patients, 3 had no risk factors, 2 had 1 risk factor, and 7 had multiple risk factors. Anticoagulant therapy was administered to 4 patients, of which 1 had neurological sequelae; neurological sequelae or exitus occurred in 4 of the 8 patients who did not receive anticoagulant therapy. The present findings showed that appropriate prophylaxis in appropriately selected patients reduced the rate of recurrence of CSVT.
Introduction
Cerebral sinovenous thrombosis (CSVT) rarely occurs in children. Previous studies reported that the annual incidence of childhood CSVT is 0.25 to 0.67 per 100 000 children but is increasing due to greater clinical awareness, more sensitive neuroimaging techniques, and the survival of children with previously lethal diseases that confer a predisposition to sinovenous thrombosis. 1 –4
The clinical symptoms of CSVT are varied. Seizures of various subtypes accompanied by focal or diffuse neurologic signs are the most common presentation in neonates, 1,4,5 whereas in children headache, papilledema, and focal neurological deficits are the principal clinical manifestations. 6 A wide range of possible risk factors have been shown to be associated with pediatric sinovenous thrombosis. Direct injury to the venous sinuses, chronic inflammatory diseases, nephrotic syndrome, head and neck infection, malignancy, and dehydration plays important roles in the etiology. 1,7 Prothrombotic abnormalities have been reported to be present in 33% to 99% of children with CSVT. 8 Despite an increased understanding of the natural history of pediatric cerebral thrombosis, its mortality rate remains significant (5%-12%), and neurological sequelae occur in 61% to 74% of children with CSVT. 9,10
The present study aimed to present the etiology and risk factors for sinovenous thrombosis and the radiological findings, anticoagulant therapy used, and treatment outcome of patients who were treated for CSVT at Ankara University, School of Medicine, Department of Pediatric Neurology, Ankara, Turkey, during a 10-year period.
Materials and Methods
This retrospective study included 12 patients treated for CSVT between January 2002 and August 2012, who were <18 years of age at the time of diagnosis. Cerebral sinovenous thrombosis was diagnosed based on the presence of an acute thrombotic cerebrovascular event that manifested as hemiplegia, aphasia, visual or balance disturbance, or seizures. In all patients, the clinical diagnosis of CSVT was confirmed via magnetic resonance imaging (MRI) and MR venography (Figure 1). The inclusion criteria were as follows: (1) age 0 (gestational age ≥38 weeks) to 18 years, (2) sudden onset of focal neurological deficits, convulsion, headache, and loss of consciousness (any of these clinical findings were sufficient for diagnosis), (3) neuroimaging (MRI and MR venography) findings of recent ischemia/infarct of venous distribution.

Case 8: imaging of magnetic resonances and 3-dimensional magnetic resonances venogram in the patient with nephrotic syndrome who is thrombosis of superior sagittal and transverse sinus.
All patients underwent an echocardiography and a hematological investigation that analyzed prothrombin time (PT) and partial thromboplastin time (PTT); fibrinogen, protein C, protein S, antithrombin III, lipoprotein(a), factor VIIIC (FVIII), factor IX (FIX), and homocysteine levels; and the presence of prothrombotic gene mutations (factor V G1691A [FV G1691A], prothrombin [PT G20210A], and methyl tetrahydrofolate reductase C677T [MTHFR C677T]). Blood samples obtained via peripheral venipuncture were collected into plastic tubes without any additives and into plastic tubes containing 1/10 by volume of 3.8% trisodium citrate. After centrifugation, the samples were stored at −70°C. For genetic analysis, venous blood was collected into sample tubes containing EDTA. The genotypes of FV G1691A, PT G20210A, and MTHFR C677T were determined via polymerase chain reaction and analysis of restriction fragments, as previously reported. 11 The study protocol was approved by the Ankara University Ethics Committee, and written informed consent was obtained from the parents of each patient prior to performing any procedures.
Levels of FVIII and FIX were measured using a 1-stage clotting assay, and the von Willebrand factor level was measured using an immunoturbidimetric assay. The FVIII and FIX levels were accepted as high if they were above the cutoff value of 150 IU/dL. Protein C and protein S levels were measured using commercially available enzyme-linked immunosorbent assay kits. The lipoprotein(a) level was measured using a particle-enhanced immunonephelometric assay (reference range: 0-30 ng/mL). Following 12-hour of fasting, blood samples were collected into tubes containing EDTA, and the homocysteine level was measured using an AxSYM homocysteine assay (Abbott, Wiesbaden, Germany).
Statistical Analysis
Data were statistically analyzed using SPSS v13.0 for Windows (SPSS, Inc, Chicago, Illinois). Data are presented as mean ± standard deviation. All categorical data were analyzed using the chi-square test or Fisher exact test. The level of statistical significance was set at P ≤ .05.
Results
In all, 5 girls (41.7%) and 7 boys (58.3%) with mean age of symptom onset of 5.2 ± 6.29 years (range: 0-18 years) were followed at our institution for a mean of 1.8 ± 1.73 years (range: 0-6.5 years). The neonatal group included 6 patients (50%), and the nonneonatal group included 6 patients (50%).
In the neonatal group, 1 patient (16.6%) presented with hemiparesis or hemiplegia, 1 patient (16.6%) with lethargy, and 6 patients (100%) with seizures; whereas in the nonneonatal groups, 2 patients (33.3%) presented with hemiparesis or hemiplegia, 2 patients (33.3%) showed cranial nerve involvement, 1 patient with seizures, 2 patients (33.3%) with vomiting, and 2 patients (33.3%) with headache. The patients in the neonatal group did not receive anticoagulation therapy, whereas most of the nonneonatal group patients (66.6%) did. The underlying diseases of the neonatal patients included hypernatremic dehydration in 2 patients, intracranial hemorrhage in 3 patients, and protein S deficiency in 1 patient. For the neonatal patients, hydrocephalus occurred in 2 patients and mental–motor retardation occurred in 1 patient. In all, 1 patient died during the neonatal period.
The underlying diseases of the nonneonatal patients included Behçet disease in 2 patients, nephritic syndrome in 1 patient, and B12 deficiency related to megaloblastic anemia in 1 patient. Hemiparesis occurred in 2 of the nonneonatal patients. Recurrence was not observed in any of the nonneonatal patients.
The frequency of prothrombin gene 20210 G/A and FV 1691G-A mutation carriers in the Turkish population was reported to be 2.7% and 7.9%, respectively. 12,13 In this study cohort, 2 patients had the heterozygous factor V Leiden (FVL) mutation (16.6%), 2 had the MTHFR homozygous mutation (16.6%), 1 had the PT G20210A mutation (8.3%), and 1 had the MTHFR heterozygous mutation (8.3%). The comparison of the prothrombin gene alleles found in the normal population to those in the patients with CSVT is shown in Table 1.
Comparison of the Normal Population With Patients With CSVT in Terms of Frequency of Prothrombin Gene 20210 G/A and Factor V 1691 G-A Mutation Carriers.
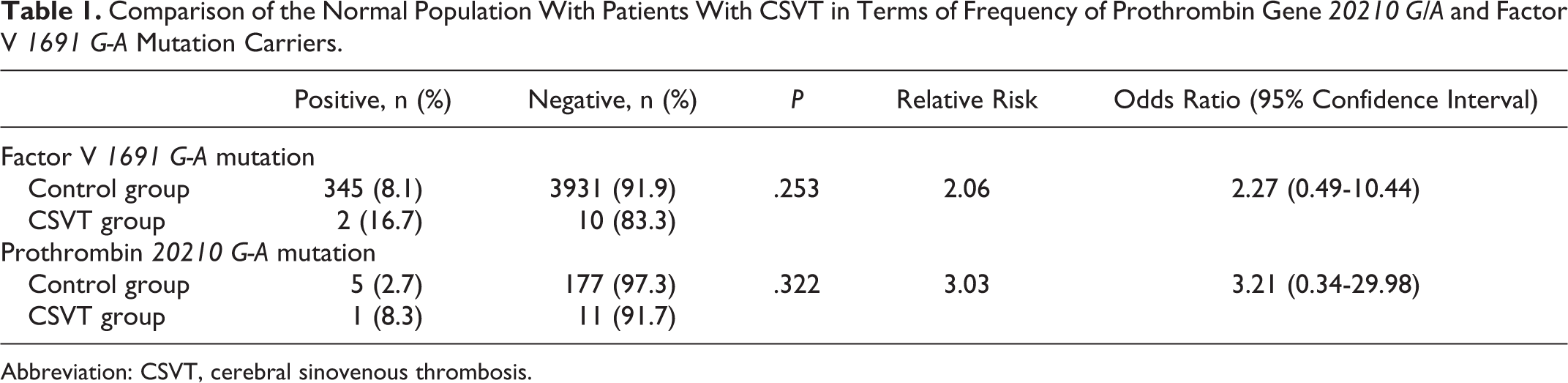
Abbreviation: CSVT, cerebral sinovenous thrombosis.
In total, 3 patients had no risk factors, 2 patients had 1 risk factor, and 7 patients had multiple risk factors. The overall distribution of the prothrombotic risk factors and underlying clinical diagnoses are shown in Table 2. Among the patients in this study, 4 received anticoagulant therapy. The patients who received anticoagulant therapy did not experience complications. Neurological sequelae were observed in 1 (25%) of the 4 patients given anticoagulant therapy, versus 4 (50%) of the 8 patients who did not receive anticoagulant therapy. Additionally, 1 (12.5%) patient who was not given anticoagulant therapy died (Table 3).
Clinic Summaries of the Neonatal Patients With CSVT.
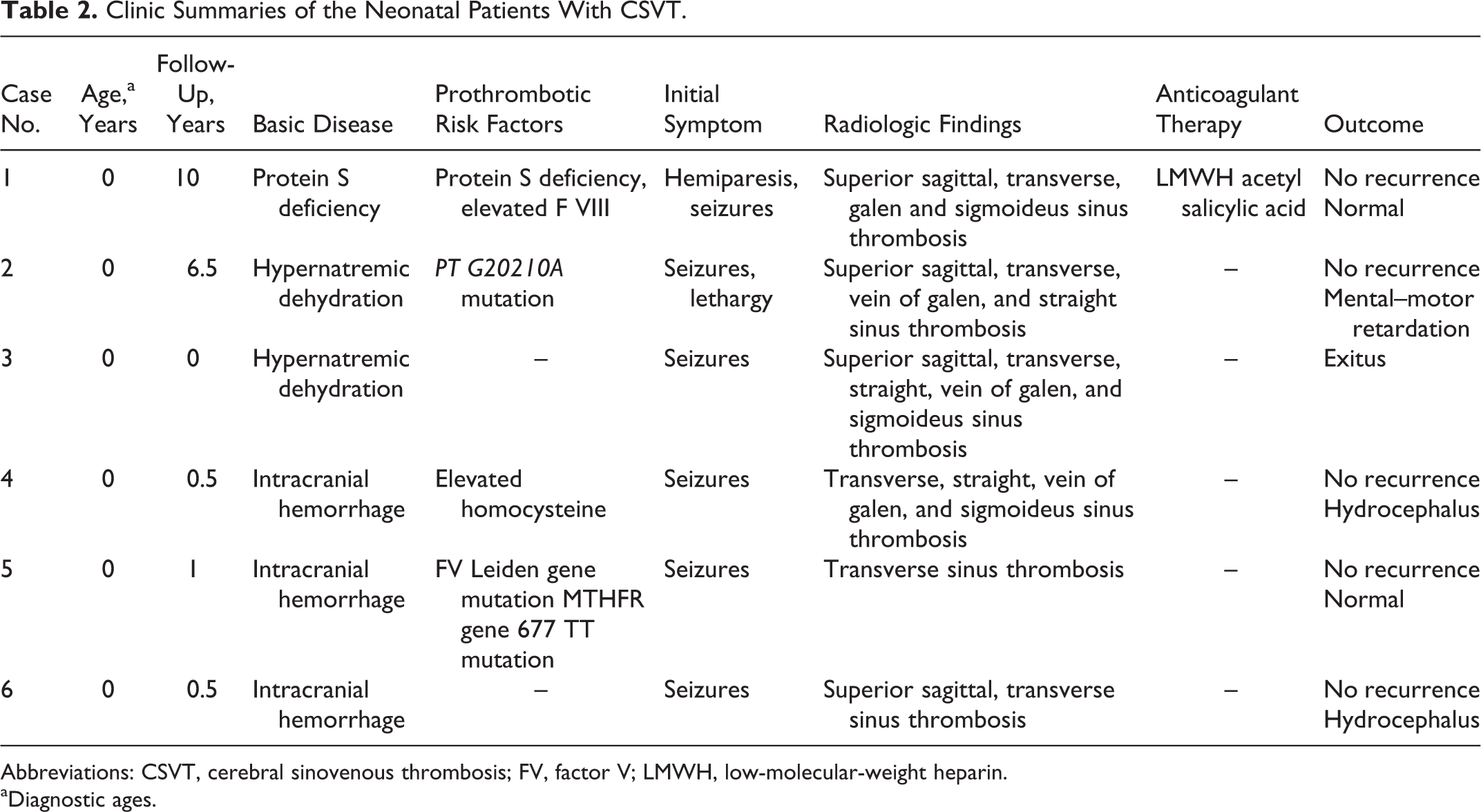
Abbreviations: CSVT, cerebral sinovenous thrombosis; FV, factor V; LMWH, low-molecular-weight heparin.
aDiagnostic ages.
Clinic Summaries of the Nonneonatal Patients With CSVT.
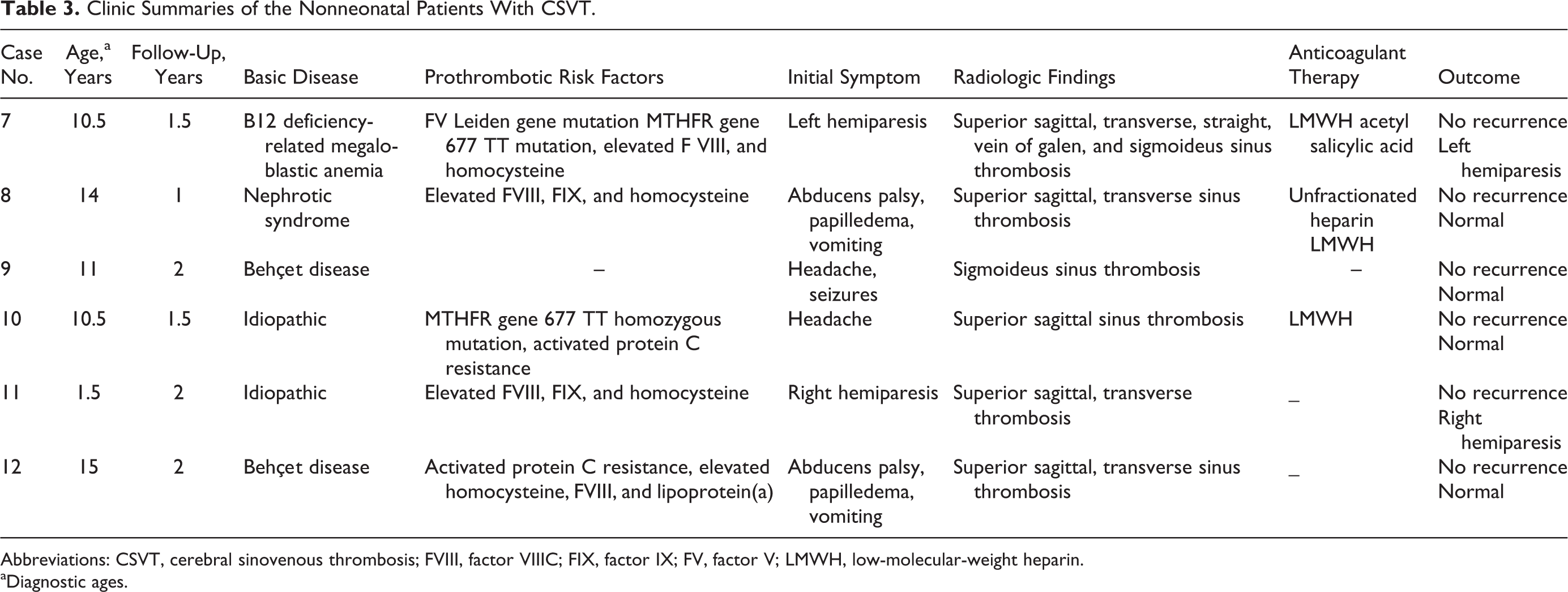
Abbreviations: CSVT, cerebral sinovenous thrombosis; FVIII, factor VIIIC; FIX, factor IX; FV, factor V; LMWH, low-molecular-weight heparin.
aDiagnostic ages.
Anticoagulant Therapy Usage
Acute treatment
Low-molecular-weight heparin (LMWH) was given twice daily and adjusted to achieve an antifactor Xa (anti-FXa) level of 0.5 to 1.0 U/mL or unfractionated heparin for 3 to 5 days adjusted to achieve an anti-FXa of 0.35 to 0.7 U/mL or a corresponding activated PTT range, followed by LMWH. Total duration of acute anticoagulation treatment was 3 months.
Prophylactic treatment
Prophylaxis was given to patients especially with children who were carrying prothrombotic risk factors (2 ≥). Acetyl salicylic acid given was between 1 and 3 mg/kg body weight per/d.
Discussion
The incidence of childhood CSVT varies between 0.25 and 0.67 per 100 000 children annually. 1 –4 Recent data from the International Pediatric Stroke Study showed that >50% of all patients with CSVT diagnosed during infancy and childhood occur in newborn infants aged between 0 and 28 days. 1,14 In the present study, 50% of the patients were neonates, which is in accordance with the literature. In addition, more boys than girls were affected, as previously reported. 15 –17
Wu et al first pointed out that CSVT should always be considered in the presence of an intraventricular hemorrhage occurring during the neonatal period, especially when this is associated with a unilateral thalamic hemorrhage. 18 In their studies, 31% of term neonates who were diagnosed with CSVT presented with an intraventricular hemorrhage. Additionally thalamic hemorrhage was detected in 16% of term neonates. 18 One of three patients with intracranial hemorrhage in our study presented with unilateral thalamic hemorrhage and parietal lobe hemorrhage was present in 2 patients. Small parenchymal brain lesions were detected in our patients. Intracranial hemorrhage in the our patients may be a result of increased venous pressure and cerebral edema due to sinovenous thrombosis.
The best treatment strategy for neonatal CSVT is controversial, and the clinical outcomes vary widely. The treatment of neonates with CSVT was not specifically addressed in the United Kingdom Royal College of Physicians guidelines. 19 The American College of Chest Physicians guidelines suggest initiating treatment with anticoagulation in neonates without large ischemic and hemorrhagic infarction or intracerebral hemorrhage and provide radiographic monitoring of such children with the recommendation to initiate anticoagulation if the extension of thrombosis occurs. 20 The American Heart Association's recommendations are to provide supportive therapy for dehydration, infection, seizures, and raised intracranial pressure and consider anticoagulation only in selected neonates with clinical or radiological evidence of propagating CSVT despite supportive therapy. 21
According to several researchers, neonates with CSVT do not require routine antithrombotic treatment because they have a negligible risk of recurrence. 22 Additionally, the high frequency of spontaneous intracranial hemorrhage associated with neonatal CSVT underlies the concern about anticoagulant treatment 14,15 ; however, new data suggest that anticoagulant treatment in cases of neonatal CSVT is safe, 14 perhaps even in the presence of intracranial hemorrhage. 23 Except for 1 neonatal patient, the others were given anticoagulant therapy in the present study. Low-molecular-weight heparin was only given to the patient with protein S deficiency. In addition, this patient was given acetyl salicylic acid for prophylaxis. Complications and neurological sequelae were not observed in this patient. In the present study, 2 patients recovered fully, 1 died during the acute phase, 2 developed hydrocephalus, and 1 developed mental–motor retardation during the follow-up period. That is, 80% (4 of 5) of the newborn patients who did not receive anticoagulant therapy either experienced exitus or had neurologic sequelae.
Prothrombotic states may cause or contribute to sinovenous thrombosis in both neonates and older children. The G20210A prothrombin gene mutation and the presence of FVL are the most common genetic disorders reported in patients with CVST. 1,24 In adult patients, it seems that the risk of CSVT is as much as 5-fold higher in patients with FVL and as much as 10-fold higher in patients with the G20210A prothrombin gene mutation than for the normal population. 25 The comparison of the genetic profile of a normal population and patients with CSVT in the present study showed that FVL increased the risk of CVST by 2-fold, and G20210A prothrombin increased it 3-fold.
In children with sinovenous thrombosis, the frequency of prothrombotic disorders—both acquired and congenital—can be as high as 50%; often, FVL and G20210A prothrombin are the most common congenital disorders, and antiphospholipid syndrome is the most common acquired disorder. 3 Whether genetic or acquired prothrombotic disorders can cause sinovenous thrombosis in children or are merely associated with sinovenous thrombosis remains unclear. Many researchers in the field of hematology advise caution in assigning thrombophilia with venous thrombosis as a causative factor unless the patient presents with a double genetic defect. 26 In any case, identification of new gene polymorphisms in the coagulation and fibrinolytic systems, their role in venous thrombosis, and their interaction with exogenous risk factors will continue to be a research challenge. The rate of recurrence of CSVT in neonates is not well known; in pediatric patients, it seems that deep venous thrombosis is more likely to recur during puberty. 26
For nonneonates having CSVT without evidence of hemorrhage, there is an agreement among 3 important guidelines to treat nonneonates with anticoagulation until the affected venous channels are completely recanalized or up to a maximum 6 months. 19 –21 While the American Heart Association suggests initial unfractionated heparin or LMWH followed with warfarin for 3 to 6 months, 21 the American College of Chest Physicians suggests initial unfractionated heparin or LMWH, followed by LMWH for 3 months. If the vessel isn’t fully recanalized, it is recommended that therapy is continued for another 3 months. 20 The Royal College of Physicians recommends initial therapy with acetyl salicylic acid. 19 None of the guidelines have recommendations for secondary prevention of CSVT. 19 –21 Initially, we preferred initial unfractioned heparin or LMWH for nonneonatal patients, and with LMWH, we completed the treatment in 3 months. In our study, neurologic sequelae were seen both in the patient who was given treatment and in the ones who weren’t given treatment. A multiple prothrombotic risk factor was observed in those patients who received treatment. We used acetyl salicylic acid as a seconder precaution only to those patients who had multiple prothrombotic risk factor. There wasn’t seen any recurrence. We think that it will be useful if acetyl salicylic acid is given to the patients having the multiple prothrombotic risk factor in order to prevent the recurrence.
In the present study, only 1 patient had 2 prothrombotic risk factors, but he also had megaloblastic anemia. Prothrombotic factors in the present study’s patients were used as a guide for prophylactic treatment, and those that received the treatment did not experience recurrence. The patients’ clinical findings were important for the acute treatment decision. Low-molecular-weight heparin was used in the present study for acute treatment, as many previous studies have reported that LMWH therapy in children with CSVT was not associated with complications; there were no major complications in our patients. 27,28
In conclusion, we presented our findings for a series of pediatric patients with CSVT. The patients were similar, in terms of initial symptoms, age, sex, and radiological findings, to those examined in earlier studies. Anticoagulant therapy was given to 33% of the patients, of which 25% had neurological sequelae; in contrast, 62.5% of the patients who did not receive anticoagulant therapy experienced either exitus or had neurologic sequelae. It has been previously reported that anticoagulation therapy for thrombosis in patients with CSVT did not negatively affect patient outcome, even in the presence of cerebral hemorrhage. 23 None of the patients in the present study experienced recurrence, but neurological sequelae were present because anticoagulant therapy wasn’t given during the acute phase. As such, we think that anticoagulant therapy should be given during the acute phase of CSVT unless the patient is experiencing major hemorrhage. Additionally, prophylaxis for the patients’ prothrombotic factors should be performed to prevent recurrence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.