
Abstract
The diagnosis of mild bleeding disorders is not easy as most of the “healthy” individuals also report bleeding symptoms. In order to get a precise bleeding history, Pediatric Bleeding Questionnaire (PBQ) has been developed. In our study, Turkish children diagnosed with Von Willebrand disease (VWD), platelet function defect (PFD), and healthy children without any symptoms (control group 1) and healthy children with symptoms but found hemostatically normal (control group 2) were analyzed with PBQ. The cut off level for “positive bleeding score” was found to be ≥2 (area under the curve [AUC]: 0.785, 95% confidence interval [CI]: 0.718-0.852). The sensitivity, specificity, positive predictive value, and negative predictive value of PBQ to define VWD versus control group 1 was 100%, 97.4%, 96.4%, and 100%; VWD versus control group 2 was 100%, 53.1%, 64.3%, and 100%; PFD versus control group 1 was 93.3%, 53.1%, 73.7%, and 85%; and PFD versus control group 2 was 93.3%, 53.1%, 73.7%, and 85%, respectively.
Introduction
An accurate bleeding history is crucial for diagnostic evaluation of suspected bleeding disorders and to predict bleeding risk. However, it is difficult to distinguish significant bleedings from trivial bleedings, which is common in healthy individuals in general population. Mild Von Willebrand disease (VWD) is the most common bleeding disorder occurring approximately 1% in general population. Apart from rare platelet function disorders (PFDs) such as Glanzmann thrombasthenia and Bernard-Soulier syndrome, which are characterized by severe bleeding tendency, there are a number of platelet function defects manifested by mild bleeding tendency and are believed to be prevalent in general population. Patients with these mild bleeding disorders often present with one or more mucocutaneous bleeding including easy bruising, epistaxis, heavy menstrual bleeding, and excessive bleedings after tooth extraction or superficial cuts. These bleeding symptoms are also reported by a 20% to 50% of healthy individuals in general population, making it difficult for the physician to decide on “excessive bleeding” before laboratory investigations and predict the bleeding risk. Moreover, reporting the severity of bleeding is influenced by feelings, education, and experience of the patient.
In order to overcome these difficulties, several bleeding questionnaires (BQs) have been developed for objective and precise quantification of bleeding symptoms and assessment of bleeding severity by a final bleeding score. In the European Molecular and Clinical Markers for the Diagnosis and Management of Type 1 VWD (MCMDM-1VWD) study, the BQ proposed by Rodeghiero et al has been modified for diagnosis of VWD. 1 A condensed form of this BQ has been evaluated by several investigators and found to be useful in the diagnosis of VWD with 100% sensitivity and 87% specificity. 2 The pediatric version of MCMDM-1VWD includes specific symptoms for children within the other category to collect a “lifelong” bleeding history and maintain it in a standardized manner. 3 The performance of Pediatric Bleeding Questionnaire (PBQ) has been tested in a few studies and the cut off level for a positive score has been reported as ≥2 for VWD and PFD. 2 –4 However, more studies are needed to determine the utility of PBQ in the diagnosis of VWD and PFD. The aim of this study was to investigate the clinical relevance of PBQ in VWD and PFD and to determine a “clinically significant” bleeding score cut off for our population to differentiate “hemostatically normal bleeders” and “children with mild bleeding disorders.”
Patient Study Population
This study included children (age < 18 years) with VWD (n = 46; 27 VWD type 1, 5 VWD type 2, and 14 VWD type 3) and children (age < 18 years) with PFD (n = 65; 7 Glanzmann thrombasthenia, 9 Bernard-Soulier syndrome, 4 Hermansky-Pudlak syndrome, and 45 platelet secretion defects [PSD]) who were followed up/or consecutively diagnosed in the Pediatric Hematology Unit of the Gazi University Medical School. Control group 1 consisted of (n = 38) healthy children without any bleeding symptoms. Children presented with bleeding symptoms but had normal prothrombin time, partial thromboplastin time, platelet function analyzer (PFA) 100, VWF:antigen (VWF:Ag), VWF:ristocetin cofactor (VWF:RCO) and platelet function tests served as control group 2 (n = 32). Children with VWD, PFD, and children in control group 2 were recruited from Gazi University Pediatric Hematology Department. Control group 1 consisted of children <18 years who were consulted to general pediatrics outpatient clinic for preoperative evaluation. Informed consent was obtained from parent/caregivers of all patients according to the latest version of Helsinki Declaration and the study was approved by the institutional review board of Gazi University Medical School.
Pediatric Bleeding Questionnaire Administration
The PBQ was administered face-to-face to 46 patients with VWD, 45 with PFD, and control groups by a pediatric hematology fellow (BB). The PBQs of 20 patients with PFD were gathered from historical but very well-organized hospital records and these patients were communicated via telephone interview. The pediatric hematologist was aware of their diagnoses but not the exact bleeding symptoms. Bleeding events were recorded before and after the diagnosis. All surgeries and hemostatic challenges (eg, tooth extraction) and prophylactic hemostatic therapies (if done) were recorded. The time to complete a PBQ was 20 to 25 minutes for face-to-face and 15 to 20 minutes for telephone administration. For accurate results, 1 independent observer also performed calculation of the total score with the pediatric hematologist who administered the questionnaire.
Laboratory Methods and Diagnostic Criteria
Historical laboratory results were used for the patient groups. Patients with VWD were diagnosed with VWF:Ag, VWF:RCO, Factor (F) VIII levels, platelet response to low-dose ristocetin (if required), and ABO blood group. The diagnostic criteria of type 1 VWD consisted of VWF:RCO and VWF:Ag levels between 0.5 and 50 IU/mL in at least 2 measurements, a VWF:RCO–VWF:Ag ratio >0.5, and positive family history of VWD. Type 2 and type 3 VWD diagnoses were made according to the criteria mentioned elsewhere. 5,6,8,9 Diagnosis of PFD was made with the use of complete blood count, blood smear, PFA-100 (including 10 mcg collagen/epinephrine and 50 mcg collagen/adenosine diphosphate as aggregants), and platelet aggregometer (Chrono-log 700 platelet aggregometer model 700; Chronolog Corporation, 2 West Park Road Havertown, PA, USA).
Statistical Analysis
Data analysis was performed using SPSS for Windows, version 11.5 (SPSS Inc, Chicago, Illinois). Mann Whitney U test was applied for comparisons of the median values between case and control groups. When more than 2 groups were compared, Kruskal Wallis test was used. When Kruskal Wallis test statistics gave statistically significant results, Conover nonparametric multiple comparison test was used to know which group differed from the other. Nominal data were analyzed by Pearson chi-square, Fisher exact, or likelihood ratio test, where applicable. Degree of association between continuous variables was evaluated by Spearman correlation analysis. The optimal cut off points of bleeding score for discrimination of case and control groups from each other were evaluated by receiver–operator curve (ROC) analysis calculating area under the curve (AUC) as giving the maximum sum of sensitivity and specificity (ie, Youden index) for the significant test. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were also calculated at the best cut off point. A P value less than .05 was considered statistically significant.
Results
Characteristics of patient and control groups are shown in Table 1. The median scores are found to be 4 in VWD type 1, 7 in VWD type 2, 16 in VWD type 3, 9 in Glanzmann thrombasthenia, 10 in Bernard-Soulier syndrome, 7.5 in Hermansky-Pudlak syndrome, 4 in PSD, 0 in control group 1, and 1 in control group 2.
Patient and Control Groups.
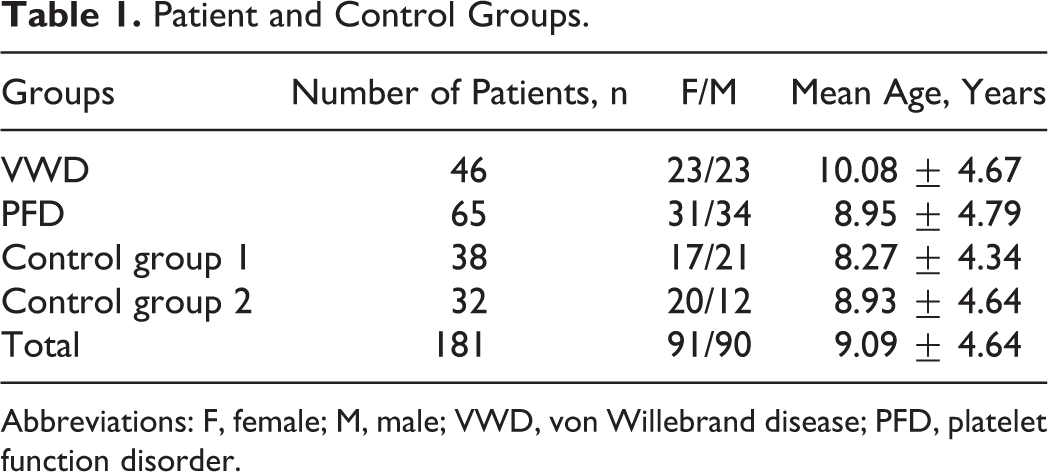
Abbreviations: F, female; M, male; VWD, von Willebrand disease; PFD, platelet function disorder.
The clinical significance for each bleeding symptom was assessed as ≥1 for menorrhagia, muscle hematoma, and hemarthrosis; ≥2 for epistaxis, bleeding from minor wounds, oral cavity, gastrointestinal (GI) system, tooth extraction, surgery, and pediatric-specific symptoms; and ≥3 for central nervous system (CNS) bleeding according to a previous study, 4 and the percentage of clinically significant scores among different groups were compared. The most frequent clinically significant bleeding symptoms that can differentiate VWD/PFD and control groups were found to be epistaxis, oral cavity bleeding, bleeding after tooth extraction, menorrhagia, and postcircumcision bleeding. The frequency of positive score for menorrhagia (≥1) was 97.1%, 20%, and 44% in menstruating females with VWD, control group 1, and control group 2, respectively, providing evidence that menorrhagia must be recognized as an important symptom suggesting bleeding disorder in menstruating females.
The cut off level for “clinically significant bleeding score” was found to be ≥2 (AUC 0.785, 95% confidence interval [CI] 0.718-0.852). The sensitivity, specificity, PPV, and NPV of PBQ to define VWD versus control group 1 was 100%, 97.4%, 96.4%, and 100%; VWD versus control group 2 was 100%, 53.1%, 64.3%, and 100%; PFD versus control group 1 was 93.3%, 53.1%, 73.7%, and 85%; and PFD versus control group 2 was 93.3%, 53.1%, 73.7%, and 85%, respectively (Table 2). An ROC analysis produced an AUC of 0.785 (95% CI 0.718-0.852; P < .05 against the null hypothesis that the true area is 0.5).
The Sensitivity, Specificity, Positive Predictive Value, and Negative Predictive Value of Pediatric Bleeding Score for Differentiation of Groups.
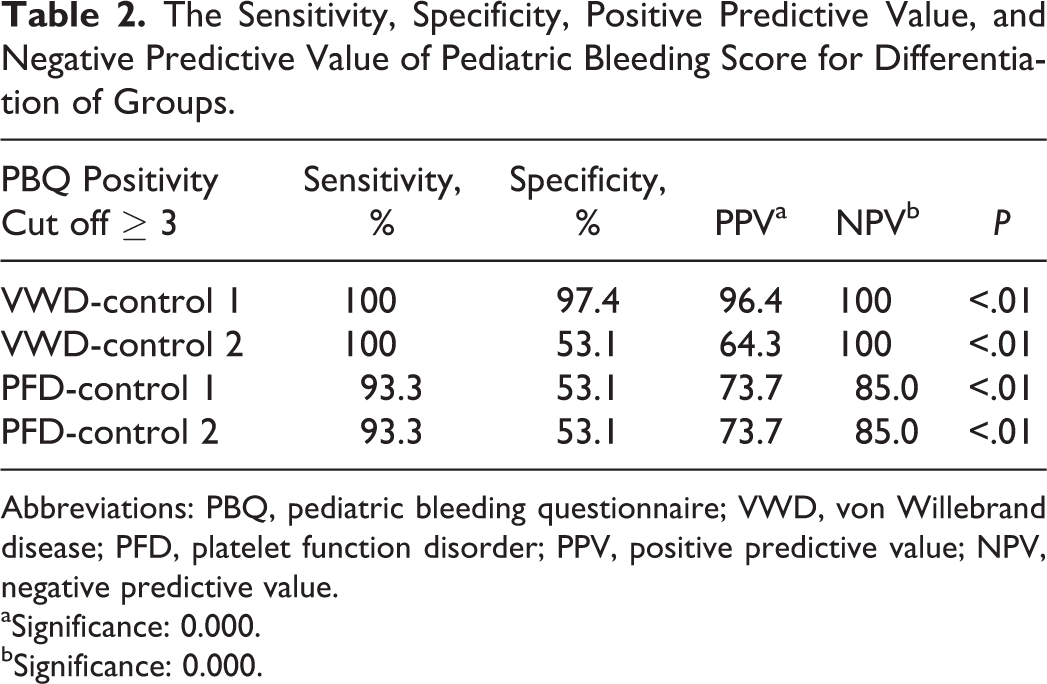
Abbreviations: PBQ, pediatric bleeding questionnaire; VWD, von Willebrand disease; PFD, platelet function disorder; PPV, positive predictive value; NPV, negative predictive value.
aSignificance: 0.000.
bSignificance: 0.000.
In VWD group, patients got a positive score of 60.9% (n = 28) for epistaxis, 34.8% (n = 16) for cutaneous bleeding, 39.1% (n = 18) for oral cavity bleeding, 6.5% (n = 3) for GI bleeding, 28.3% (n = 13) for bleeding after tooth extraction, 30.4% (n = 14) for surgical bleeding, 91.7% (n = 11) for menorrhagia (among menstruating females), 10.9% (n = 5) for muscle hematoma, 13% (n = 6) for hemarthrosis, 4.3% (n = 2) for CNS bleeding, and 36.4% (n = 8; among circumcised boys) for postcircumcision bleeding. There was no patient getting a positive score for conjunctival, umbilical, and postpartum bleeding in both VWD and PFD groups. Only 1 patient in the PFD group had a positive score for cephalhematoma. In the PFD group, the patients got a positive score of 67.7% (n = 44) for epistaxis, 58.5% (n = 38) for cutaneous bleeding, 27.7% (n = 18) for minor bleedings, 35.4% (n = 23) for oral cavity bleedings, 1.5% (n = 1) for oral cavity bleedings, 1.5% (n = 1) for GI bleedings, 13.8% (n = 9) for bleeding after tooth extraction, 6.2% (n = 4) for surgical bleedings, 76.5% (n = 13) for menorrhagia (among menstruating females), 24.1% (n = 29) for postcircumcision bleeding, and 1.5% (n = 1) for macroscopic hematuria and cephalhematoma. In the control group 1, clinically significant single symptom score was present only for 3 symptoms, with 2.6% (n = 1) for epistaxis, 20% (n = 1) for menorrhagia (among menstruating females), and 2.6% (n = 1) for postsurgical bleeding. In control group 2, in which differentiation between the normal individuals and the patients with bleeding was more challenging, 15.6% (n = 5) had a positive symptom for epistaxis, 9.4% (n = 3) for cutaneous bleeding, 3.1% (n = 1) for oral cavity bleeding, 6.3% (n = 2) for bleeding after tooth extraction, 44.4% (n = 4) for menorrhagia, and 3.1% (n = 1) for hemarthrosis. The total clinically significant score percentage (score ≥ 2) was 100% (n = 46) in VWD, 93.8% (n = 61) in PFD, 2.6% (n = 1) in control group 1, and 46.9% (n = 15) in control group 2 (Table 3), which showed that the BQ can help differentiating patients with bleeding and normal individuals.
Significantly Important Scores Among Patient and Control Groups.a
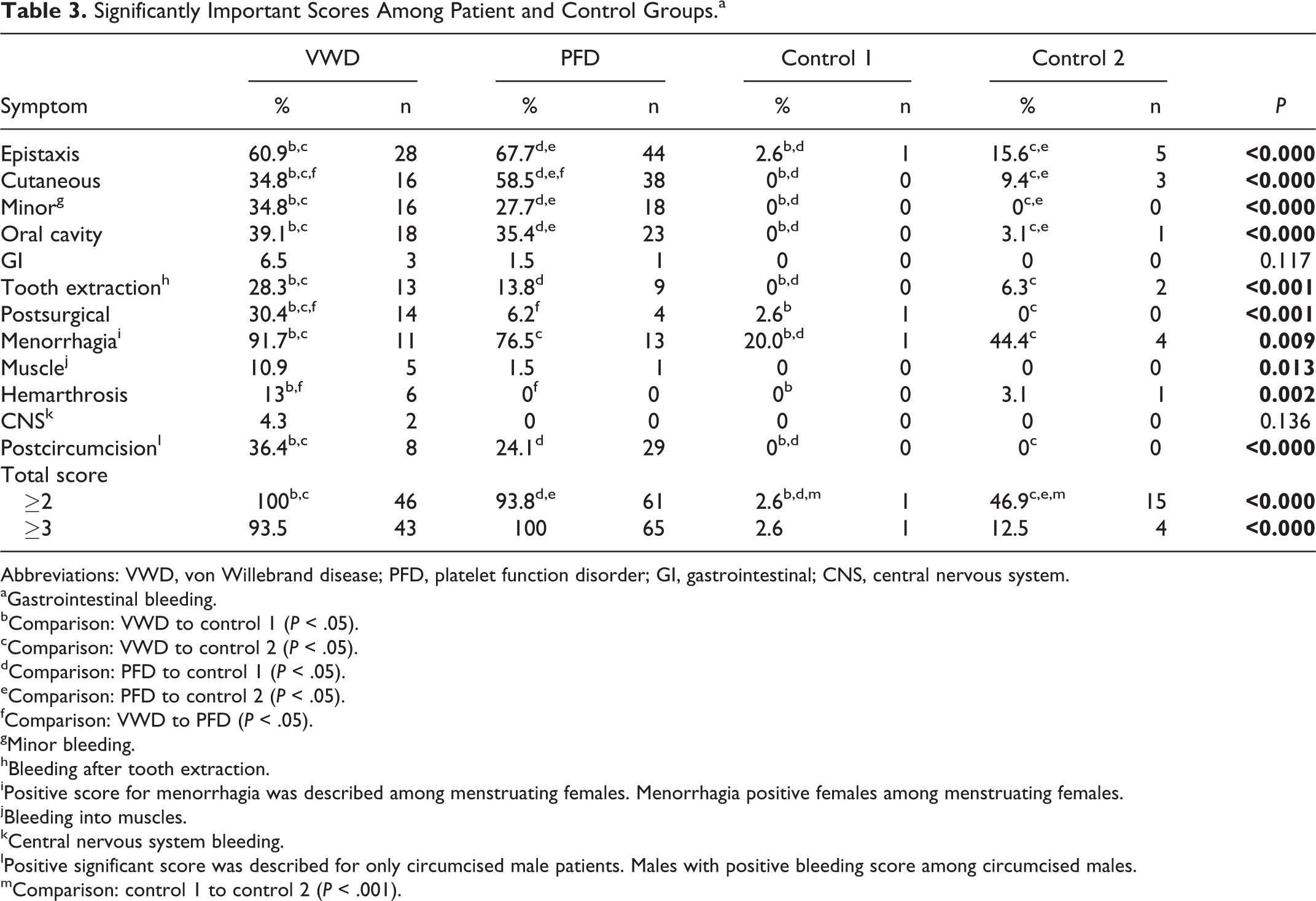
Abbreviations: VWD, von Willebrand disease; PFD, platelet function disorder; GI, gastrointestinal; CNS, central nervous system.
aGastrointestinal bleeding.
bComparison: VWD to control 1 (P < .05).
cComparison: VWD to control 2 (P < .05).
dComparison: PFD to control 1 (P < .05).
eComparison: PFD to control 2 (P < .05).
fComparison: VWD to PFD (P < .05).
gMinor bleeding.
hBleeding after tooth extraction.
iPositive score for menorrhagia was described among menstruating females. Menorrhagia positive females among menstruating females.
jBleeding into muscles.
kCentral nervous system bleeding.
lPositive significant score was described for only circumcised male patients. Males with positive bleeding score among circumcised males.
mComparison: control 1 to control 2 (P < .001).
Discussion
It is usually difficult to evaluate the hemorrhagic symptoms among children, especially in diagnosis of mild bleeding disorders such as VWD type 1 and PFD. Previously, the application of pediatric BQ in the determination of “normal” and “mild hemorrhagic disorders” has been studied and the total clinically significant bleeding score was found to be ≥2 in earlier reports. 2 –4
In this study, we tried to find out the cut off level among Turkish children. The cut off level of pediatric bleeding score was found to be ≥2 among our group of patients in consistence with previous studies. 4 The bleeding symptoms being most relevant in the diagnosis of VWD were found to be postoperative bleeding, bleeding after tooth extraction, and menorrhagia similar to the previous study by Biss et al. 6 However, the increased frequency of menorrhagia as a positive symptom in the hemostatically normal group (control group 2 has a menorrhagia frequency of 44%) suggested the need for additional laboratory tests in such patients. Bleeding after circumcision was found to be 36.4% in VWD group and 24.1% in PFD group in accordance with Biss et al as well. 6,7 In contrast to the previous studies, we did not observe any increase in total score with increasing age. 6 This may be attributed to the equalization of high scores among males due to postcircumcision bleeding and females due to menorrhagia. The heterogeneity of the patient group including both mild and serious bleeding disorders may have contributed to the bleeding tendency with increasing age as well. We analyzed both ≥2 (which is previously used as positive score cut off) and ≥3 as our own cut off value for the positive total score. The sensitivity, specificity, PPV, and NPV were found to be 93.5%, 87.5%, 91.5%, and 90.3%, respectively, in differential diagnosis of VWD and control group 2 when score cut off is ≥3. For the same groups, when score cut off was taken ≥2, the sensitivity, specificity, PPV, and NPV were found to be 100%, 53.1%, 64.3%, and 100% respectively. As our main aim was to find out the exact cut off point when NPV was 100% so that laboratory tests should not be proceeded if the child has a negative score as it would be very unlikely to have a mild bleeding disorder, we assumed the cut off level with 100% NPV should be encountered which is ≥2. Our findings were consistent with previous studies. 2 –7 We think that a cut off level of ≥2 should be suitable in our population in the differential diagnosis of “mild bleeding disorders” and “hemostatically normal patients with symptoms.”
Conclusion
In conclusion, PBQ was found to be useful in the diagnosis of VWD and PFD in Turkish children; however, to reach an exact diagnosis, hemostatic laboratory tests are still warranted. The most frequent symptoms associated with VWD/PFD were epistaxis, oral cavity bleeding, bleeding after tooth extraction, menorrhagia, and postcircumcision bleeding. We think that a cut off level of ≥2 is also suitable in our population in differential diagnosis of “mild bleeding disorders” and “hemostatically normal patients with symptoms.” In conclusion, the high NPV and ROC data show that PBQ can be used in advance to differentiate between VWD, PFD, and normal children.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.