
Abstract
Introduction:
Inferior vena cava filters (IVCF) are used liberally in clinical practice and have been associated with multiple complications. Herein, we present results from our institution.
Methods:
Records of consecutive patients discharged between January 1, 2009 and 2012 were reviewed. Indications were subcategorized under absolute, relative, and prophylactic. Student t test and Kaplan-Meier survival analysis were employed.
Results:
During this period, 254 vena cava filters (VCF) were placed. Of these, 65 were placed for absolute indication, 28 for relative, and 161 for prophylaxis. Follow-up imaging was available for 96 patients of which 15 showed complications. Successful retrieval of 19 filters was achieved.
Conclusion:
The study demonstrates that most IVCF are being placed for prophylaxis with low retrieval rate. This contradicts current recommendations. Moreover frequent migration and penetration of IVCF can lead to serious complications. Strict enforcement of IVCF placement guidelines and setting up of filter clinics for timely retrieval is suggested.
Keywords
Introduction
Pulmonary embolism (PE) is considered to be the most common preventable cause of deaths in hospitals accounting for approximately 10% of inpatient deaths. Even patients who survive the initial diagnosis of PE face a mortality rate of 17.5% at 90 days. 1 The PE remains a frequently missed diagnosis with high-associated morbidity and mortality 2,3 In this setting, since their introduction in 1970s, inferior vena cava filters (IVCFs) are being increasingly used in clinical practice to prevent PE. 4 Vena cava filters are of 2 types, permanent and nonpermanent. Nonpermanent filters are further divided into optional filters (which can be retrievable or convertible devices) or temporary filters (which must be removed as a result of their design constraints). 5
The American College of Chest Physicians (ACCP) recommends IVCF placement only in patients with proven venous thromboembolism (VTE) when primary therapy for VTE (anticoagulation) cannot be started, must be stopped, or is insufficient to protect patients from clinically significant PE. 5 –8
The IVCFs are in use for the last 4 decades, and their use has significantly increased since they were first introduced. In 2007, approximately 167 000 filters were implanted as compared to 2000 in 1979, and these numbers are expected to increase to 259 000 in 2012. 9 Although recurrent PE is unusual following filter insertion (2%-4% in most series), there is no strong evidence that IVCFs prevent death from PE. 10
Insertion of IVCF reduces but does not eliminate the risk of PE and increases the risk of deep vein thrombosis (DVT). Moreover, it does not affect the survival or overall frequency of VTE, 6,11 although it has been associated with procedural as well as long-term complications. In a 2010 report published by Food and Drug Administration (FDA), a total of 921 adverse events involving IVCF have been reported to the FDA since 2005. The FDA suspects that these events may be related to a retrievable filter remaining in the body for long periods of time, beyond the time when the risk of PE has subsided. 12
The FDA recommends that implanting physicians and clinicians responsible for the ongoing care of patients with retrievable IVCF consider removing the filter as soon as protection from clinically significant PE is no longer needed. 12 However, retrieval rate of IVCF is significantly low as shown in most studies (12%-45%). 13 It is reported in multiple studies that migration, perforation, fragmentation, fracture (with possible embolization), occlusion, and thrombosis are real risks. 14 The main reason for filter nonretrieval remains suboptimal follow-up and coordination of care after discharge. 15 Multiple approaches have been recently suggested in an attempt to improve the universally low current retrieval rates, including automatically scheduled follow-ups for all the patients who received a caval filter along with documentation of the anticipated estimate of duration of placement, with proactive strategies focused on contacting patients to ensure adequate follow-up. These approaches have shown variable improvements in the retrieval rates. 16,17
We conducted a retrospective review of practice at our institution to evaluate our current application of widely recommended guidelines of use of IVCF and to formulate a protocol for improved patient follow-up and IVCF retrieval rates.
Materials and Methods
Records of consecutive patients discharged from our institution (Saint Barnabas Hospital) between January 1, 2009 and 2012 with vena cava filter placement were reviewed. The inclusion criterion was the insertion of an IVCF as specified by appropriate Diagnosis-related group/International Classification of Diseases (DRG/ICD) 9 codes. The generated computerized list was evaluated for patient age, sex, race, comorbidities, admitting service, body mass index, IVCF inserting service, reasons for insertion, filter characteristics, retrieval, and complications based on the follow-up computed tomography (CT) scans. For purpose of avoiding confusion trauma, surgery and orthopedics were categorized under trauma surgery. A 2-tailed student t test was used for calculating P value, and Kaplan-Meier estimation was used for survival analysis. Patients were deemed as lost to follow-up if they had no contact per hospital charts for more than a year and have not died as per death registries.
Indications were subcategorized under absolute, relative, and prophylactic based on the current ACCP, Society of Interventional Radiology, and Eastern Association for the Surgery of Trauma (EAST) guidelines (Table 1). 5,18,19 Approval from institutional review board was obtained prior to the review. Unique codes were assigned to all patients. All data were stored in a secured computer with password protection and accessible only by the investigators.
Distribution of Indications Based on American College of Chest Physicians (ACCP), Society of Interventional Radiology (SIR), and Eastern Association for the Surgery of Trauma (EAST) Guidelines.
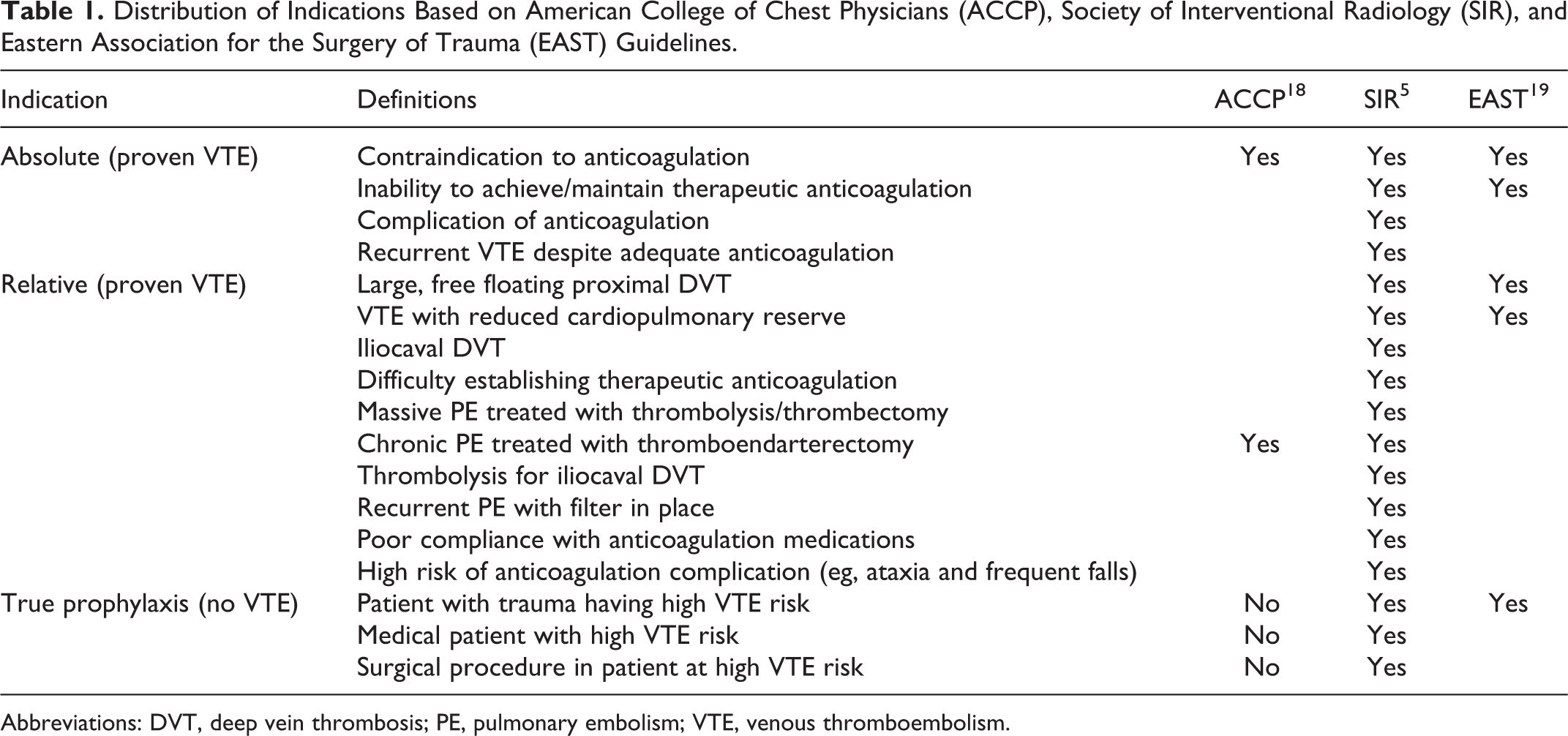
Abbreviations: DVT, deep vein thrombosis; PE, pulmonary embolism; VTE, venous thromboembolism.
Results
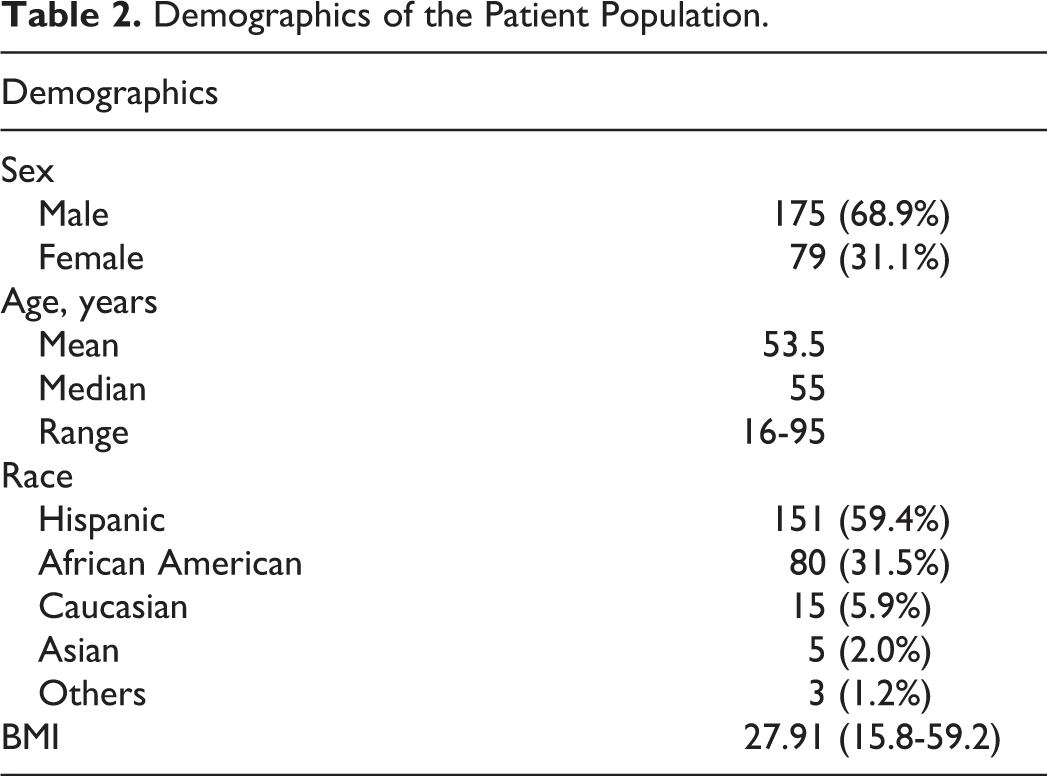
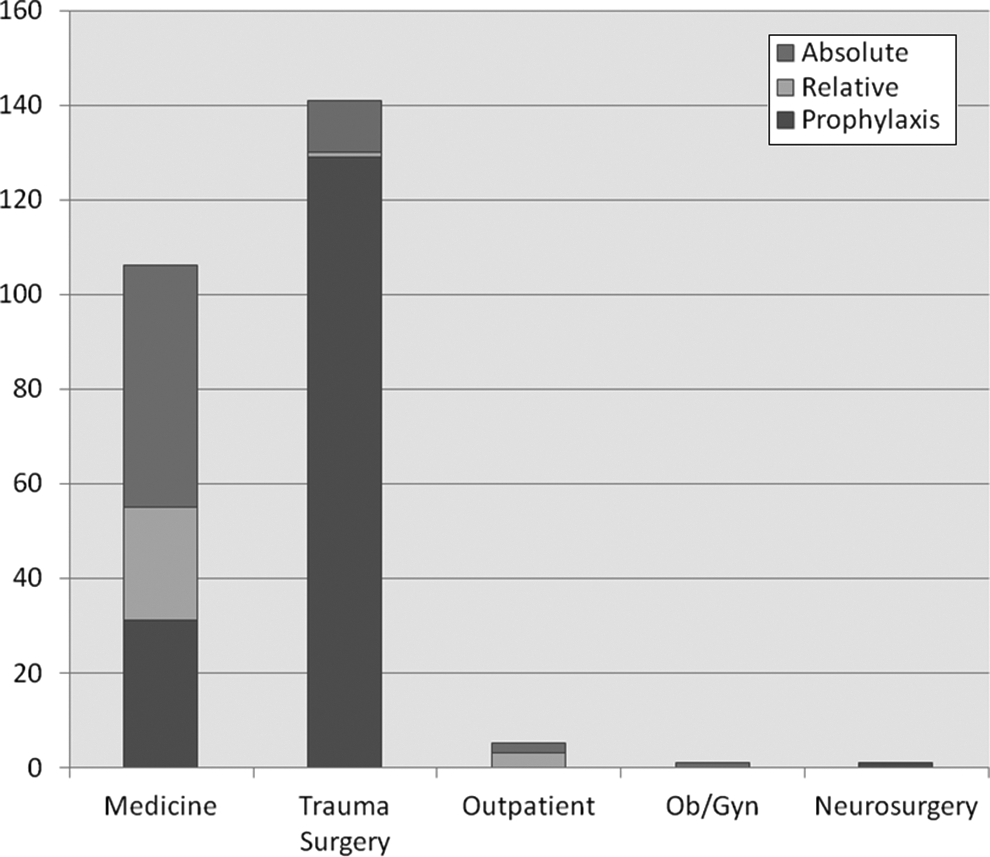
During this period 254 VCF were placed of which 249 were placed as inpatient and 5 were placed as outpatient. All but 1 filter were placed below the level of renal veins. Racial, age, and gender distribution are presented in Table 2 and Figure 1. Of the 254 patients, 141 patients were admitted under trauma surgery, 106 under medicine, 1 under neurosurgery, and 1 under obstetrics and gynecology. Median age at filter placement was 55 years (range 16-95 years; Table 3).
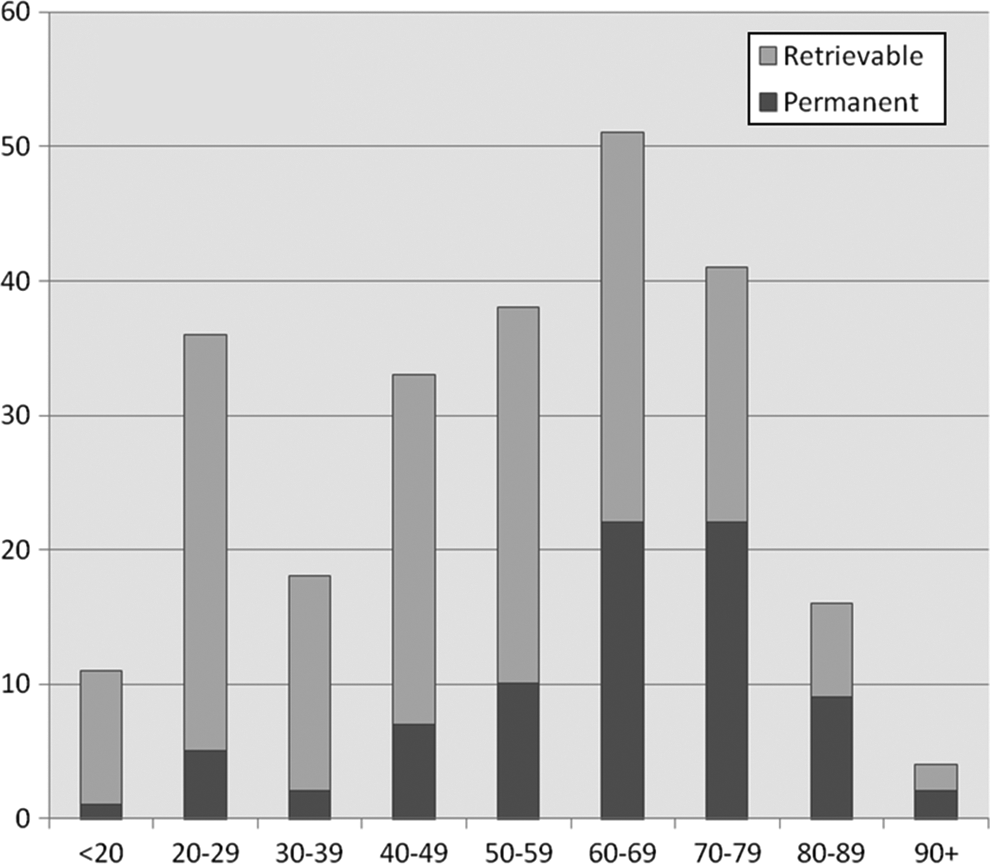
Proportion of retrievable to permanent filters in various age groups.
Demographics of the Patient Population.
Patient Distribution.
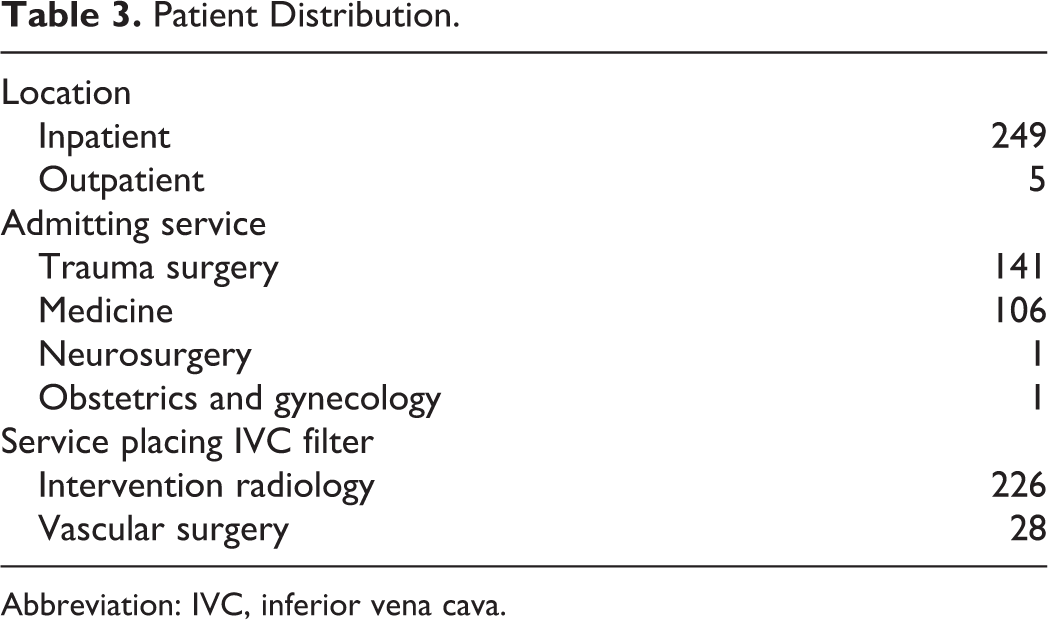
Abbreviation: IVC, inferior vena cava.
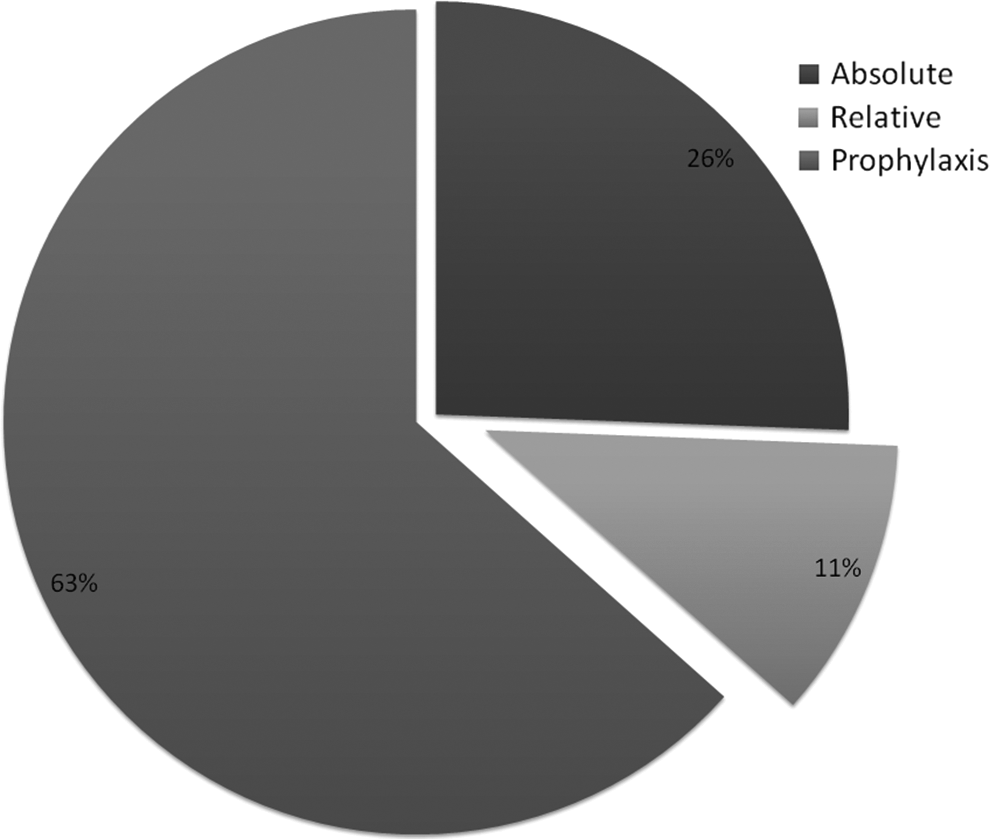
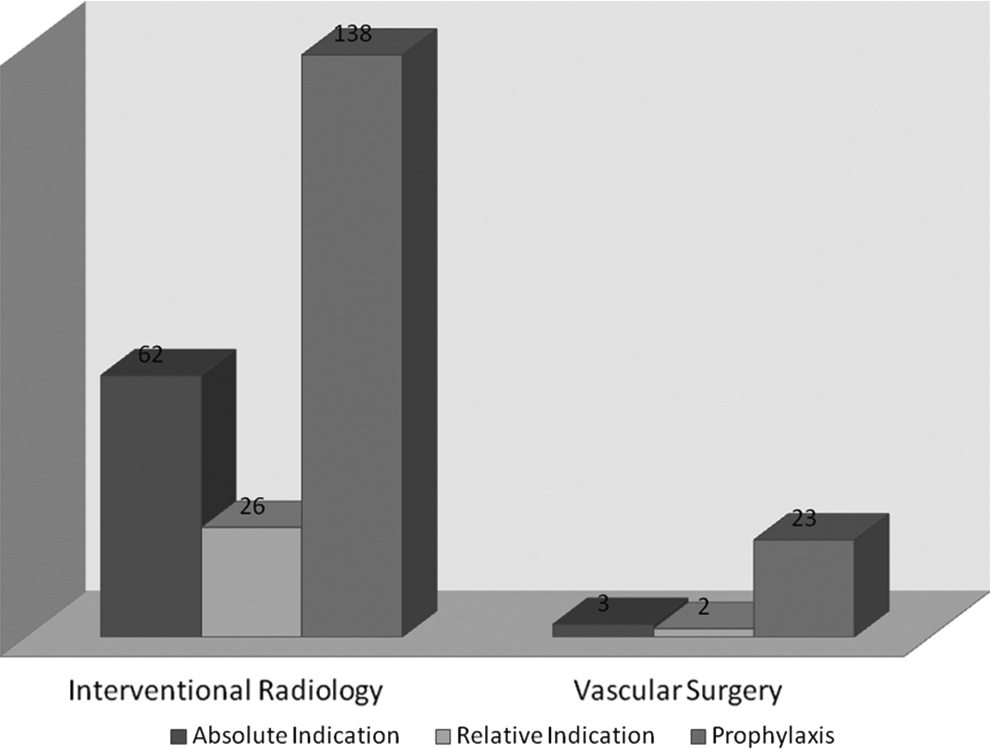
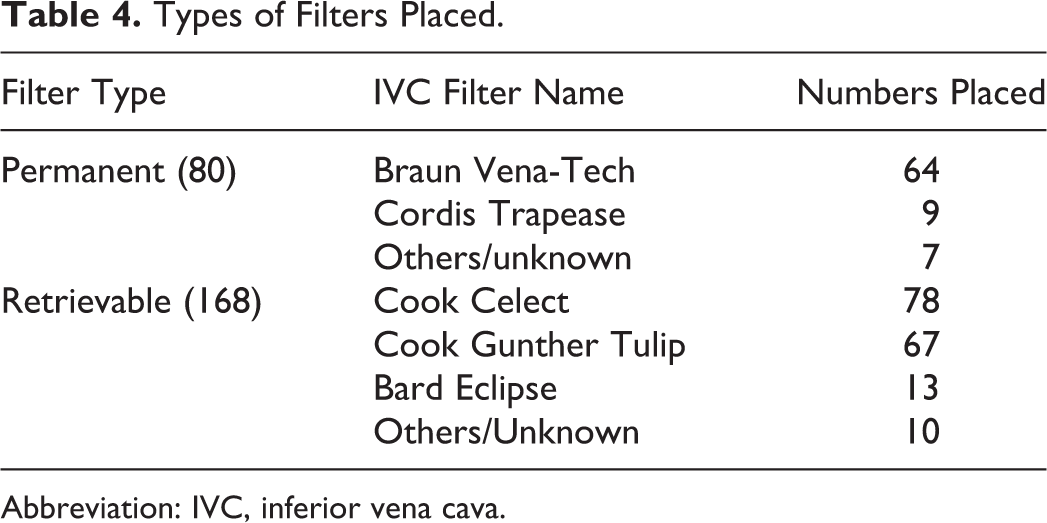
Interventional radiology placed 226 (89%) and vascular surgery placed 28 (11%) IVCFs (Table 3). Of the IVCFs, 65 (25.6%) were placed for an absolute indication, 28 (11%) for a relative one, and 161 (63.4%) for prophylaxis (Figures 2 –4). Overall, 80 VCF were permanent, 168 retrievable, and 6 filters had no documentation of retrievability type (Table 4). Vena-Tech (B Braun Medical Inc, Bethlehem, PA, USA) (80%) was the most commonly placed permanent filter, and Cook Celect (Cook Medical, Bloomington, IN, USA) (46.4%) and Cook Gunther Tulip (Cook Medical, Bloomington, IN, USA) (39.9%) were the most commonly placed retrievable filters. Of the 161 filters placed for prophylaxis, trauma surgery placed 129 VCF as compared to 31 by medicine (80.1% vs 19.3%, P < .001).
Number of filters placed per admitting service and categorization as per indications.
Overall placement indications.
Distribution of indications of filter insertion as per placement service.
Types of Filters Placed.
Abbreviation: IVC, inferior vena cava.
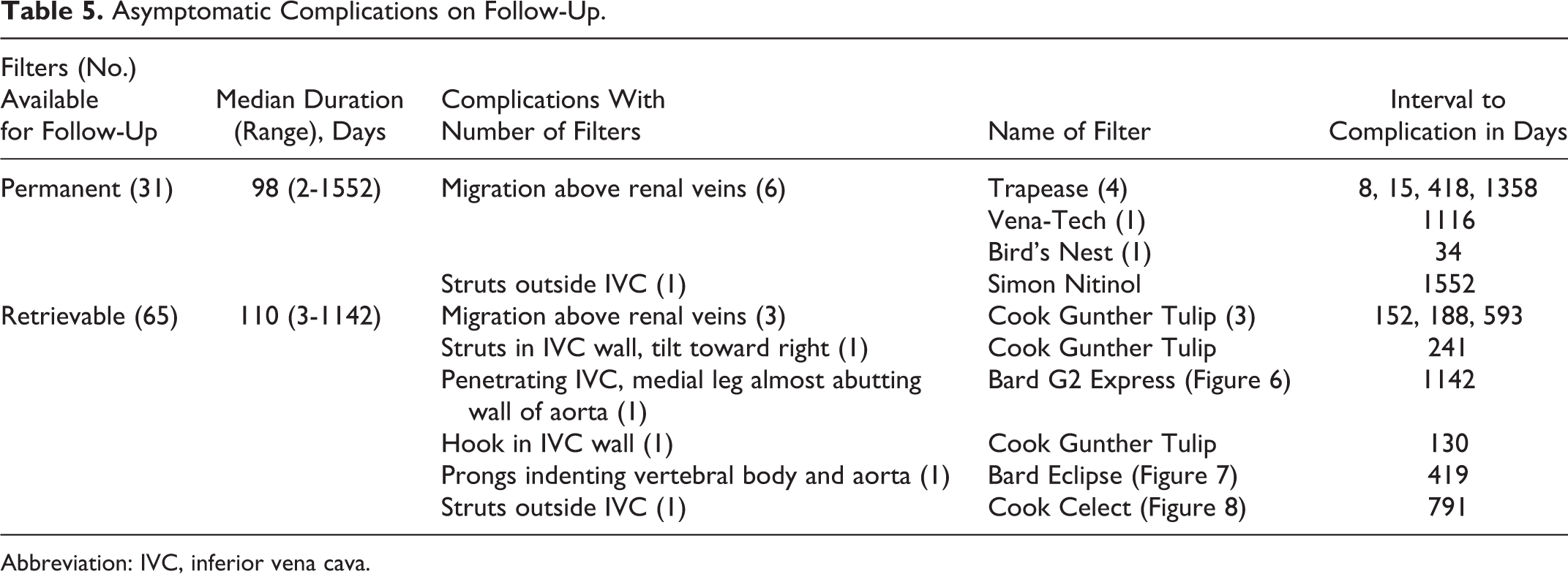
After IVCF placement, 96 patients had CT scans for various unrelated reasons which were analyzed to elucidate information regarding filters. The median follow-up for CT scans was 108.5 days (range 2-1552 days). Asymptomatic migration above renal veins in 9 (6 permanent and 3 retrievable) and limb or hook penetration in or outside IVC in 6 (1 permanent and 5 retrievable) patients were observed (Table 5; Figures 5–7). Due to asymptomatic nature of the findings, no intervention was done.
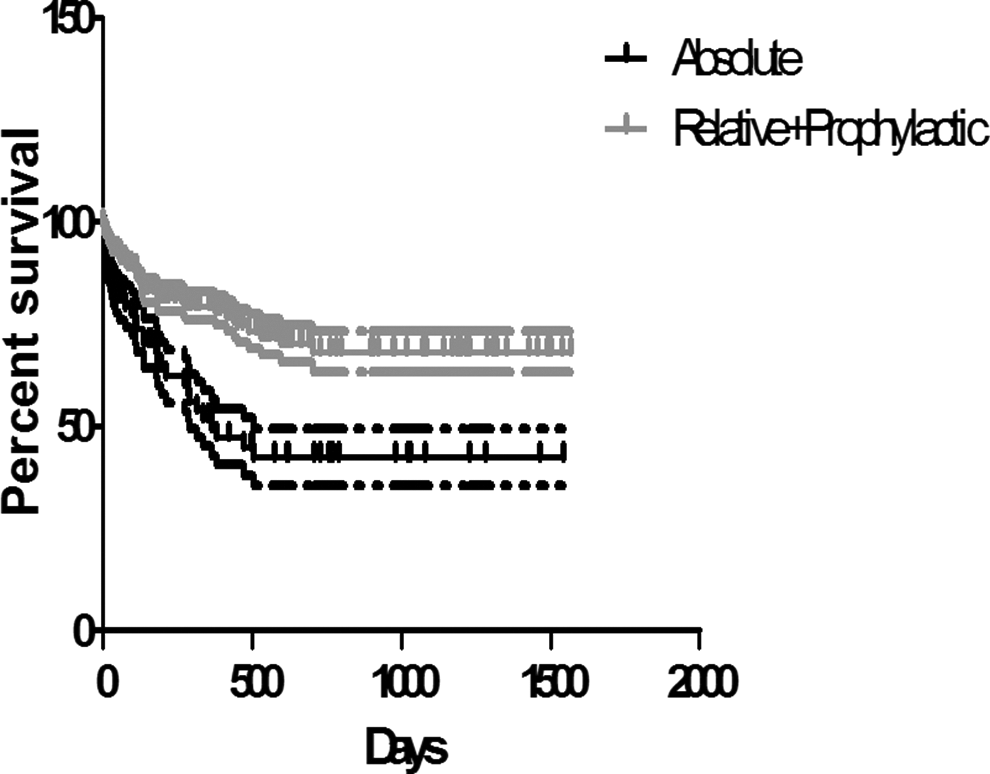
Kaplan-Meier analysis of patients with absolute indications as compared to relative and prophylactic indications.
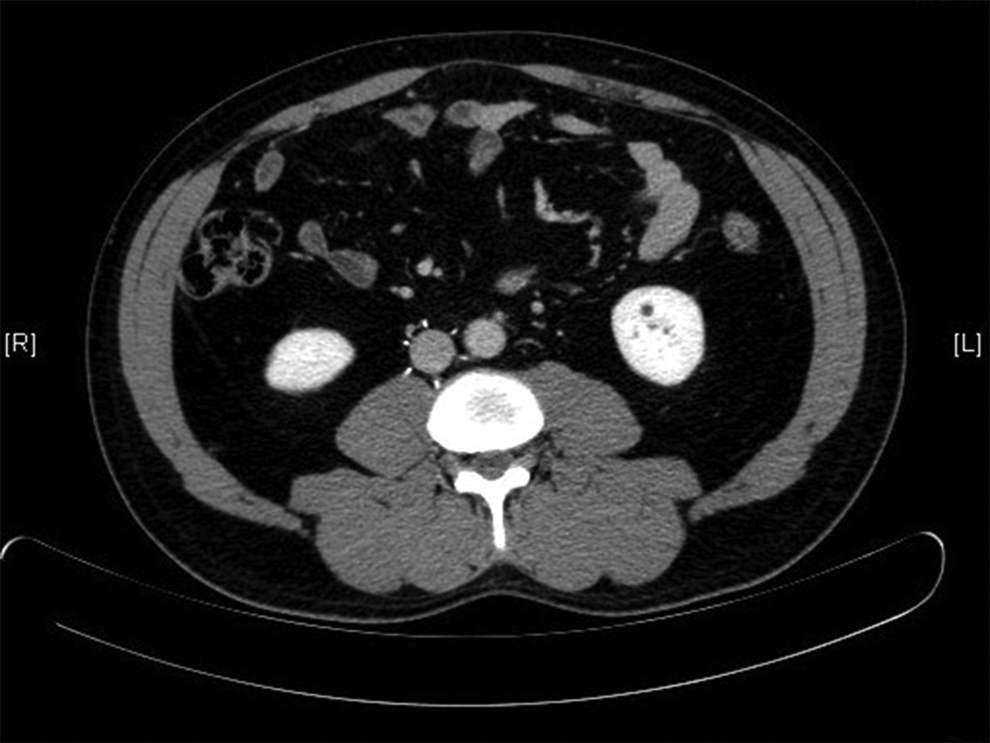
Bard G2 express filter penetrating inferior vena cava with medial leg almost abutting wall of aorta.

Bard eclipse filter with prongs indenting vertebral body and aorta.
Asymptomatic Complications on Follow-Up.
Abbreviation: IVC, inferior vena cava.
Successful retrieval of 19 (11.3%) filters without any significant complication was achieved by Interventional Radiology at a median of 122 days (range 7-1142 days). Of the retrieved filters, 14 were Cook Celect, 4 were Gunther Tulip, and 1 was Bard G2 Express filter (Bard Peripheral Vascular, Tempe, AZ, USA). Asymptomatic snare fracture during retrieval of a Cook Celect filter was encountered during retrieval in 1 case. No failed attempt was encountered during the procedures. Patients who had filter retrieval were significantly younger as compared to patients who did not have filter retrieval (median age at filter placement 32 vs 51 years, P < .006). On searching the death registries, 68 (26.8%) patients were found to be dead during course the of the study, and 80 (47.6%) patients with retrievable filters were deemed lost to follow-up.
Kaplan-Meier survival analysis showed a significant median survival difference between patients with absolute indication of IVCF placement as compared to patients with relative and prophylactic indications (365 days vs undefined, 95% confidence interval [CI] 1.559-4.589, P = .0004, hazard ratio 2.675; Figure 8). This indicates that the patients with no absolute indication for IVCF placement are probably less sick, leading to longer survival, and thus are more prone to long term of IVCF complications like migration, penetration, and so on.
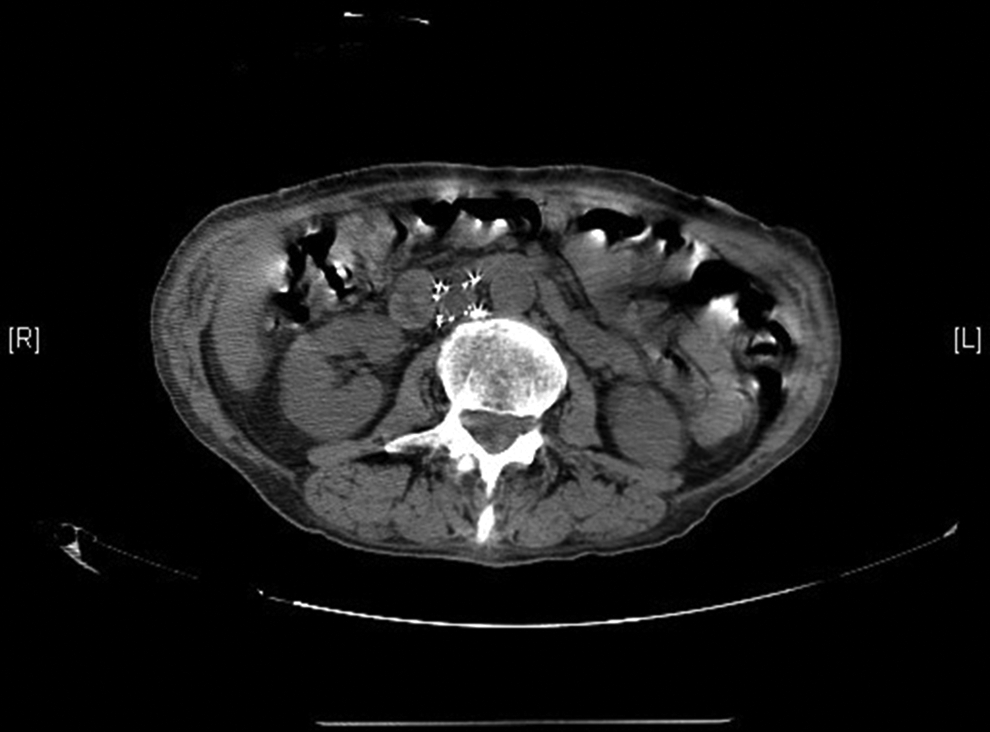
Cook Celect filter with struts outside inferior vena cava.
Discussion
The IVCFs are in use since last 4 decades, and there is tremendous increase in their usage since their introduction. Data show that in 2007 approximately 167 000 filters were implanted as compared to 2000 in 1979, and their number is expected to rise to 259 000 in 2012. 9
Although recurrent PE is unusual following filter insertion (2%-4% in most series), there is no strong evidence that IVCFs prevent death from PE. 10
Several studies on the effectiveness of IVCF filters have been conducted in the past. In one of the largest randomized trials to date, 400 patients with proximal deep venous thrombosis were assigned to either standard anticoagulation alone or anticoagulation with IVCF. Significantly fewer patients in the IVCF group had PE during the first 12 days after randomization (1% vs 5%). However, no significant differences in survival or rates of symptomatic PE between the 2 groups were revealed after a 2-year follow-up period. A significantly higher rate of recurrent deep venous thrombosis was observed among IVCF group (21% vs 12%). 20
In a second report after 8 years of follow-up on the same population, the overall incidence of VTE was similar among patients with and without IVCF (36% vs 35%, respectively), and patients with filters were more likely to experience DVT (35% vs 27%) but less likely to experience a symptomatic PE (6% vs 15%). The overall mortality and incidence of postthrombotic syndrome were similar in both the groups. 11
A 2011 analysis of the National Trauma Bank 21 revealed substantial nationwide variations in IVCF placement. The north east region was found to have the highest filter placement rate per patient (median 2.6; interquartile range [IQR] 1.2-5.9), whereas the west was found to have the lowest rate (median 0.44; IQR 0.14-1.2; P < .001). This variation could not be explained by patient or center characteristics and may represent differences in regional culture, market pressures, and funding and reimbursement patterns. 21
Also, prior institutional experiences do not favor IVCF placement outside the guidelines. In a single-center retrospective study, only 5% of the 196 patients who received IVCF outside the guidelines developed VTE implying that the rest (95%) might not have required an IVCF. 22 Similarly, in another retrospective study comparing clinical outcomes of patients with VTE who were treated with anticoagulation and filter versus anticoagulation alone, no differences in outcome measures of new PE, recurrent DVT, or mortality were observed after stratification according to the history of PE or VTE prior to the index VTE event. This again suggests that IVCF may not provide any substantial additional benefit for patients who can tolerate anticoagulation. 23
The Cochrane Peripheral Vascular Diseases Group reviewed 2 randomized studies involving 529 patients. 24 The first study involving 129 patients with hip fractures 25 showed a reduction in PE rates in the filter group as compared to the control group (4 of 41 vs 19 of 59, relative risk [RR] 0.3, 95% CI 0.11-0.82). However, mortality benefit was not statistically significant (4 of 41 vs 14 of 59 RR 0.41, 95% CI 0.15-1.16). The study was itself subject to significant biases due to inadequate randomization, unblended outcome assessors, lack of DVT prophylaxis, and more people unable to have surgical fixation in the control group. 25 The second study reviewed was Prevention du Risque d'Embolie Pulmonaire par Interruption Cave (PREPIC), involving 400 patients and was found to lack statistical power to detect reduction in PE over shorter time periods as described earlier. 20 Based on these 2 studies, the review concluded that no recommendations can be made on the basis of these 2 studies, and ACCP guidelines 7 remain valid. 24
In another review involving 37 studies comprising 6834 patients, the rate of PE after IVCF placement was only 1.7%. 13 However, multiple complications were reported, especially with long-term use (>30 days), and mean retrieval rate was found to be only 34%. 13
In a recently published meta-analysis of 7 studies 26 involving 1900 patients with trauma, the rate of PE was statistically lower in the IVCF group as compared to a matched control group without IVCFs (odds ratio [OR] 0.21, 95% CI 0.09-0.49). No significant difference in DVT was reported (2 studies, OR 1.6, 95% CI 0.76-3.37). However, pharmacologic prophylaxis was used only in 4 of the 7 studies, leading to no recommendations for or against prophylactic IVCFs. 26
In a study involving 49 patients with intracranial malignancies and VTE at Brigham and Women’s Hospital, Boston, 42 patients received IVCF. The rate of complications was strikingly high (62%) in the IVCF group with 12% having recurrent PE and 57% developing filter thrombosis, recurrent DVT, or postphlebitic syndrome, all of which significantly reduced the quality of life. 27
The ACCP recommends against the routine use of vena cava filters in addition to anticoagulants in most patients with DVT (grade 1A). 7 The IVCF placement is suggested in patients with DVT or PE having complications or contraindications to anticoagulant treatment or with recurrent thromboembolism despite adequate anticoagulation (grade 2C). 7 The IVCF placement is not recommended for primary prophylaxis or against PE in patients with trauma (grade 1C). 8 The EAST recommends insertion of prophylactic vena cava filter in patients with very high-risk trauma who cannot receive anticoagulation because of increased bleeding risk and have an injury pattern rendering them to be immobilized for prolonged period of time including severe closed head injury (Glasgow Coma Scale score <8), incomplete spinal cord injury with paraplegia or quadriplegia, and complex pelvic fractures associated with long bone fractures and multiple long bone fractures (class III). 19
Our experience suggests that most physicians are unaware of IVCF-related adverse events, namely, migration, embolizations (detachment of device components), perforation of IVC, and filter fracture. Vena cava filters are perceived as a safe alternative to anticoagulation for prevention of PE in noncompliant patients or patients at risk of falls or with anticipated prolonged immobilization. In our study, a vast majority (74.4%) of patients had IVCF placed for similar relative or prophylactic reasons including noncompliance, fall risk, and prolonged immobilization after surgery or trauma.
Our study is limited due to availability of a short follow-up with a median of 108.5 days on only 96 patients. Our other limitation is that we did not compare rates of VCF placement before and after an institutional policy. Placement of IVCFs without proper indications, loss to follow-up, continuation even after cessation of indication, and low retrieval rate were the areas that continue to be a major problem compromising patient safety. In our study, a majority (63.4%) of patients had IVCF placed just for prophylaxis. Also 47.6% patients with retrievable filters were deemed lost to follow-up, which significantly contributes to low retrieval and predisposition to potential complications due to prolonged unnecessary continuation of IVCF beyond indication.
We suggest setting up of strict IVCF placement protocols in our institution. Patients should be educated regarding IVCF both before placement and at discharge and should be given an IVCF card, written pamphlets/handouts, and/or IVCF lockets. We also suggest setting up of dedicated IVCF registries to keep track of patients in whom the filter is no longer indicated and dedicated IVCF clinics for improved patient follow-up. These have shown to improve filter retrieval rate. 28,29 Physician awareness and education will also help a long way in achieving these objectives.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.