
Abstract
Hospitalized acutely ill patients face high risk for venous thromboembolism (VTE) unless appropriate thromboprophylaxis is applied. This study aimed to determine VTE prophylaxis practices for inpatients in Turkey and to evaluate the impact of physicians’ training via a modified “Standard Medical Patients’ VTE Risk Assessment Model (MERAM).” A total of 607 inpatients included in this national multicenter noninterventional observational registry were evaluated in terms of demographics, VTE risk, and preventive measures at 2 consecutive cross-sectional visits. Physicians were asked to complete a questionnaire on current VTE method risk assessment and other models including MERAM. The VTE prophylaxis rates significantly increased from 49.4% to 62.4% between visits (P < .05). The lack of risk evaluation decreased from 74.6% to 19.5% (P < .001). Percentage of physicians using prophylaxis and use of MERAM increased between visits. Physician training proved effective for providing general “awareness” of VTE prophylaxis and led to higher rates of risk assessment model-based appropriate VTE prophylaxis.
Keywords
Introduction
Venous thromboembolism (VTE), a collective term for a spectrum of diseases including deep vein thrombosis (DVT) and pulmonary embolism (PE), is commonly associated with clinically symptomatic and asymptomatic episodes and high mortality in hospitalized patients. 1 –4 Randomized-controlled trials and epidemiological studies demonstrated that more than half of the patients who developed symptomatic VTE had medical risk factors rather than surgical ones. 5 Medical patients comprise around 60% of all hospital admissions; and it is estimated that 50% to 70% of symptomatic thromboembolic events and 70% of fatal PE occur in hospitalized medical patients. 1,2,6 Without prophylaxis, the incidence of DVT and PE in ill medical patients was shown to be comparable to that reported in surgical patients having moderate risk. 7 In this regard, acutely ill medical patients are considered to form a clinically heterogeneous group of patients at significant but preventable risk of VTE complications. 8,9 The burden of thromboembolic disease in medical settings was stated to be substantial in terms of morbidity and mortality. 4
The American College of Chest Physicians (ACCP) guidelines strongly recommend that certain groups of hospitalized medical patients should routinely receive thromboprophylaxis. 8,9 Nonetheless, it is evident that a critical gap exists between the strong evidence in support of thromboprophylaxis in high-risk groups and its implementation in practice, 10 generally in medical patients than in hospitalized surgical patients. 11 The principle reasons identified to explain the consistent underuse of VTE prophylaxis in patients having medical illnesses were as follows: insufficient awareness of clinicians of the burden of the problem, lack of an optimal system to assess and stratify VTE risk (eg, easy-to-use and convenient national guidelines), significant heterogeneity of the general medical population, and concern about potential bleeding risk. 4,12 Implementation strategies such as providing educational material and/or computer alert reminders, and patient-mediated interventions were reported to be effective in other clinical areas. 13 However, there has been little research on effective knowledge translation strategies specifically targeted to VTE prevention apart from continuing medical education and use of computer-generated alerts. 10
Various risk assessment models (RAMs) for VTE are widely employed and have been validated in surgical patients. However, a correct assessment of individual VTE risk is more challenging in nonsurgical patients because of more heterogeneous clinical features and limited number of clinical studies in this group. 4 Therefore, availability of a standardized, validated, and easy-to-use RAM for clinical practice is crucial for optimal management of VTE prophylaxis in medical patients. 4,14
As evidenced by 3 large multinational studies including Epidemiologic International Day for the Evaluation of Patients at Risk for Venous Thromboembolism in the Acute Hospital Care Setting (ENDORSE), 15 International Medical Prevention Registry on Venous Thromboembolism (IMPROVE), 16 and Deep Vein Thrombosis FREE (DVTFREE), 3 appropriate prophylaxis rates in at risk medical patients varied from 39.5% to 60% and that prophylaxis rates in surgical patients were higher than that in medical patients. 17
Data from Turkey in the ENDORSE study revealed that based on the 2008 ACCP criteria, VTE risk was observed in 36% of patients (65% surgical and 24% medical) and the VTE thromboprophylaxis rate in these patients was 39% for both surgical and medical patients. These results reinforce the rationale for urgent implementation of hospital-wide strategies for systematically assessing VTE risk and providing appropriate prophylaxis. 18
In this regard, the present Standard Medical Patients’ VTE RAM (MERAM) study was designed to evaluate the appropriate VTE prophylaxis practices in hospitalized patients who were carrying thrombosis risk in a selected group of hematology, cardiology, oncology, neurology, and pulmonary medicine clinics in Turkey, before and after training the physicians on fundamental principles of thromboprophylaxis. Additionally, by providing the MERAM form adapted for Turkish population by the multidisciplinary steering committee, we were able to collect data on the initial testing of this form in real hospital settings in Turkey.
Methods
Study Population
A total of 607 inpatients from 55 centers, including university hospitals, Ministry of Health state, or research and training hospitals, in 9 cities across Turkey were included in this national, noninterventional observational study conducted between November 2009 and November 2010. Immobilized medical patients who were hospitalized at selected cardiology, oncology, hematology, neurology, and chest disease departments for medical reasons other than any surgical intervention and who have signed an informed consent were enrolled. Immobilization was defined as having reduced mobility for at least 3 days. Reduced mobility was considered as requiring total bed rest or being sedentary without bathroom privileges (level 1 immobility) or with bathroom privileges (level 2 immobility). 19 Patients receiving VTE prophylaxis treatment and pregnant or nursing women at the time of enrollment were excluded from the study. Ethics committee and Ministry of Health approvals were obtained before the initiation of the study.
Two cross-sectional study phases were defined at the same study sites, and data from 346 and 261 patients, respectively, were collected within a 90-day interval before and after training the physicians on VTE prophylaxis and the MERAM form. All treatment decisions were left to the discretion of the physician and documented in the case report form.
Treatment was not modified in enrolled patients as investigators were asked to collect previous and current VTE data in accordance with the basic principles of Good Epidemiological Practice. Ethics committee and Ministry of Health approvals were obtained before the initiation of the study.
MERAM Form
The MERAM form (Figure 1) is a modified version of the of the RAM reported by Cohen et al 20 and adapted for Turkish population by the multidisciplinary steering committee and approved by different Medical Societies in Turkey.
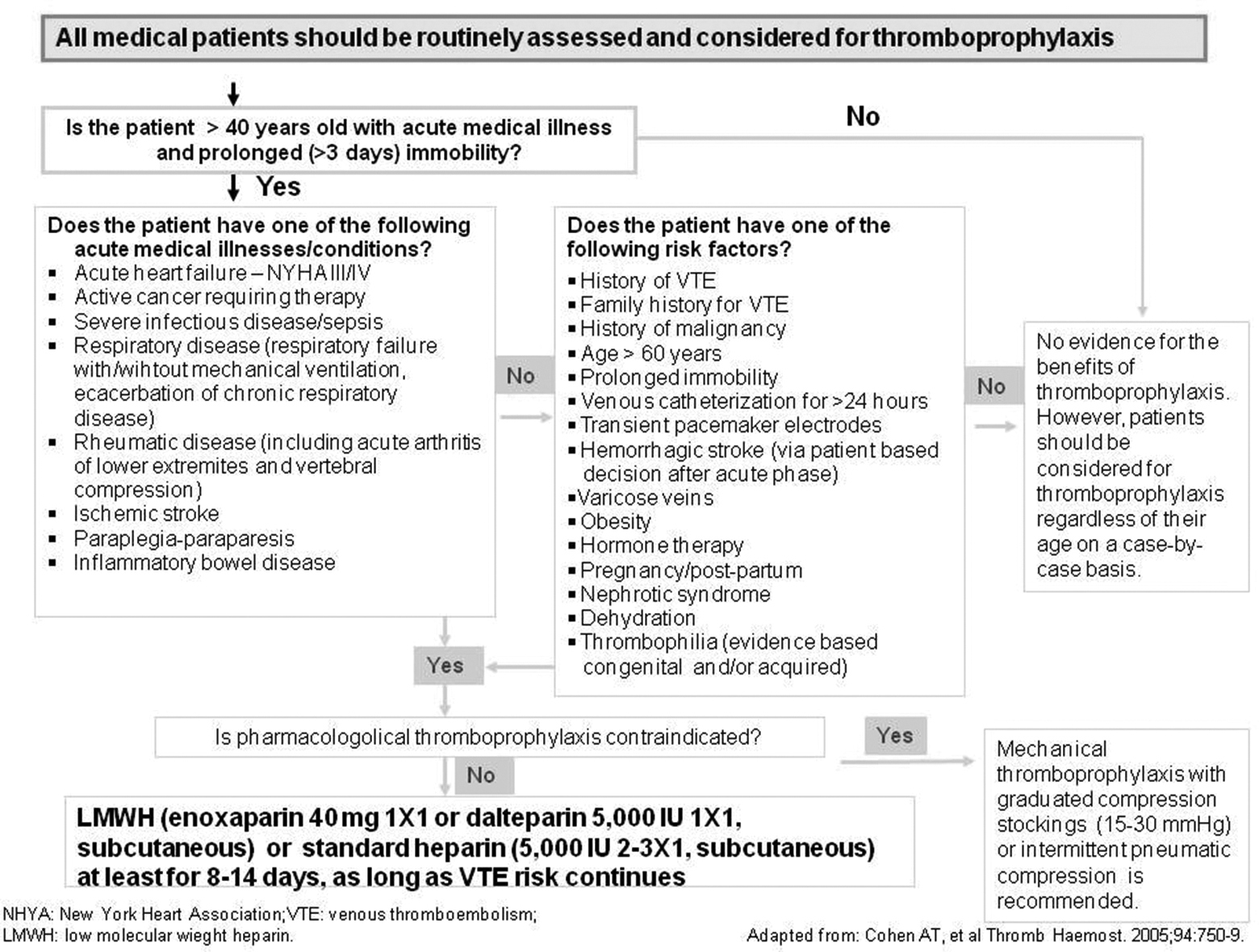
The MERAM for assessment of VTE risk in medical patients. MERAM, Standard Medical Patients’ VTE Risk Assessment Model; VTE, venous thromboembolism.
Unlike the original RAM, 20 the MERAM form does not classify medical illnesses and risk factors as evidence based and consensus based. Among the medical illnesses, acute myocardial infarction is excluded in the MERAM form since the immobilization duration is less than 24 hours with the benefit of on-time reperfusion treatment and prophylactic parenteral anticoagulant use in the current practice. The MERAM includes additional risk factors such as hemorrhagic stroke, 21 family history of VTE, venous catheterization for >24 hours, and transient pacemaker electrodes.
First Cross-Sectional Phase
This cross-sectional study phase (day 0; n = 346; mean (standard deviation [SD]) age: 58.9 (17.1) years; 58.1% males) was conducted as a baseline survey and performed in a single day at each participating institution. Data on patients’ demographics, VTE risk factors (prolonged immobilization, obesity, prior VTE, venous insufficiency, sex hormone use, and others), VTE risk (low, moderate, high, or very high) of the patients were assessed by the physician. Also, the type of thromboprophylaxis provided was collected at this visit. Additionally, the physicians were asked to complete a questionnaire on the current method of VTE risk assessment at their clinical setting and use of any RAMs, if any.
Physician Training
After the completion of the first cross-sectional data collection phase, the physicians were invited to a Web-based training on the basic principles of VTE prophylaxis for inpatients hospitalized for medical reasons and were introduced to the MERAM form. The training module was prepared by the coordinating physician of the participating subspecialties. This Web-based system enabled assessment of training metrics. Physicians, whose completion exceeded 51%, were asked to initiate the second cross-sectional visit.
Second Cross-Sectional Phase
The second cross-sectional study phase (n = 261; mean (SD) age: 63.5 (15.3) years; 52.5% were males) was conducted after approximately 90 days from the baseline survey at the same sites. Similar to the first cross-sectional visit, it was performed in a single day at each participating clinic, and data on VTE risk factors, VTE risk of the patients, and VTE preventive measures were collected. Additionally, the physicians’ questionnaire had 2 additional items concerning the use of the MERAM form and the reasons for not using the MERAM form, if they did not.
Study Parameters
The rate of medical inpatients who received any form of appropriate VTE prophylaxis in line with ACCP guidelines and the rate of use of various RAM forms in patients hospitalized for medical reasons were evaluated prior to and after training of physicians on thromboprophylaxis and risk assessment management. Patient demographics, risk profiles, and pharmaceutical or other forms of VTE prophylaxis employed for inpatients were the other parameters evaluated.
Statistical Analyses
The study sample size calculation was based on the outcomes of the Turkish arm of the ENDORSE study, 19 which showed that the VTE risk was 24% among medical patients, while only 39% of them were receiving thromboprophylaxis despite their risk.
It was postulated that the rate of prophylaxis for hospitalized medical patients in any medical subspecialty clinic could be increased to 45% after training on VTE prophylaxis. To compare the rate of prophylaxis before and after training program with a type 1 error (α) of .05 (2-sided) and a power of 95%, the number of patients expected to be enrolled for each subspecialty was calculated to be a minimum of 97, leading to the estimated sample size of 970. However, because a total of 607 patients at both phases could be included, comparisons between 5 subspecialties were omitted.
Statistical analyses were conducted using the computer software SPSS (version 13.0; SPSS Inc, Chicago, Illinois). Data are mean (SD), minimum–maximum, and percentage where appropriate. Comparisons were done by Student t test, chi-square, or analysis of variance tests for parametric data; Mann Whitney U, and Kruskal Wallis tests were used for nonparametric data comparisons. Statistically significance was set at P < .05.
Results
Sociodemographic and Basic Clinical Features of Patients
The basic sociodemographic and clinical features of the patients included in first and second phases were not significantly different than each other except age. By chance, the second group of patients was slightly but significantly older (mean (SD) age: 58.9 (17.1) vs 63.5 (15.3) years; P < .05).
Patients who were hospitalized at 5 different medical clinics mostly had chronic diseases and were confined to bed and treated medically. The most common reasons identified for hospitalizations were acute leukemia (n = 43; 40.6%) in hematology, ischemic stroke (n = 81; 61.4%) in neurology, chemotherapy (n = 46; 40.3%) in oncology, cardiac failure (n = 45; 40.2%) in cardiology, and obstructive pulmonary disease (n = 66; 46.0%) in chest disease departments.
The majority of the patients at both phases had 2 or 3 risk factors (70.5% and 62.8%, respectively), and the most frequent risk factors for VTE were prolonged immobilization, obesity, and malignancy. The percentage of patients’ additional risk factors (9.5% vs 15.7%) was significantly higher at the second cross-sectional phase than that at the first cross-sectional phase (P < .05). There was no significant difference between 2 phases with respect to the overall number of risk factors (Table 1).
Risk Factors (RFs) for VTE Identified at Both Cross-Sectional Phases.
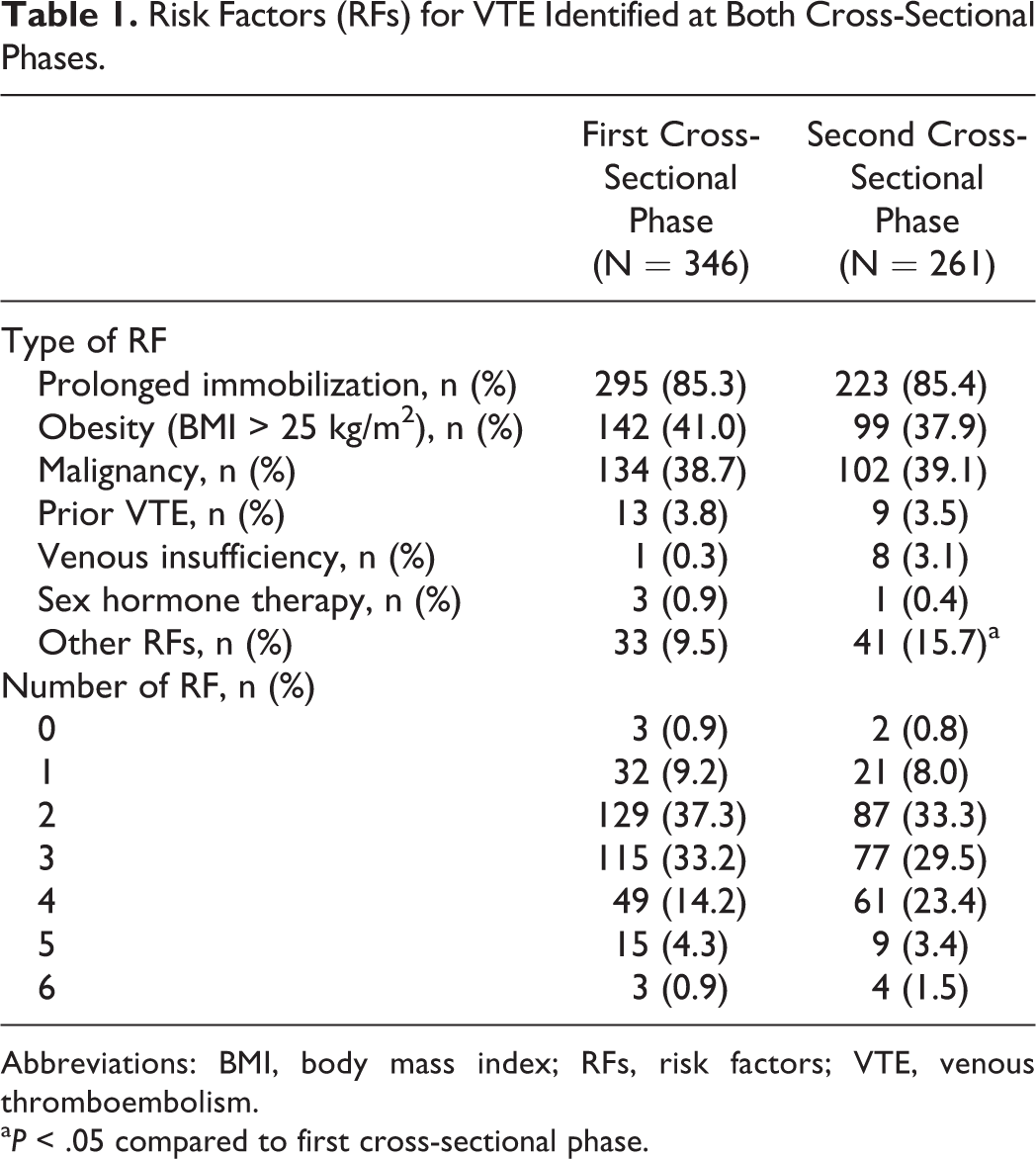
Abbreviations: BMI, body mass index; RFs, risk factors; VTE, venous thromboembolism.
a P < .05 compared to first cross-sectional phase.
Only a minority of the patients (1.7% and 2.7% at the first and second phases, respectively; P < .05) had received any VTE treatment prior to entry in the study.
Application of VTE Prophylaxis
During the first cross-sectional phase, absence of risk evaluation was evident for 74.6% (n = 258) of the patients, which was significantly decreased to 19.5% (n = 51) during the second visit (P < .001). On the other hand, considering the use of VTE prophylaxis at both cross-sectional phases, VTE prophylaxis rate was determined to be significantly increased from 49.4% (n = 171 of 346) at the first visit to 62.4% (n = 163 of 261) at the second visit (P < .05).
Anticoagulants were the most commonly prescribed medications for VTE prophylaxis at both visits (85.4% and 91.4%, respectively). Among anticoagulant and antiplatelet medications, low-molecular-weight heparin (LMWH) was used in 79.0% and 83.4% (P = .294), aspirin (ASA) in 42.7% and 47.9% (P = .345), clopidogrel in 10.5% and 17.8% (P = .055), warfarin in 11.7% and 12.3% (P = .873), UFH in 1.2% and 3.7% (P = .134) of patients at the first and second visits, respectively. Intermittent pneumatic compression was the most used nonpharmacological treatment for VTE prophylaxis (77.8% and 75.0% at first and second visits, respectively).
Median duration of VTE prophylaxis was as follows at the first versus second cross-sectional phases: ASA use, 10.7 (2-317) versus 13.2 (2-62) days (n = 14); clopidogrel use, 30.4 (2-31) versus 10.4 (2-41) days (n = 7 and 9); LMWH use, 8.1 (1-57) versus 10.7 (1-70) days (n = 115 and 126); unfractionated heparin (UFH) use, 14 versus 5.6 (1-28) days (n = 2 and 6); and oral anticoagulant use, 11.2 (8-61) versus 6.6 (1-8) days (n = 7 and 4).
When the rate of VTE prophylaxis administration to certain groups of patients who should receive prophylaxis based on the criteria included in the MERAM form was evaluated, only half of those patients received prophylaxis; this percentage significantly (P = .0014) rose to 62.2% during the second phase (Table 2). Logistic regression analysis revealed that the combination of the effect of immobilization, chronic heart failure, and age >40 years was a significant determinant of prophylaxis decision both at the first and second cross-sectional phases (P < .001 for each), while prolonged immobilization per se was not considered a significant determinant.
Rate of VTE Prophylaxis Administration in Certain Groups of Patients Who Should Receive Prophylaxis Based on the Criteria Included in the MERAM Form.
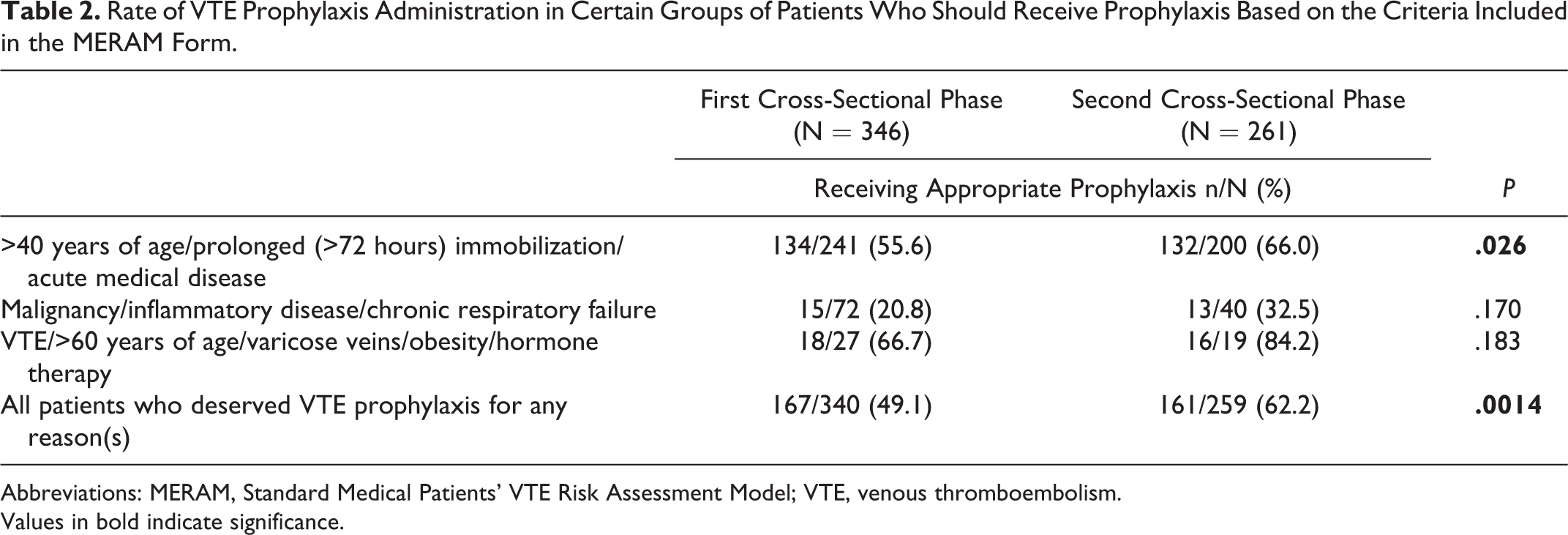
Abbreviations: MERAM, Standard Medical Patients’ VTE Risk Assessment Model; VTE, venous thromboembolism. Values in bold indicate significance.
Method/Practice Implemented by Physicians for VTE Prophylaxis
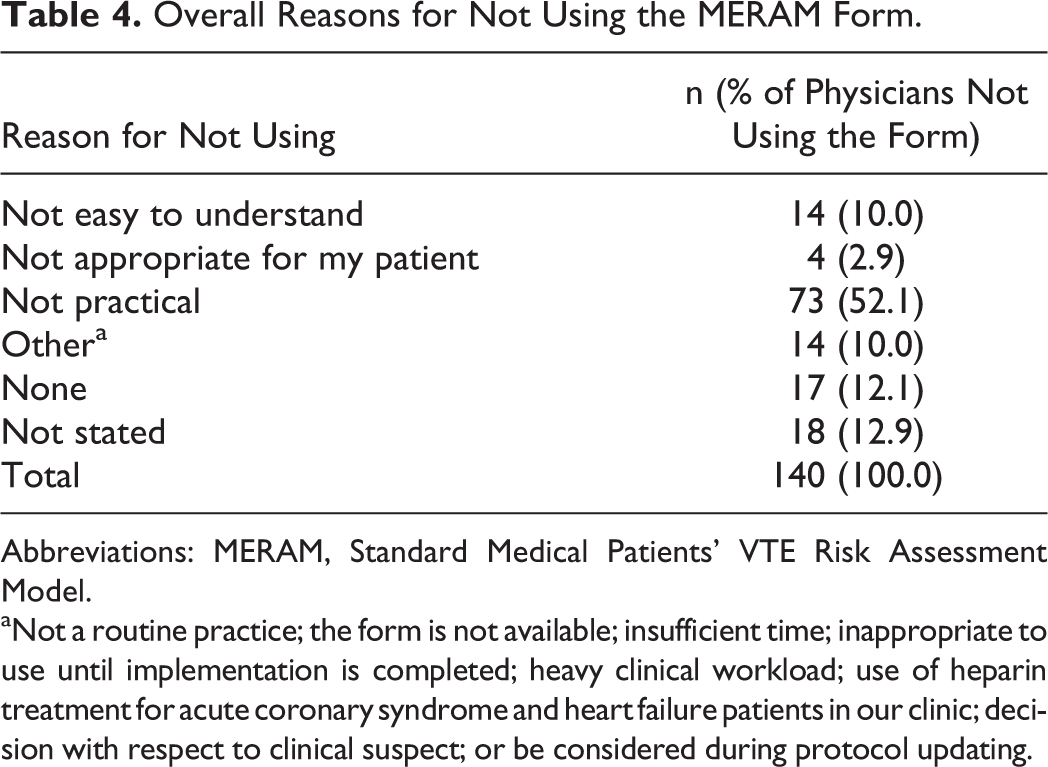
Physicians, who have given some form of prophylaxis to their patients, were additionally questioned on the method/practice they implemented for this prophylaxis at the first (n = 203) and second (n = 208) visits. The percentage of physicians recommending VTE prophylaxis to their patients was determined to be 85.2% at the first visit, while it increased to 97.1% at the second visit. Questioning physicians regarding the method/practice they implement for assessing the need for prophylaxis revealed an increase in the use of the MERAM form (9.8%-33.7% across visits) or the anonymous risk form of their departments (6.9%-11.4%). In contrast, other risk assessment methods declined after training programs (personal decision, 55.5%-40.1%; with senior medical officer’s decision, 24.3%-17.8%; and after consultation, 8.7%-2.5%; Table 3). Lack of practicality was the most commonly declared reason for not using the MERAM form by physicians when they were asked on the basis of each individual patient (Table 4).
Method/Practice Implemented by Physicians for VTE Prophylaxis.
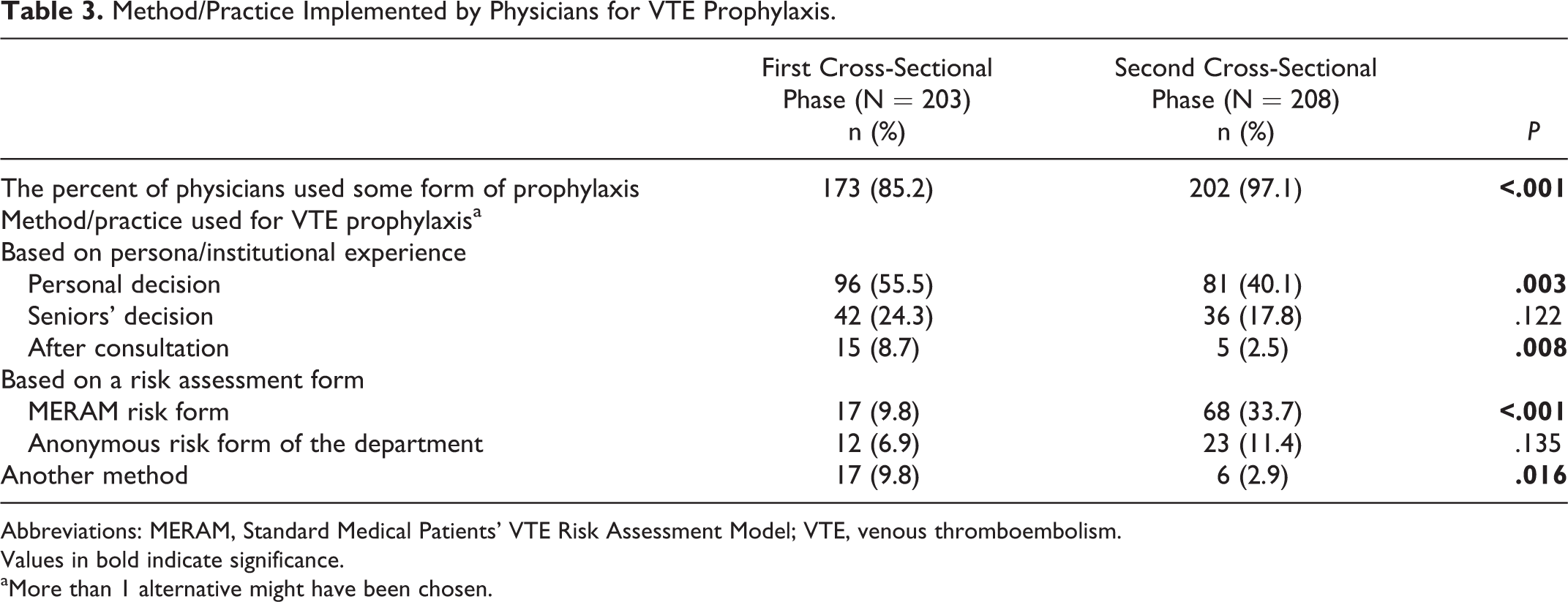
Abbreviations: MERAM, Standard Medical Patients’ VTE Risk Assessment Model; VTE, venous thromboembolism. Values in bold indicate significance.
aMore than 1 alternative might have been chosen.
Overall Reasons for Not Using the MERAM Form.
Abbreviations: MERAM, Standard Medical Patients’ VTE Risk Assessment Model.
aNot a routine practice; the form is not available; insufficient time; inappropriate to use until implementation is completed; heavy clinical workload; use of heparin treatment for acute coronary syndrome and heart failure patients in our clinic; decision with respect to clinical suspect; or be considered during protocol updating.
Discussion
Our findings related to the evaluation of the appropriate VTE awareness and prophylaxis practices in Turkey among a selected population of medical ward physicians revealed a significant improvement in patient’s risk assessment following training of physicians on fundamental principles of thromboprophylaxis, physical examination, and methods of evaluation of at risk patients who are hospitalized.
The key finding obtained from this first national registry study by training and providing a MERAM form was the significant decrease in the number of physicians not employing any method/test or form for the evaluation of VTE risk among hospitalized patients from 74.6% at the first cross-sectional visit to 19.5% in the second visit.
Strikingly, despite homogenous patient groups enrolled at both visits, a higher number of patients having additional risk factors in the second visit seemed to be associated with the significant difference observed in the assessed VTE risk levels. Physicians who have prescribed any type of prophylaxis were additionally questioned on the method/practice they implemented, and data indicated an increase in the administration of pharmacological prophylaxis (85.2%-97.1% across visits) as well as in the use of the MERAM form (9.8%-33.7%) or an anonymous risk form of their departments (6.9%-11.4%) following the training of physicians. In contrast, other risk assessment methods declined after training programs (personal decision, 55.5%-40.1%, P = .003; with senior medical officers decision, 24.3%-17.8%, P = .122; and after consultation, 8.7%-2.5%, P = .008).
Providing the first large-scale, epidemiological data on the number of patients at risk for VTE in the acute care hospital setting as well as the proportion of these at risk patients who received prophylaxis as recommended by the ACCP guidelines, global results of ENDORSE study 15 revealed the rate of receiving ACCP-recommended VTE prophylaxis to be much lower in medical patients (39.5%) compared with surgical patients (58.5%). In the Turkish arm of ENDORSE study, 18 VTE prophylaxis was prescribed in only 39.0% and 38.5% of surgical and medical patients, respectively. Indeed, risk for VTE among Turkish medical patients (23.8%) was reported to be lower than reported in the global data from ENDORSE study (41.5%) 15 as well as in other studies including IMPROVE (60.0%) 16 and CURVE (90.0%). 10 This may indicate the likelihood of insufficient awareness of physicians about VTE risk evaluation that may be associated with the availability of more detailed former studies in surgical patients for much longer time than studies concerning prophylaxis of medical patients. 18 Notably, data from a recent observational study for VTE risk assessment among hospitalized patients in general surgery clinics across Turkey revealed the benefit of using a standard VTE prophylaxis and risk factor assessment form in achievement of higher rates of VTE prophylaxis (65.9%) for surgical patients at high risk for VTE. 22
The above-mentioned figures may indicate the need for valid and reliable diagnostic guidelines and risk assessment tools specific to VTE screening in medical wards in Turkey.
Compatible with higher use of risk assessment forms after training, the percentage of patients receiving thromboprophylaxis increased from 49.4% at the first visit to 62.4% during the second cross-sectional visit in our study population.
Given the fact that the risk for developing VTE increases with the increasing number of risk factors, identification of 3 or more risk factors in 52.6% and 57.8% of our patients at first and second visits, respectively, is notable.
Indeed, the rate of prophylaxis in our medical patients before physician training (49.4%) was higher than the rate reported in Turkish arm of ENDORSE study (39.0%). In this regard while physician training seems to have substantial influence on the increase of VTE prophylaxis to include more than 60% of patients, the meeting for awareness conducted with participating physicians before the study initiation might be contributing to the higher VTE prophylaxis rate than the Turkish arm of ENDORSE even before the training.
Nevertheless, integrated quality improvement initiatives incorporating several active strategies were suggested to be more effective at improving VTE prophylaxis practices compared with a single strategy. 23 –25 In this regard, combined regular physician education, a decision support tool, and a mechanism for audit and feedback were reported to lead to a significant improvement in the proportion of medically ill patients receiving appropriate prophylaxis from 43% to 85% after 18 months. 23
A number of strategies have been suggested in an attempt to improve the use of thromboprophylaxis in medical patients including development of easy to follow and simple clinical guidelines, introduction of a simple RAM to perform for routine use, and local specific educational programs both in teaching and in nonteaching hospitals. 4
Hence, one of the foremost gains of the present study was the development of a modified RAM, the MERAM form, which was shown to be an essential step to increase the general awareness and the associated rate of use of thromboprophylaxis. The study coordinating committee has assigned another important task during the planning phase of this important registry study; implementation of an “easy-to-use” risk assessment form in Turkish (MERAM form), which could be available after the completion of the training period as a handy tool for daily use. Although this form was created as part of “risk assessment management” tool implementation, participating physicians were free to use any method for VTE risk assessment. Accordingly the MERAM form was used by a significantly higher percentage of physicians at the second visit performed after training (33.7%) than those at the first visit (9.8%), whereas no significant increase was observed in the use of an anonymous risk form of their departments (6.9%-11.4%) after training.
Considering criteria included in MERAM form for administration of VTE prophylaxis, patients aged >40 years and/or with prolonged immobilization (>72 hours) and/or with any acute medical condition (55.6%-66.0%); patients with any form of cancer and/or inflammatory disease and/or chronic respiratory insufficiency (20.8%-32.5%); and patients with VTE and/or aged over 60 years, and/or with various veins, and/or receiving any form of hormone replacement treatment, and/or obesity (66.7%-84.2%) were determined to have higher likelihood of receiving appropriate prophylaxis at the second visit after the training.
Besides, combination of 3 factors including immobilization, chronic heart failure, and age >40 years was identified as the significant determinant of prophylaxis decision both at the first and at the second cross-sectional visits.
Although a relatively large number of studies have evaluated the safety and efficacy of UFH and LMWH in the prevention of VTE in surgery, few studies have been performed in patients having general medical illnesses; moreover, trials regarding thromboprophylaxis in internal medicine have often small sample sizes and methodological limitations. 4 Nevertheless, guidelines recommend use of LMWH or UFH (5000 U 3 times daily) for VTE prophylaxis in hospitalized medical patients with risk factors for VTE; in patients with contraindications to anticoagulants, mechanical prophylaxis is recommended. 7 In this respect, administration of LMWH as medical treatment and intermittent pneumatic compression as nonmedical treatment for VTE prophylaxis in majority of our patients at both visits is in accordance with the ACCP guidelines. 9
Results of the present study showed that, in Turkey, physicians working in medical wards are more or less aware of the importance of VTE prophylaxis, whereas no local guidelines are available in the clinical practice. Current VTE prophylaxis largely depends on decisions within the clinics given either by senior physicians or by treating physicians themselves. Physicians, on the other hand, are willing to use a well-established RAM; however, continuous reinforcement may be needed to increase the rate of correct thromboprophylaxis. In this respect, since lack of practicality was the most commonly identified reason for not using the MERAM form by physicians at each department ranging from 72.7% in cardiology to 37.5% in hematology, it should be improved and further evaluated in well-designed prospective clinical trials.
The limitations of our study are that we did not evaluate the long-term impact of MERAM application; and since the study centers were the third step health care institutions, our results cannot be extrapolated to all health care system in Turkey. In addition, due to the observational nature of the study, some potential confounding factors might not have been controlled.
In conclusion, our findings have shown that increased awareness of VTE prophylaxis and use of an appropriate RAM in a selected patient population who were hospitalized for longer durations due to medical reasons led to an increase in appropriate VTE prophylaxis. Our findings also provide data for the initial testing of a modified RAM and a consequent form in real hospital settings across Turkey.
Footnotes
Appendix A
Acknowledgments
Authors would like to thank to Prof Sule Oktay, MD, PhD, and Cagla Ayhan, MD, from KAPPA Consultancy Training Research Ltd (Istanbul, Turkey) for their support in article preparation, and to Arzu Calisgan, MSc, from Monitor Medical Research and Consulting (Istanbul, Turkey) for statistical analysis both funded by Sanofi Turkey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Sanofi Turkiye (grant number DIREG_04484).