
Abstract
The prevalence of the Factor V Leiden (FVL; G1691A) mutation and the methylenetetrahydrofolate reductase (MTHFR; C677T) mutation was determined in 180 patients with sickle cell (SS) disease (126 sickle homozygous and 54 sickle β-thalassaemia—age 1-47 years) and in 130 healthy controls. The FVL mutation in the heterozygous state was present in only 3 patients with SS disease and was absent in the controls. Genotyping of MTHFR 677C > T revealed increased frequency of the C allele than the T allele in patients as well as in controls. This suggests that these genetic markers may not be major risk factors for a hypercoagulable state in Indian patients with SS disease.
Introduction
Sickle cell (SS) anemia is an autosomal recessive disorder caused by a substitution of glutamic acid by valine at the sixth position of the β-globin gene (hemoglobin beta gene, on chromosome 11p15.4). Although it is a monogenic disorder, it behaves clinically as a multigenic trait with phenotypic variability. 1
Patients with SS anemia have a varied clinical expression ranging from death in childhood to recurrent painful vaso-occlusive crisis and multiple organ damage in adults, and to being relatively well even in old age. 1 The coinheritance of α-thalassemia and the −158 (C→T) polymorphism in the Gγ globin gene promoter explains some of the clinical heterogeneity but cannot explain interindividual variability in many cases. This indicates that additional regulatory elements may be involved. Thus, it is necessary to study different polymorphic variations in various nonglobin genes to understand the pathogenesis of the disease. 2–5
A hypercoagulable state in SS disease has been well established. 6 Vascular thrombosis is a common complication observed in patients with SS disease. Coagulation and fibrinolytic abnormalities lead to the development of hypercoagulability. Vaso-occlusive crisis, acute chest syndrome, and occlusive stroke are the major causes of death in patients with SS disease. These complications result from previous thromboembolism events and endothelial cell damage. 7
A single-point mutation 1691G-A in the gene coding for coagulation factor V results in an Arg 506-Gln (factor V Leiden [FVL]) substitution that is resistant to degradation by activated protein C and leads to a relative hypercoagulable state. A mutation in the thermolabile methylenetetrahydrofolate reductase (MTHFR; C677T), which leads to an Ala 677-Val switch, shows elevated serum homocysteine levels. These increased levels are an important risk factor for vascular disease. 7 The prothrombin G20210A mutation involves a guanine to adenine substitution at nucleotide 20210 of the prothrombin gene. The mutation is associated with an increased plasma concentration of prothrombin, which leads to an increase in thrombin generation, and an increased risk of thrombosis. 7,8 In this study, we have determined the prevalence of the FVL and MTHFR (C677T) mutations in patients with SS disease from western India.
Materials and Methods
A total of 180 patients with SS disease were studied. They included 126 patients who were sickle homozygous (76 males and 50 females) with median age of 12 years (range, 1-47 years), and 54 patients with sickle β-thalassemia (26 males and 28 females) with median age of 10.5 years (range, 1to 41 years). A well-designed proforma was filled up to record the clinical findings for all the patients. Various clinical phenotypes such as the presence of vaso-occlusive crisis, avascular necrosis, and acute chest syndrome were taken into consideration. Blood samples were collected in tubes containing EDTA after taking an informed consent from the patients and the parents of pediatric patients. The control group included 130 age- and sex-matched individuals from the same population group. The study was undertaken after obtaining clearance from our institutional ethics committee.
Methods
Red cell indices were measured on an automated blood cell counter (Sysmex K 1000, Sysmex Corporation, Japan). Hemoglobin A2, fetal hemoglobin, and sickle hemoglobin (HbS) levels were measured using cation exchange high-performance liquid chromatography on the Variant Hemoglobin Testing System (Bio-Rad Laboratories, Inc, Hercules, California). 9 Genomic DNA was isolated from peripheral blood leucocytes using the QIAamp Blood Mini Kit (Qiagen Inc. USA). Confirmation of the sickle status was done by reverse dot-blot hybridization. 10
Detection of FVL Mutation (G1691A)
The presence of the FVL mutation was detected by single specific primer-polymerase chain reaction (PCR), using sequence-specific primers with 3′end mismatches as described earlier. A normal- or mutant-specific fragment of 240 bp for the G and A allele was observed along with a control band of 424 bp. 11
Detection of the MTHFR Mutation (C677T)
The MTHFR gene mutation was detected by PCR and restriction enzyme digestion using HinfI. A fragment of 175 bp corresponded to the mutant allele and 198 bp to the wild-type allele. 7
Statistical Analysis
Allele and genotype frequencies were compared by standard contingency table analysis using the 2-tailed Fisher exact test probabilities. Statistical significance was defined as a P value
Results
Clinical evaluation of our patients showed different clinical phenotypes as well as variable severity. Vaso-occlusive crisis was observed in 103 of our patients with variable severity. Of the 67 sickle homozygotes with vaso-occlusive crisis, 40 were males and 27 were females. In all, 37 (19 males and 18 females) patients with sickle β-thalassemia also had vaso-occlusive crisis. Acute chest syndrome was observed in 8 (5 males and 3 females) patients with SS disease of which 4 were sickle homozygous and 4 were having sickle β-thalassaemia. In all, 8 patients had avascular necrosis (5 males and 3 females) of which 6 were sickle homozygous and 2 were sickle β-thalassemia. One patient who was sickle homozygous had a history of stroke. Heterozygous FVL G/A was observed in 3 patients with vaso-occlusive crisis, whereas 1 patient with crisis showed the presence of the homozygous MTHFR mutation (677T). Patients with acute chest syndrome and avascular necrosis did not show these polymorphic variations (Table 1).
Prevalence of Inherited Risk Factors for Vascular Disease in Patients With Sickle Cell Disease.
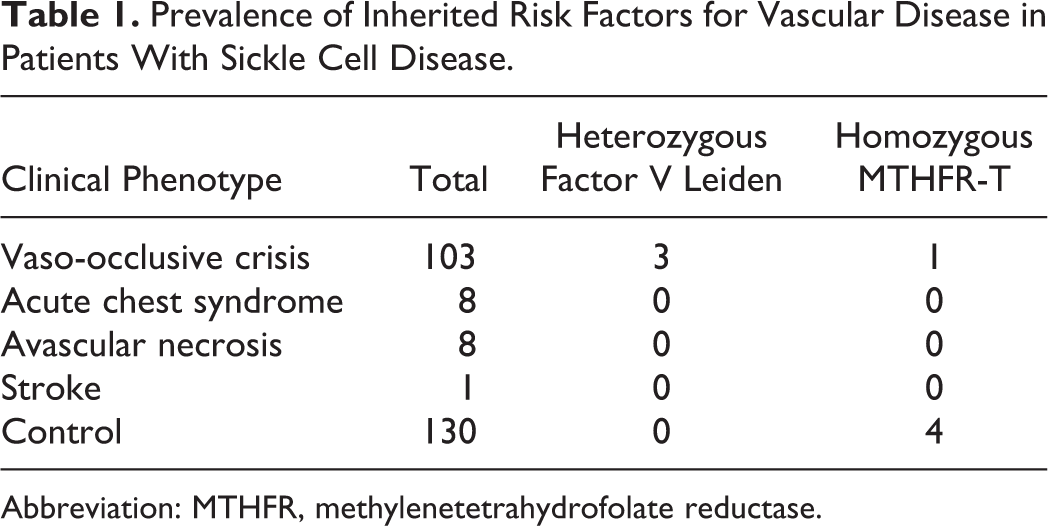
Abbreviation: MTHFR, methylenetetrahydrofolate reductase.
The homozygous G/G genotype of FVL was seen in 97.6% of the patients and all the normal individuals. The homozygous mutant genotype (A/A) was found to be absent in this study. Frequency of the G allele was significantly increased when compared to the A allele (Table 2).
Distribution of G and A allele of Factor V Leiden (P Value = .139).
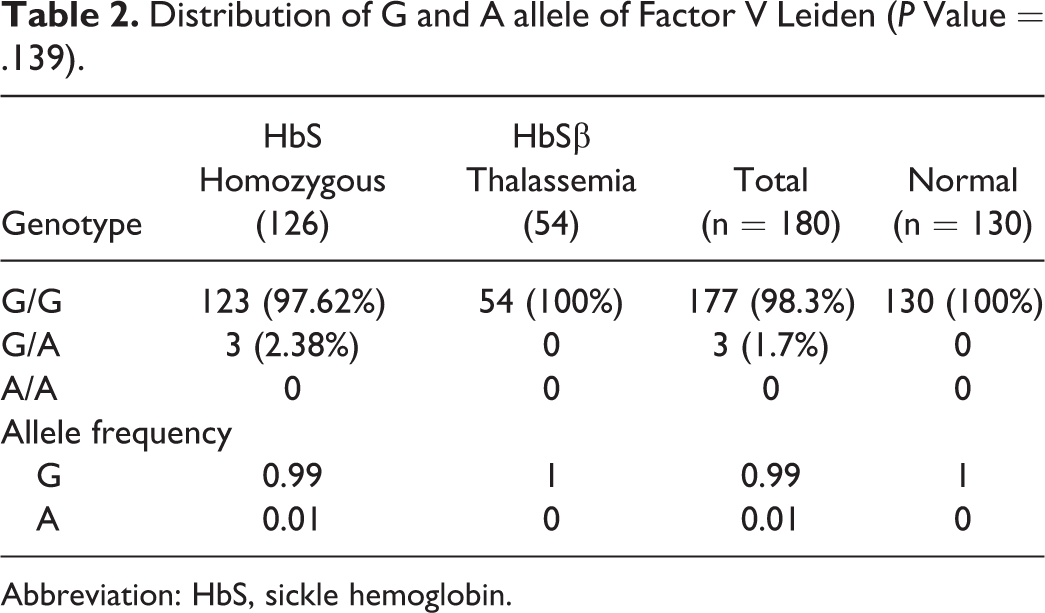
Abbreviation: HbS, sickle hemoglobin.
Frequency of the MTHFR C677T polymorphism was not found to be higher among our patients. Homozygous 677T mutation was observed in 0.6% of patients when compared to 3% in normals (Table 3).
Distribution of C and T allele of MTHFR (P Value = .213).
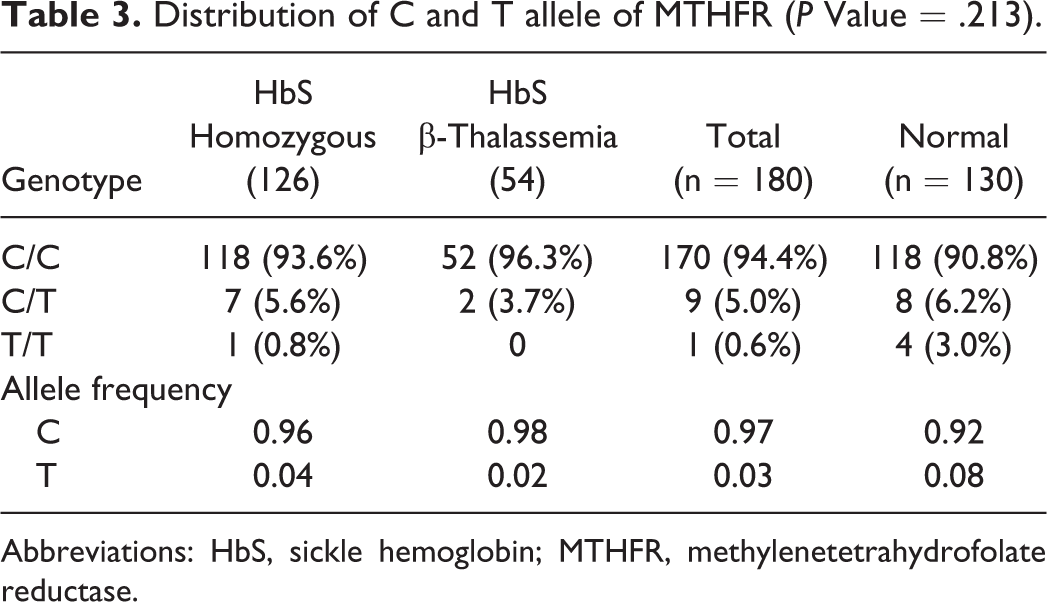
Abbreviations: HbS, sickle hemoglobin; MTHFR, methylenetetrahydrofolate reductase.
Discussion
The SS anemia is characterized by a hypercoagulable state with increased generation of thrombin and fibrin, as well as platelet activation, which leads to increased risk of thromboembolic complications. Important causes of mortality in patients with SS disease are related to vascular occlusion. This suggested that management of SS disease complications would be possible by manipulating hemostasis pharmacologically. 7
The role of inherited thrombophilia in the pathogenesis of SS thrombosis has been reported in various studies. The frequency of FVL, prothrombin G20210A, and thermolabile MTHFR C677T mutations and their association with incidence and recurrence of thromboembolism in patients with SS disease have been studied in different populations. 6,7,12–14
The FVL is a single-point mutation involving a guanine to adenine transition at position 1691 in exon 10 of the factor V gene. According to the studies performed in Southern Iranian patients with SS disease, heterozygous FVL was found in 14.3% of patients who were sickle homozygous, 13.3% of sickle heterozygotes, 10% of patients with HbS β-thalassemia, and 1.6% of the controls. Increased prevalence of the FVL in sickle heterozygotes and patients with HbS β-thalassemia was statistically significant compared to controls. However, a significant correlation was observed between FVL and SS anemia in patients with sickle homozygous. 6
Many studies have reported a low frequency of thrombophilic mutations in patients with SS disease and the lack of association between these mutations and risk of thromboembolism. In Eastern Saudi Arabia, the prevalence of the FVL mutation and the prothrombin G20210A mutation were similar in patients and controls (P = .174 and P = .397, respectively). However, an increased prevalence of the MTHFR 677T/T genotype was seen among patients, although this was also not statistically significant (P = .217). 12
In another study done by Andrade et al, contradictory results were found among patients with SS disease from Brazil. Previously, they had reported heterozygosity for FVL and prothrombin variant and homozygosity for MTHFR-T to be common among a nonselected population of Brazil, whereas increased prevalence was observed among the patients with vascular disease. 15 However in a later study, no distinct increased prevalence of these risk factors was found. This may be because of the highly heterogeneous Brazilian population. 7
Filho et al also recently carried out a study on the Brazilian population to examine possible genetic risk factors responsible for cerebrovascular disease in patients with SS disease. Apart from FVL, prothrombin G20210A, and thermolabile MTHFR C677T polymorphisms, they also studied the frequency of the βS-globin gene haplotypes and coinheritance of α-thalassemia. The frequency of the –α3.7 kb deletional α-thalassemia was similar in patients and controls (P = .751) Children with the Bantu/Atypical βS-globin gene haplotype had a 15 times greater chance of cerebrovascular disease than children with other βS-globin gene haplotypes. They also found the frequency of the MTHFR C677T polymorphism to be similar in patients and controls. However, the FVL and prothrombin gene mutations were found to be absent. 13
Hatzlhofer et al compared 2 groups of patients with SS disease with and without vascular complications. No significant associations were found between the groups for MTHFR A1298C, Factor V G1691A, or prothrombin G20210A mutation. However, the 677CT and TT genotypes showed a significant risk of vascular complications possibly predictive for the development of vascular complications in patients with SS anemia. 16
Kutlar et al tried to elucidate the role of the MTHFR polymorphism in increased risk of avascular necrosis in SS disease. The frequency of the 677T mutation was 35.6% in patients with avascular necrosis and 12.9% in those without avascular necrosis (P = .006). They suggested that the thermolabile MTHFR variant may be a contributing risk factor for avascular necrosis in some populations with SS disease. 17
Homozygosity for the MTHFR gene C677T polymorphism may cause hyperhomocysteinemia, which, in patients with homozygous SS disease, may increase the risk to develop stroke. Cumming et al studied the role of the MTHFR C677T polymorphism in patients with SS disease with stroke. However, they did not find any association. 18 In our study, we had only 1 patient with SS disease with stroke, and the MTHFR C677T polymorphism was found to be absent.
As India is a big country with a diverse population, the prevalence of FVL and MTHFR C677T shows variable distribution in different regions. Khare et al showed that FVL was absent, whereas heterozygous MTHFR C677T was seen in 14% of normal individuals from western India. 19 Similar findings have also been reported by Vora et al in western India. 20 However, the prevalence of FVL in healthy school children from the Parsi community in western India was 10.5% in the heterozygous state and 2.2% in the homozygous state. 21 On the other hand, Das et al and Angeline et al found the prevalence of FVL in normal populations from north India and south India to be 1.9% and 5.5%, respectively, 22,23 whereas Kumari et al showed that, in eastern India the MTHFR C677T polymorphism in the heterozygous the homozygous states was present in 21.3% and 1.1%, respectively, of normal individuals. 24 All our patients were from the western Indian region.
In the Asian Indian population, although SS disease is very common among the tribal populations and some nontribal groups in western, central, and part of eastern India, there is only 1 report from north India, where Pandey et al found a low impact of these inherited hypercoagulability risk factors on the pathogenesis of SS disease and sickle β-thalassemia. 25
Among the risk factors we studied in patients from western India, a low prevalence of the FVL mutation and homozygosity for the MTHFR-T was observed. This suggested that an inherited hypercoagulability risk factor does not play a major role in the pathogenesis of SS disease and its complications in our population. Thus, the study of these risk factors did not allow the identification of patients with SS disease having a high risk of occlusive vascular complications.
Footnotes
Acknowledgments
We are thankful to Dr Shrimati Shetty and Dr Bipin Kulkarni for providing the PCR primers and protocol and West Bengal University of Health Sciences, Kolkata, for their support. We acknowledge the Indian Council of Medical Research, New Delhi, for financial support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for authorship, and/or publication of this article.