
Abstract
The aim of the study was to assess the factors associated with the anticoagulation treatment in patients with atrial fibrillation (AF). A total of 2242 consecutive patients who had been admitted with AF on their electrocardiogram were included in the study. After excluding valvular AF, 1745 patients with nonvalvular AF were analyzed. Mean CHA2DS2-VASc score [cardiac failure, hypertension, age ≥ 75 (doubled), diabetes, stroke (doubled), vascular disease, age 65 -74 and sex category (female)], frequency of persistent/permanent AF, hypertension, diabetes mellitus (DM), stroke history, body mass index, and left atrial diameter were significantly higher in patients receiving anticoagulant therapy. Stroke history, persistent/permanent AF, hypertension, DM, age, heart failure, and left atrial diameter were independent predictors of warfarin prescription. Labile international normalized ratio was the only independent negative predictor of effective treatment with warfarin. In this study, we demonstrated that stroke history, persistent/permanent AF, hypertension, DM, and left atrial diameter were positive predictors, whereas advanced age and heart failure were negative predictors of oral anticoagulant use in patients with nonvalvular AF.
Introduction
Atrial fibrillation (AF) is the most common cardiac arrhythmia in clinical practice, with an overall prevalence of 1% to 2% in the adult population. 1 The increasing prevalence of AF made this arrhythmia one of the most important reasons for cardiovascular morbidity and mortality. 2 The prognosis of the patients with AF varies widely depending on the presence of thromboembolic events that can be prevented by anticoagulation therapy. 3 Therefore, the current guidelines recommend anticoagulant treatment in patients with moderate to high risk of thromboembolic events. 1 These patients have high scores, a score evaluation system using a 9-point scale (9-point score evaluation) derived as CHA2DS2-VASc acronym [cardiac failure, hypertension, age ≥ 75 (doubled), diabetes, stroke (doubled), vascular disease, age 65 -74 and sex category (female)]. 4 Current anticoagulation treatment is based on the CHA2DS2-VASc score, the age and sex of the patient, and the type of AF. 1 Our aim was to assess the factors associated with the anticoagulation treatment and its determinants in a large multicenter cohort of patients with AF.
Methods
Study Population
Atrial Fibrillation in Turkey: Epidemiologic Registry (AFTER) is a prospective, multicenter study designed with the aim of describing the prevalence and epidemiology of AF in Turkey. 5 A total of 2242 patients were recruited in 17 referral hospitals, reflecting all the population of the 7 geographical regions of Turkey. The inclusion criteria were determined as “all consecutive patients over 18 years of age who had applied to the cardiology outpatient clinics except emergency room with at least one attack of AF identified on electrocardiographic examination.” Patients who refused to be included in the study or not signed the consent form were excluded from the study. Data regarding demographic, echocardiographic, and biochemical variables and physical examination were collected via a standard questionnaire by the cardiologists. The study was approved by the Dicle University ethics committee, which was the main center of the study. Every patient signed an informed consent.
Definitions
The CHA2DS2-VASc score was based on a 9-point system in which 2 points are assigned for a history of stroke or transient ischemic attack and for age ≥75 years and 1 point each is assigned for a history of hypertension, diabetes, or recent cardiac failure, age between 65 and 74 years, vascular disease (previous myocardial infarction, peripheral artery disease, or aortic plaque), and female gender. 4
The Hypertension, Abnormal renal/liver function, Stroke, Bleeding history or predisposition, Labile International Normalized Ratio, Elderly, Drugs/alcohol (HAS-BLED) score was assessed by adding (as the addition of) 1 point for each of the following factors: systolic blood pressure >160 mm Hg, abnormal liver or renal function, stroke, bleeding history or predisposition, labile international normalized ratio (INR), age >65 years, concomitant treatment with nonsteroid anti-inflammatory drugs, or alcohol abuse. 6
According to the European Society of Hypertension/the European Society of Cardiology guidelines, hypertension was defined as 2 blood pressure readings higher than 140/90 mm Hg or the presence of specific treatments with a previous diagnosis. 7 Individuals with diabetes mellitus (DM) were diagnosed according to the criteria of the American Diabetes Association, namely, when fasting plasma glucose level was >126 mg/ dL, hemoglobin A1C level was found as >6.5%, a casual plasma glucose level was found as >200 mg/dL along with the classic symptoms of hyperglycemia, and/or the current use of diabetes medication. 8 Routine echocardiographic examination was performed in all the patients.
Effective INR range was defined as an INR of 2.0 to 3.0. Labile INR was defined as unstable/high INRs or poor time in therapeutic range of <60%. 6
Statistical Analysis
Statistical Package for Social Sciences software (SPSS 15, Chicago, Illinois) was used for analysis. Descriptive parameters were shown as mean ± standard deviation or in percentages. Two-sided t tests and chi-square tests were used to analyze the differences in means and proportions between the groups. Abnormally distributed variables were compared using Mann-Whitney U test. Multiple logistic regression analysis was applied to identify variables that had an independent relationship with anticoagulant therapy and effective INR. A P value of <.05 was considered significant.
Results
The results of the study were derived from the baseline recordings of the AFTER cohort. After excluding valvular AF, 1745 patients with nonvalvular AF were analyzed. The demographic and clinical characteristics of the study population according to the prescription of anticoagulant treatment are shown in Table 1. In all, 40% of the patients were receiving warfarin. The number of patients using anticoagulant and antithrombotic therapy is shown in Figure 1. Mean CHA2DS2-VASc score, frequency of persistent/permanent AF, hypertension, DM, stroke history, body mass index, and left atrial diameter were significantly higher in patients receiving anticoagulant therapy.
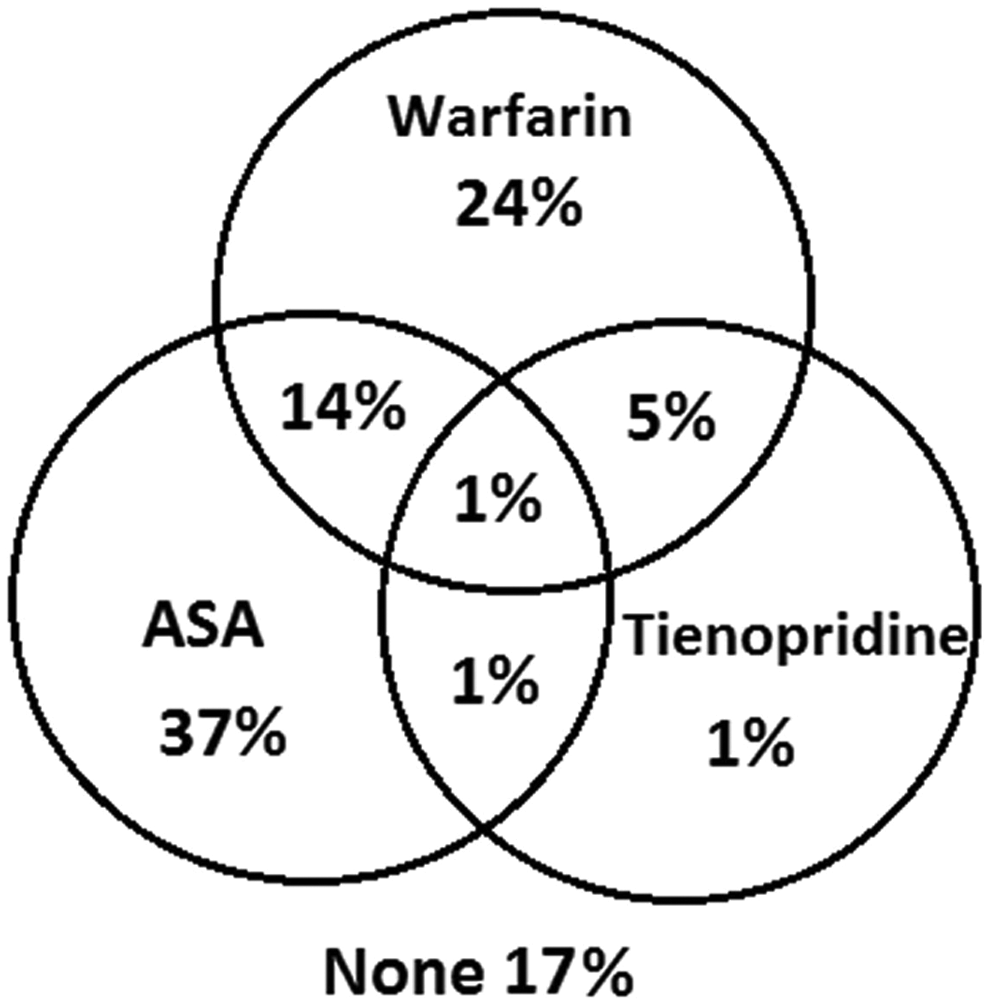
The number of patients using anticoagulant and antithrombotic therapy.
Baseline Demographic Characteristics of the Patients.a
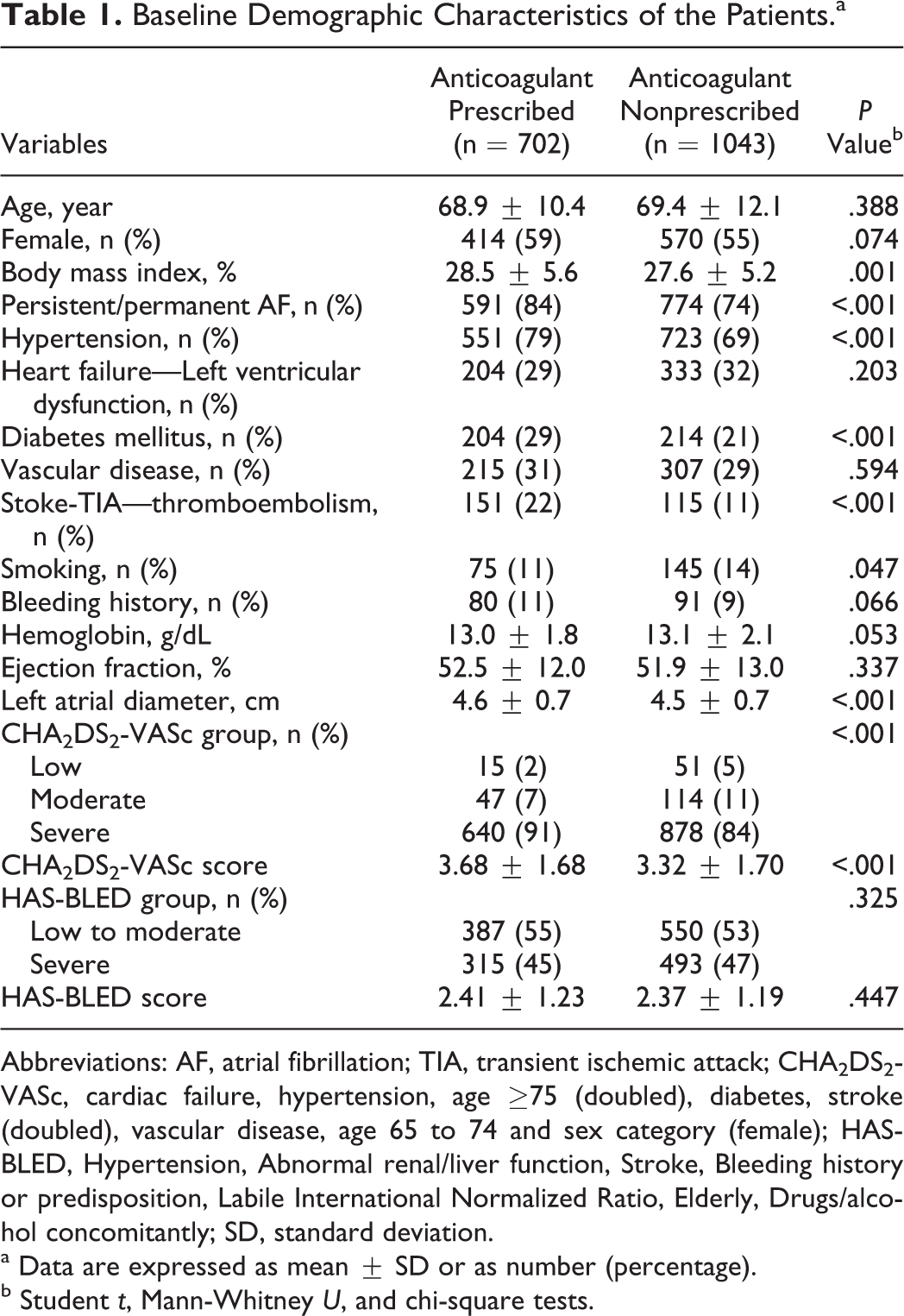
Abbreviations: AF, atrial fibrillation; TIA, transient ischemic attack; CHA2DS2-VASc, cardiac failure, hypertension, age ≥75 (doubled), diabetes, stroke (doubled), vascular disease, age 65 to 74 and sex category (female); HAS-BLED, Hypertension, Abnormal renal/liver function, Stroke, Bleeding history or predisposition, Labile International Normalized Ratio, Elderly, Drugs/alcohol concomitantly; SD, standard deviation.
a Data are expressed as mean ± SD or as number (percentage).
b Student t, Mann-Whitney U, and chi-square tests.
Independent predictors of warfarin use were analyzed by multivariate regression analysis. Stroke history, persistent/permanent AF, hypertension, DM, age, heart failure, and left atrial diameter were independent predictors of warfarin prescription (Table 2).
Multivariate Logistic Regression Analysis of the Warfarin Use.
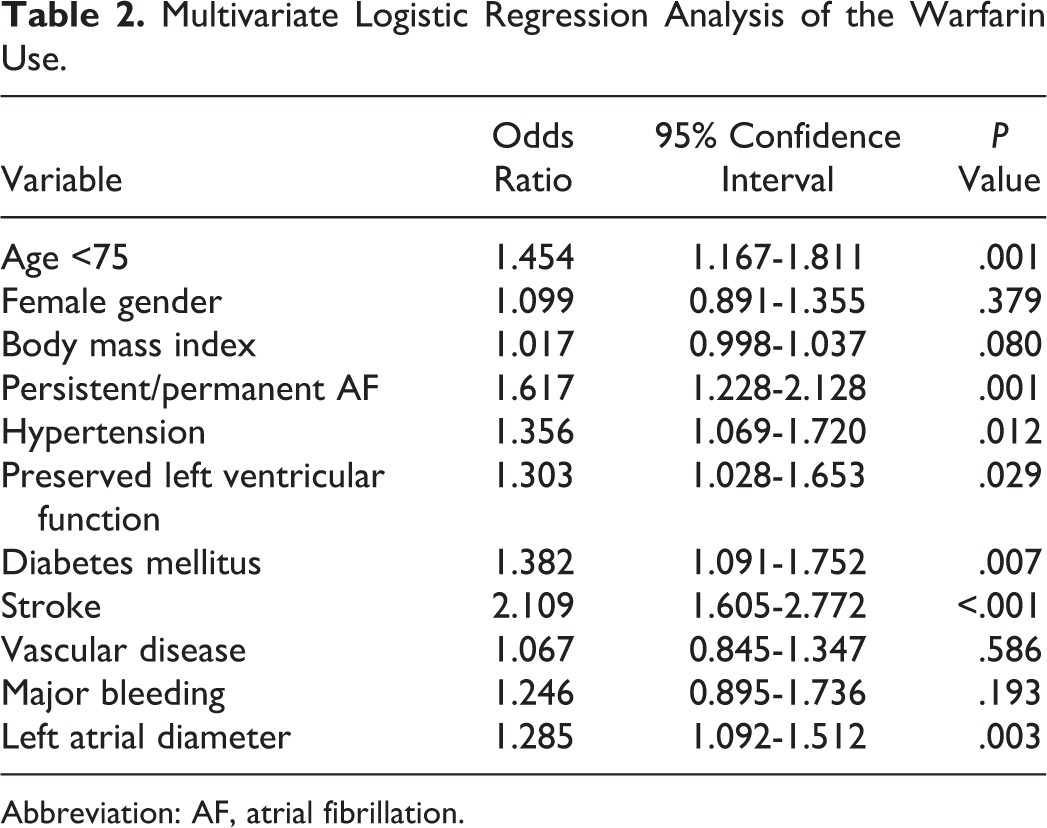
Abbreviation: AF, atrial fibrillation.
Among the warfarin users, the effective INR was found as 39%. Predictors of effective INR were also analyzed. Labile INR value was the only independent negative predictor of the effective treatment with warfarin (odds ratio = 0.618, 95% confidence interval = 0.401-0.953, P = .029; Table 3).
Multivariate Logistic Regression Analysis of the INR Effectivity.
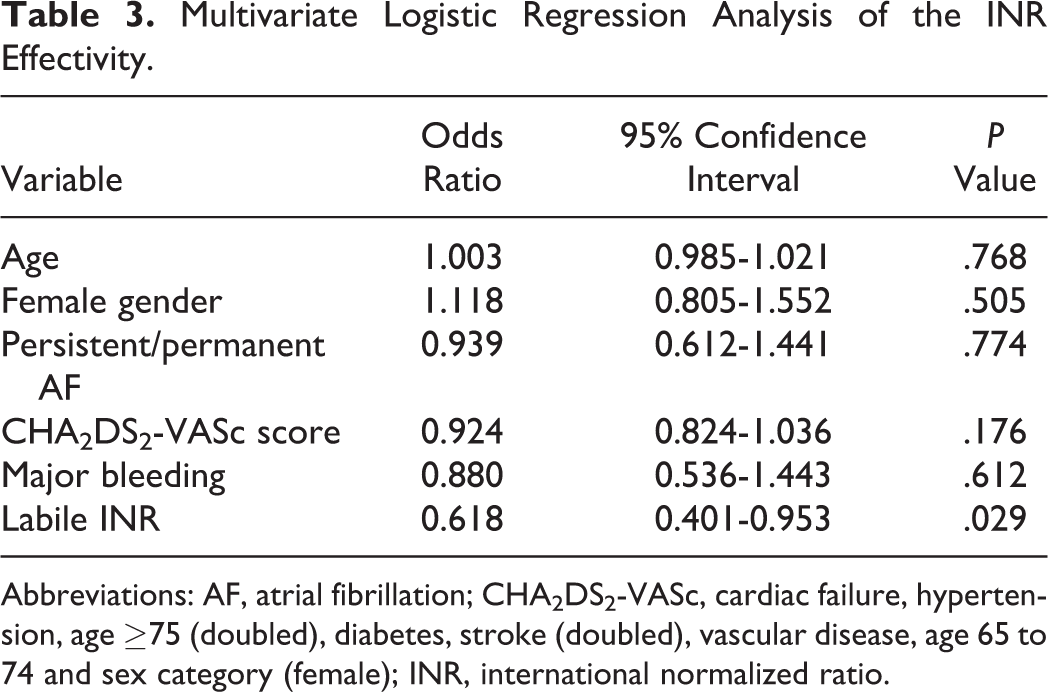
Abbreviations: AF, atrial fibrillation; CHA2DS2-VASc, cardiac failure, hypertension, age ≥75 (doubled), diabetes, stroke (doubled), vascular disease, age 65 to 74 and sex category (female); INR, international normalized ratio.
Discussion
Our study revealed that 40% of the patients in the cohort study received anticoagulant therapy. The prescription of anticoagulant therapy was mostly associated with the CHA2DS2-VASc score components except vascular disease and female sex category. On the other hand, steady-state INR value was the only independent predictor of effective treatment with warfarin.
Numerous randomized controlled trials of warfarin therapy have demonstrated that oral anticoagulant therapy can reduce the risk of ischemic stroke by approximately 68% in patients with nonvalvular AF. 9,10 Despite this conclusive evidence of efficacy, numerous studies have shown that warfarin prescription in patients with AF is suboptimal in real-world practice. 11,12 Recently, in their meta-analysis, Baczek et al 13 reported that the frequency of warfarin use across studies ranged from 9.1% to 79.8% (median = 49.1%). Warfarin therapy necessitates close follow-up by the physician because of the narrow therapeutic index that is influenced by multiple factors. There are also potential barriers related to the patients’ compliance and health care system. 14 The underprescription of warfarin is the result of the complex nature of the drug. Reviews and meta-analyses that have been conducted in order to more completely identify prescriber and patients’ characteristics associated with warfarin prescription have various results. Pugh et al 15 showed that increasing age, increased bleeding risk, previous bleeds, fall risk, and comorbidities were the barriers to anticoagulation. On the other hand, Baczek et al 13 reported that alcohol/drug abuses were perceived as barriers to compliance and contraindications for warfarin, including dementia, falls, gastrointestinal hemorrhage, intracranial hemorrhage, hepatic and renal impairment, advanced age, were associated with significant reductions in warfarin use. Stroke history, persistent/permanent AF, hypertension, DM, age <75, heart failure, and left atrial diameter were independent predictors of warfarin prescription in the present study. However, almost all of the studies have common negative predictors, for example, advanced age and increased bleeding risk, and positive predictors, for example, stroke. We have previously shown that a history of stroke, high income level, the presence of persistent and permanent AF, and younger age were independent predictors in our single-center survey. 16 Bertomeu-González et al 17 showed that all the variables included in the CHADS2 risk score were associated with the anticoagulant prescription.
Age was the mainly evaluated patient characteristic in previous studies. Almost every investigation showed that there were significant reductions in warfarin use, with increasing or advanced (>80) age. 11,12,15,16,18 Similarly, thromboembolic event history was another common predictor of anticoagulant prescription. Furthermore; Agarwal et al 11 found a statistically significant relationship between CHADS2 score and warfarin use in their study conducted among 44 193 patients. In our analysis, among the CHA2DS2-VASc components, age, DM, hypertension, and stroke were independent predictors of warfarin prescription. Trends were observed in the meta-analysis conducted by Baczek et al 13 regarding hypertension and diabetes (P = .06 and .13, respectively). However, heart failure was a negative predictor of warfarin use in our country, although it is a part of the CHA2DS2-VASc risk score. It can be related to statistical chance or a tendency of physicians’ preference for prescribing warfarin in patients with preserved left ventricular function.
Our analysis showed a 1.6-fold increased odds of receiving warfarin in patients with persistent/permanent AF. Similarly, Waldo et al 19 demonstrated a 1.8-fold increase in warfarin prescription in these patients.
One of the most important findings of the current study is the detection of left atrial diameter as an independent predictor of warfarin use. To our knowledge, we are the first to analyze and report an echocardiographic variable as a determinant of warfarin prescription. Each centimeter of increase in left atrial diameter was associated with an increase in 28% of warfarin prescription. One of the possible reasons of this finding is the extensive use and higher reliability of this measurement. In our country, echocardiographic measurements are directly performed by cardiologists without any assistance of technicians.
We further analyzed the independent predictors of the INR effectivity. Labile INR was the single independent negative predictor of a steady-state INR regarding other important covariates such as age, sex, CHA2DS2-VASc score, AF type, and major bleeding. Although not surprising, it underlines the important barrier pertaining to warfarin. Therefore, novel anticoagulants will be welcomed in real-world practice against stroke prevention. 20
Conclusion
In this cohort study, we revealed that anticoagulant therapy was applied to 40% of the patients in the study. The prescription of anticoagulant therapy was mostly associated with the CHA2DS2-VASc score components except vascular disease and female sex category. On the other hand, a labile INR was the only independent negative predictor of effective treatment with warfarin.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.