
Abstract
Right ventricular dysfunction (RVD) defined by echocardiography and/or by natriuretic peptides is a well-known predictor of prognosis in patients with pulmonary embolism (PE). This study investigated carbonic anhydrase IX (CA IX) levels for predicting echocardiographic RVD in patients with PE. A total of 150 normotensive patients with PE were included. The levels of CA IX, N-terminal pro-brain-type natriuretic peptide (NT-proBNP), and high-sensitive cardiac troponin T were significantly elevated in patients with PE with RVD on echocardiography. A receiver–operating characteristic curve analysis showed a value of 0.751 for CA IX, 0.714 for NT-proBNP, and 0.650 for high-sensitive troponin-T to predict RVD on echocardiography. The cutoff value to predict RVD was 32.45 pg/mL for CA IX (sensitivity: 89.3% and specificity: 51.1%). There was a significant positive correlation between the CA IX level and the systolic pulmonary arterial pressure on echocardiography (ρ = .21; P = .035). The CA IX is a significant serologic predictor of RVD in acute PE and correlates with systolic pulmonary arterial pressure.
Introduction
The short-term prognosis and risk stratification of pulmonary embolism (PE) are associated with the hemodynamic status and underlying diseases. 1,2 It has been suggested that patients with PE should be classified according to hemodynamic parameters, presence of right ventricular dysfunction (RVD), and myocardial injury. 3 Those named as high-risk patients are diagnosed in the presence of shock or persistent systemic hypotension (defined as a systolic blood pressure < 90 mm Hg or a pressure decline of ≥40 mm Hg for 15 minutes if not due to new-onset arrhythmia, hypovolemia, or sepsis). The patients with PE identified as normotensive patients are classified as nonhigh-risk patients with PE, whereas the presence of markers of RVD 4 and/or myocardial injury 5 identify intermediate-risk patients with PE. It is more likely that patients with PE at intermediate risk with markers of RVD and myocardial injury are at greater risk than patients with discordant results. 3 Therefore, RVD, defined by echocardiography and/or by natriuretic peptides, is a well-known predictor of early mortality and provides critical clinical information for risk stratification or management of acute PE. 3,4,6 –9
Carbonic anhydrases (CAs) are a large family of zinc metalloenzymes, which catalyze the reversible hydration of carbon dioxide. The CA IX is a transmembrane glycoprotein with an active extracellular enzyme site, and it has been shown previously that CA IX is hypoxia inducible and is considered to be one of the best cellular biomarkers of hypoxia. 10 The presence of CA IX in plexiform lesions of patients with idiopathic pulmonary arterial hypertension has been demonstrated. 11 It was also shown that pulmonary arteries in an emphysematous lung showed increased remodeling and CA IX expression in association with hypoxia. 12 RVD appears secondary to increased pulmonary arterial pressure, which is induced by abnormal hypoxic vasoconstriction of pulmonary artery following PE. 13 The CA IX as one of the best cellular biomarkers of hypoxia may play a role in this interaction. The present study is to investigate whether CA IX is associated with RV dysfunction due to PE and to investigate the optimal cutoff values of CA IX for predicting RV dysfunction in patients with acute PE. In addition, the N-terminal pro-brain-type natriuretic peptide (NT-proBNP) and high-sensitive troponin-T have been investigated for the prediction of RVD.
Materials and Methods
Study Design and Patient Settings
The present study was a single-center study, and the investigation conforms to the principles outlined in the Declaration of Helsinki. The study was approved by the local ethics committee. The study was conducted at a university hospital, a tertiary care hospital, that serves as a primary referral center for patients with suspected PE. Consecutive patients presenting with clinically suspected PE, referred for diagnostic work-up, were eligible for this study. Only patients with objectively confirmed PE on the basis of the presence of PE on spiral computed tomography angiography were included. All the patients with massive PE with hemodynamical instability defined by the European Society of Cardiology (ESC) as a systolic blood pressure < 90 mm Hg or a pressure drop of ≥40 mm Hg for >15 minutes if not caused by new onset arrhythmia hypovolemia or sepsis were excluded. 3 Therefore, according to the ESC guidelines, all the patients with PE who met the criteria of submassive (intermediate risk) or nonmassive PE (low risk) category were included in the present study. Because malignancies particularly renal cell carcinomas can result in elevated CA IX, we excluded patients with active malignancies having the potential to increase CA IX. We also excluded patients with acute myocardial infarction and overt congestive heart failure having the potential to affect NT-proBNP, high-sensitive troponin-T, and RVD.
Blood Samples and Laboratory Methods
Venous plasma samples were collected on admission and immediately stored at −80°C. Samples were later analyzed in batches after a single thaw. Levels of human serum CA IX (CA IX) were determined by an enzyme-linked immunosorbent assay kit (Catalog No. DCA 900; R&D systems, China), according to the manufacturer’s protocols. The absorbance of the samples was measured at 450 nm using a VersaMax tunable microplate reader (Molecular Devices, California). The results were expressed as pg/mL. The minimum detectable dose of human CA IX is typically less than 2.28 pg/mL.
High-sensitive troponin T and NT-proBNP were measured by an electrochemiluminescence immunoassay using Elecsys 2010 (Roche Diagnostics, Mannheim, Germany) according to the manufacturer’s protocol. According to the manufacturer, the NT-ProBNP test has an intra-assay coefficient of variation of 0.8–3% and a detection range of 5 to 35 000 pg/mL.
Investigations
All consecutive patients in whom the diagnosis of PE had been made underwent echocardiographic examination. All patients were examined by 2-dimensional, pulse-wave Doppler echocardiography within the first 24 hours after a diagnosis of PE, using a Vivid 7 (GE Vingmed Ultrasound, Horten, Norway) with a 2.5-MHz transducer. The transthoracic echocardiography (TTE) examinations by an experienced echocardiographer were blinded to the results of biochemical assays and were also blinded to the results of the patients’ data. Right ventricular function was evaluated by TTE, and RVD was diagnosed in the presence of any of the following: dilatation of the right ventricle (diastolic diameter > 30 mm), right ventricle/left ventricle diameter ratio > 1, abnormal motion of the interventricular septum, hypokinesis of right ventricle, or tricuspid valve regurgitation (jet velocity > 2.5 m/s). 2,3
Statistical Analyses
The Kolmogorov-Smirnov test was used to test for normal distribution of continuous variables. Data characterized by a normal distribution were expressed as mean values followed by standard deviation. Parameters without such a distribution were expressed as median with interquartile range. Student test (normal distribution) or Mann-Whitney test (nonnormal distribution) were used to compare the 2 groups. The investigation for a diagnostic cutoff value was based on receiver–operating characteristic (ROC) curves. Multivariate regression analysis was used in a stepwise descending method from prognostic factors with significance <0.1 at univariable analysis. Results are given as odds ratios (95% confidence interval), and P < .05 was considered statistically significant. Data were analyzed using SPSS statistical software (version 13.01, serial number 9069728; SPSS Inc, Chicago, Illinois).
Results
Overall, 150 normotensive patients with acute PE were included in the study. The baseline clinical characteristics of the study patients are summarized in Table 1. All the diagnoses of PE were confirmed by contrast-enhanced multidetector computed tomography. All the patients were normotensive, and none of them required ventilatory support. Overall, a transthoracic echocardiogram was performed in 106 (75.0%) patients; of these, 75 (70.7%) patients were diagnosed with RVD.
Baseline Clinical Characteristics of Pulmonary Embolism Patients.a
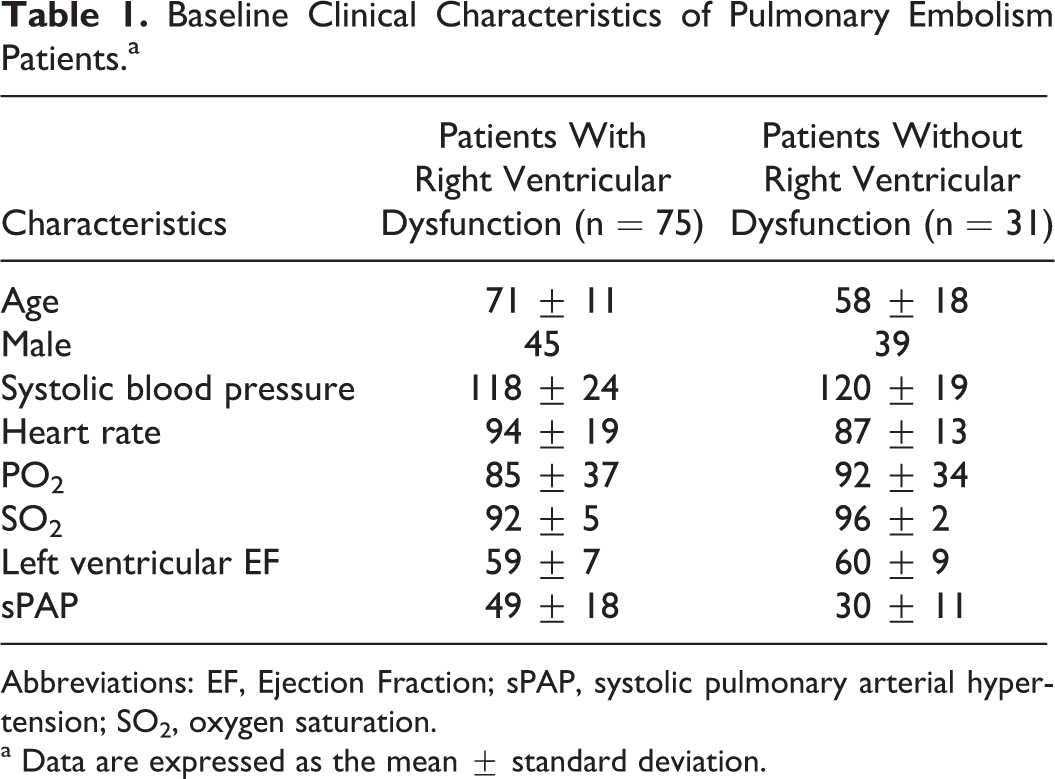
Abbreviations: EF, Ejection Fraction; sPAP, systolic pulmonary arterial hypertension; SO2, oxygen saturation.
a Data are expressed as the mean ± standard deviation.
The levels of CA IX, NT-proBNP, and high-sensitive troponin-T were significantly elevated in the patients with PE with RVD relative to the patients with PE without RVD (Table 2). By the ROC curve analysis, the area under the curve to predict RVD on echocardiography was 0.751 for CA IX, 0.714 for NT-proBNP, and 0.650 for high-sensitive troponin-T (Figure 1). The optimal cutoff values to predict RVD were 32.45 pg/mL for CA IX (sensitivity: 89.3% and specificity: 51.1%), 530 pg/mL for NT-proBNP (sensitivity: 80% and specificity: 47%), and 0.013 ng/mL for high-sensitive troponin T (sensitivity: 81.1% and specificity: 48.4%), respectively. The CA IX showed a significant positive correlation with systolic pulmonary arterial pressure on echocardiography (ρ = .21; P = .035; Figure 2).
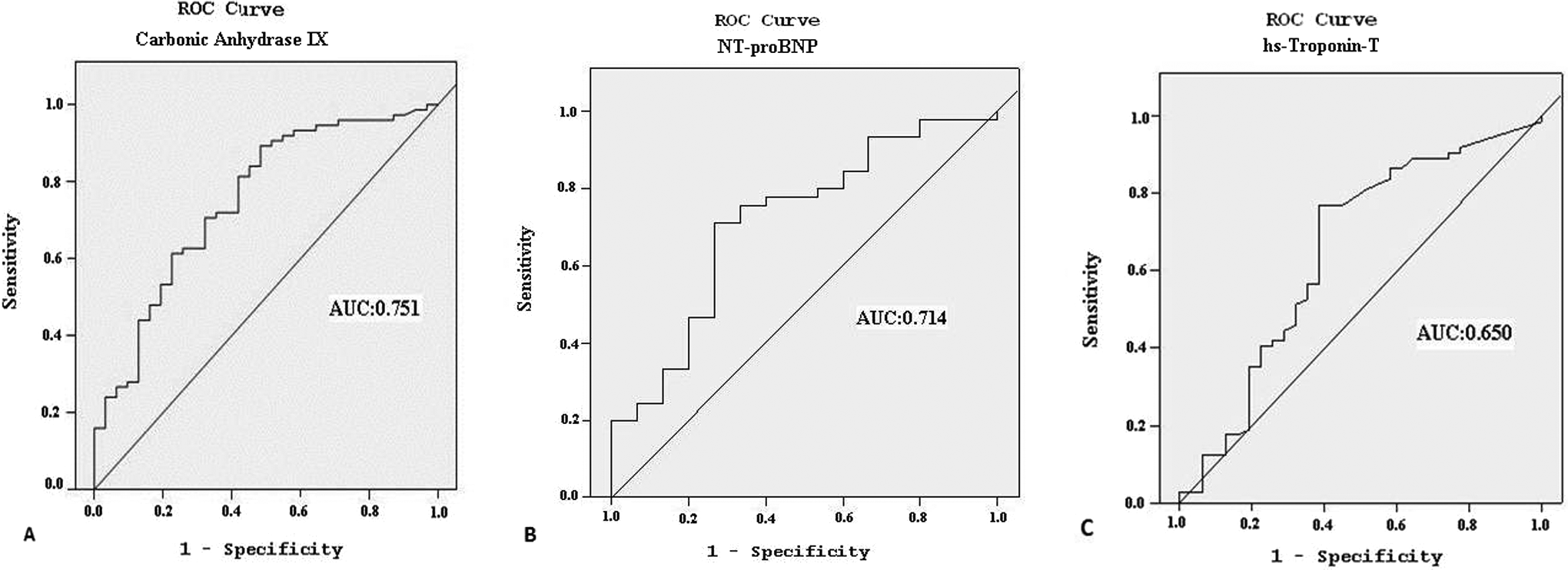
Receiver–operating characteristic curve analyses for (A) carbonic anhydrase IX, (B) NT-proBNP, and (C) high-sensitive Troponin-T to predict right ventricular dysfunction on echocardiography. NT-proBNP indicates N-terminal-pro-brain-type natriuretic peptide; hs-troponin-T: high-sensitive troponin-T.
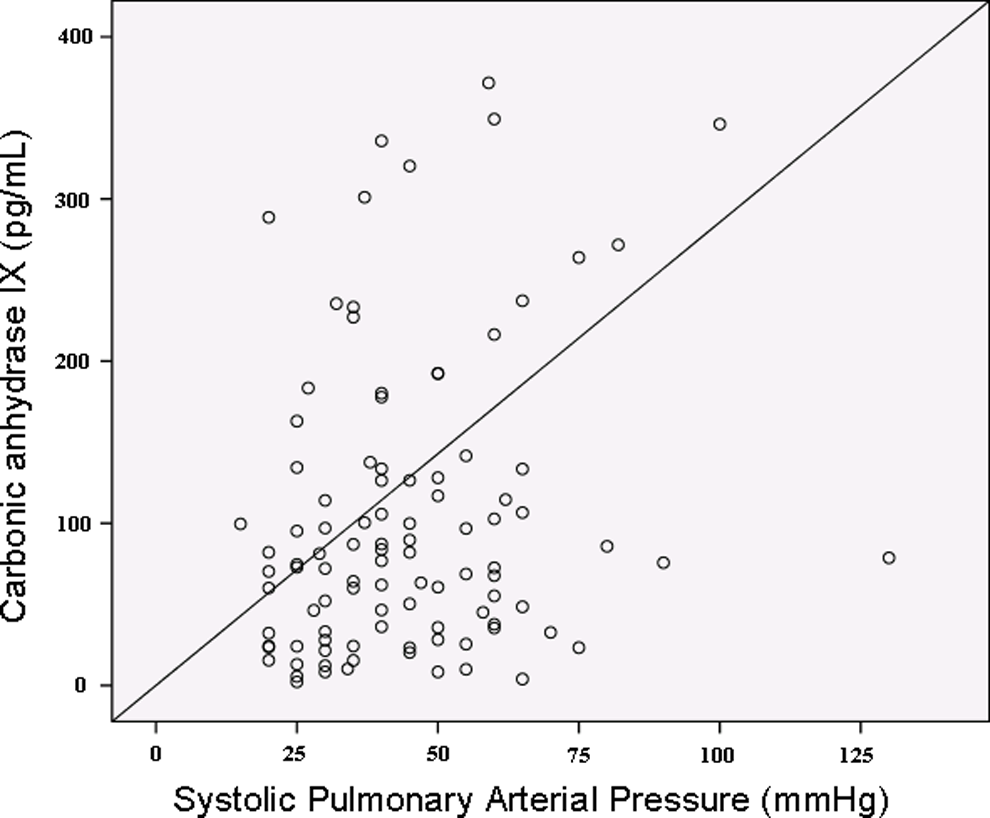
Correlation between carbonic anhydrase IX and the echocardiographic systolic pulmonary hypertension.
Comparison Between Biomarkers and RVD on Echocardiography.a
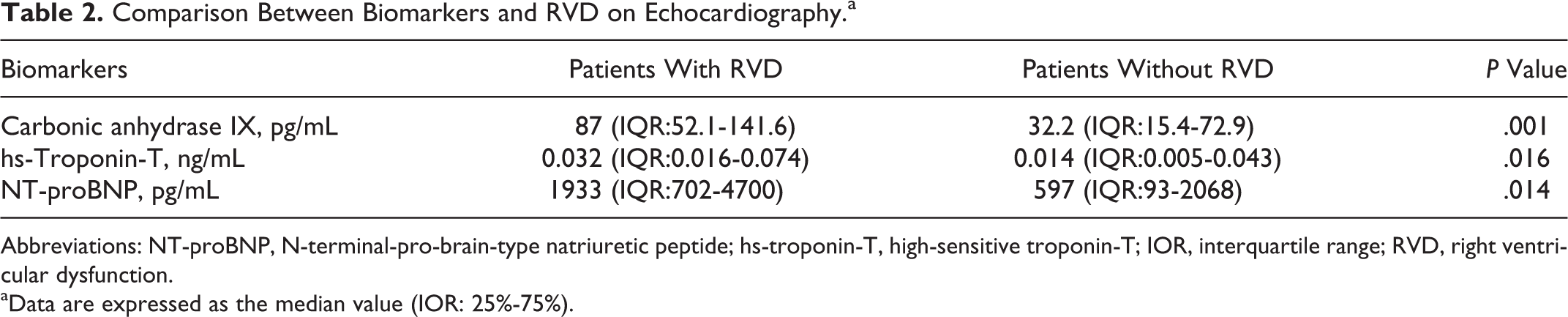
Abbreviations: NT-proBNP, N-terminal-pro-brain-type natriuretic peptide; hs-troponin-T, high-sensitive troponin-T; IOR, interquartile range; RVD, right ventricular dysfunction.
aData are expressed as the median value (IOR: 25%-75%).
In the univariate analysis, a significant association was revealed between RVD on echocardiography and age, heart rate > 110/min, CA IX (cutoff = 32.45 pg/mL), NT-proBNP (cutoff = 530 pg/mL), and high-sensitive troponin T (cutoff = 0.013 ng/mL).
Multivariate logistic regression analysis was performed to identify the independent predictors of RVD on echocardiography. The CA IX was >32.45 pg/mL, and age were significant independent predictors of RVD after the adjustment for the baseline characteristics (Table 3).
Predictor of Echocardiographic Right Ventricular Dysfunction by Multivariate Logistic Regression Analysis.
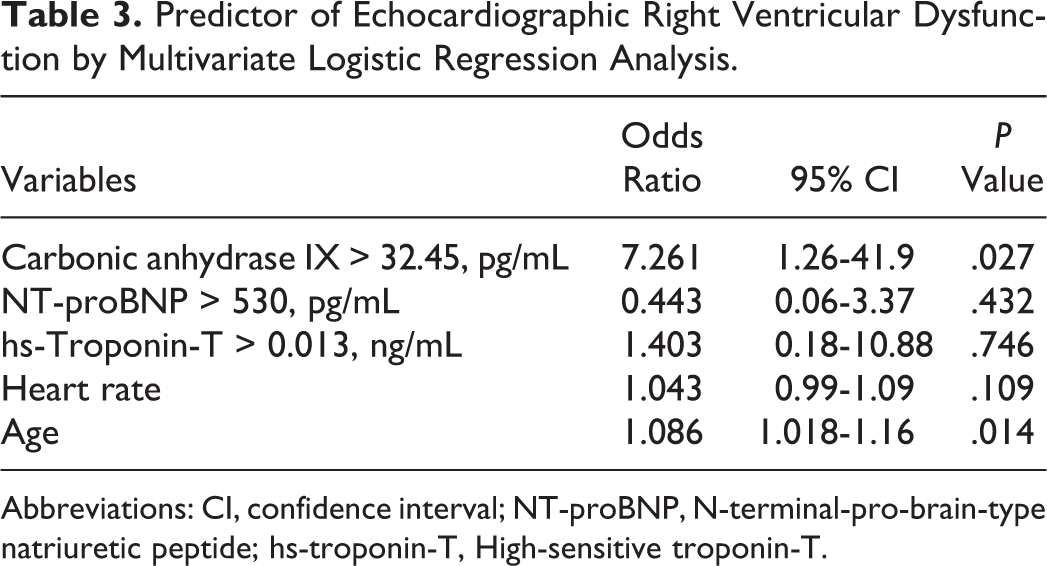
Abbreviations: CI, confidence interval; NT-proBNP, N-terminal-pro-brain-type natriuretic peptide; hs-troponin-T, High-sensitive troponin-T.
Discussion
Approximately 80% of patients with PE present with normal systemic blood pressure. 6 The RVD on echocardiography is an independent and important predictor of mortality in patients with acute PE, regardless of hemodynamic status. 1 However, echocardiographic criteria of RVD differ among published studies and include dilatation of right ventricle, hypokinesis of right ventricle, increased right ventricle/left ventricle diameter ratios, and increased tricuspid jet velocities. 4,7 Therefore, normotensive patients with PE have a variable frequency of RVD on echocardiography that is between 27% and 70%. 6,8,14 –17 This variable frequency of RVD is mainly due to the different criteria of RVD on echocardiography in patients with PE. It is not known which of these criteria is the most sensitive to define RVD due to PE and which, if any, correlates best with the patient’s prognosis. 4 There is also a limitation about the echocardiography, because echocardiography largely depends on the experience of the operator and accurate identification of RVD, which needs an expert cardiologist in echocardiography. Furthermore, echocardiography with an expert cardiologist is not always readily available, especially in emergency settings. Therefore, there is an obvious need to define RVD by easily applied serological biomarkers. Recent studies propose that brain-type natriuretic peptide (BNP) or NT-proBNP as markers of RVD, released by myocardial stretching, provide prognostic information in addition to that derived from echocardiographical measurement of RVD. 18,19 Although elevated BNP or NT-proBNP concentrations are associated with a worse prognosis, the positive predictive value of these biomarkers has been reported as being between 12% and 26%. However, it has been proposed that low levels of BNP or NT-proBNP can be reliably used to define patients with PE that have a good prognosis with a negative predictive value of 94% to 100%. 3,20 –25
The main finding of the present study was that the levels of NT-proBNP, high-sensitive troponin-T, and CA IX were significant predictors of echocardiographic RVD. It can be expected that simple measurements of CA IX in addition to cardiac biomarkers can be useful to predict the presence of RVD, especially in hospital settings where echocardiographic examinations and experts in echocardiography are not readily available. The measurement of cardiac biomarkers can be a simple and useful method as an alternative to echocardiography. The NT-proBNP and conventional cardiac troponin-T have been shown to be associated with RVD and the prognosis of PE. Most of the troponin assays studied in the literature as predictors of RVD and for the prognosis of PE are conventional cardiac troponin-T assays.
18,26
–28
In addition to NT-proBNP and troponin-T, in the present study, we have also studied a new marker named CA IX for the prediction of RVD based on echocardiography, and it was found that the level of CA IX was significantly elevated in patients with PE with RVD compared to patients with PE without RVD. Both in univariate and multivariate analysis CA IX was significantly associated with RVD.
The CA IX belongs to the group of genes most responsive to hypoxia and has therefore been proposed as an intrinsic marker of hypoxia. 33 The presence of CA IX in plexiform lesions of patients with idiopathic pulmonary arterial hypertension and in pulmonary arteries in emphysematous lungs in association with hypoxia has been shown previously. 11,12 Hypoxia-induced expression of CA IX in cardiomyocytes has also been proposed to have particular importance for the study of cardiac pathophysiology, especially in association with different diseases related to a defective supply of oxygen and nutrients to the heart. 34 Hypoxia is one of the initial triggering factors causing pulmonary vasoconstriction and increased pulmonary vascular resistance in PEs. 35 Increases in pulmonary vascular resistance lead to pulmonary hypertension and caused an acute rise in right ventricular afterload. This, in turn, increases tension in the wall of the right ventricle and may lead to impaired systolic function, dilatation of right ventricle, elevated right ventricular end-diastolic pressure and volume, and may cause RVD in PE. 4,36,37 In the present study, the level of CA IX was significantly elevated in patients with PEs with RVD and had a fairly good sensitivity(89.3% at a cutoff level of 32.45 pg/dL) for the prediction of RVD in PEs. There was also a positive correlation between CA IX and systolic pulmonary arterial pressure measured by echocardiography in the present study. The hypoxia-related activation of hypoxia inducible factor 1 plays a role in the pathogenesis of pulmonary hypertension. 38,39 Expression of hypoxia inducible factor and its transcriptional target CA IX in idiopathic pulmonary arterial hypertension plexiform lesions and remodeled pulmonary arteries 11 might be a key point for the positive correlation between CA IX and systolic pulmonary arterial pressure measured by echocardiography, in the present study. The CA IX may serve as a predictor of right ventricular dysfunction from the point of view of its expression in both the pulmonary vascular system and the cardiomyocytes. 11,12,34 Nevertheless, further studies are needed to verify these findings, especially in patients with pulmonary hypertension.
The present study has some potential limitations. The results about CA IX and its association with RVD on echocardiography are preliminary results and need to be verified from the point of view of CA IX and its association with mortality in patients with PE. Therefore, prospective randomized double-blind studies are needed to study or investigate an association of CA IX with adverse outcomes in patients with PE. Second concern could be that in the study population, we had 2 patients having an emphysematous lung without supplemental oxygen treatment before. The CA IX expression has been shown in pulmonary arteries of the emphysematous lung in association with hypoxia. 12 Therefore, these 2 cases with emphysematous lung without supplemental oxygen treatment before have no affect on the external validity of the study results. Third limitation may be the exclusion of active malignant patients with PE from the study population due to potential confounding effect of the active malignancy on CA IX level. Therefore, the results of the present study could not be generalized for all the patients with PE with active malignancies.
In conclusion, the level of CA IX was significantly elevated in patients with PE having RVD, with a sensitivity of 89.3% at a cutoff level of 32.45 pg/dL for the prediction of RVD based on echocardiography. There is also a positive correlation between CA IX and systolic pulmonary arterial pressure measured by echocardiography. Further follow-up studies are needed to investigate the prognostic role of CA IX in patients with PE.
Footnotes
Acknowledgment
The authors thank Prof RW Guillery from University of Oxford for the English corrections made in the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by KTU Scientific Research Coordination Unit.