
Abstract
The aim of this study was to establish a method to predict the antiplatelet effects of aspirin in vivo based on in vitro results. Aspirin in 5 different concentrations was added to the platelet-rich plasma samples, and the rates of platelet aggregation induced by collagen were determined in vitro. In addition, platelet aggregation and plasma drug concentration values were determined in vivo before and after the administration of aspirin (162 mg). The 50% effective concentration (EC50) values obtained from the in vivo and in vitro experiments were shown to have relevance, because the EC50 ratio for each subject was the same (0.23 ± 0.03). The actual and predicted values for the rate of inhibition of platelet aggregation were well correlated (P < .0001, r = .95) when the predicted rate was determined using the present method. Our results suggest that the antiplatelet effects of aspirin can be predicted using blood samples obtained before its administration.
Introduction
Platelets play an important role in normal hemostasis and the pathogenesis of atherothrombotic diseases, such as acute coronary syndrome; thus, antiplatelet agents are widely used for the treatment of cardiovascular thrombosis. Aspirin is an effective antiplatelet agent, as its effects are exerted within several minutes after administration and persist for approximately 7 days, which is the life span of platelets. Aspirin elicits its antiplatelet effects via inhibition of platelet cyclooxygenase-1 (COX-1) by irreversible acetylation of a specific serine moiety, thereby blocking the formation of thromboxane A2. Furthermore, platelets do not resynthesize COX-1, because they do not have a nucleus, thus allowing the effect of aspirin to persist for the lifetime of the platelets. 1
However, some patients who have taken aspirin have been reported to experience recurrent events. 2 –4 Moreover, all patients do not derive the same benefits from aspirin, with up to 40% possibly resistant to its effects. 5 In addition, it is thought that its antiplatelet effects appear immediately after administration for the treatment of acute thrombotic disease, which influences prognosis. Therefore, it is important to predict the antiplatelet effects of aspirin before administration, though no methodology to evaluate these effects in individual patients has been established in a clinical setting and is urgently needed.
Currently, the detection of platelet activation is assessed by flow-cytometric determination of PAC-1 and CD62P platelets, 6 based on the response to arachidonic acid, collagen, or adenosine diphosphate. 7 Among the various parameters of platelet function, platelet aggregation has been most extensively evaluated in clinical situations. However, criteria have not been established, because studies of platelet responsiveness generally use 1 or 2 agonists at 1 or 2 concentrations for determination of the best range of concentrations. Herein, we examined platelet aggregation after aspirin administration with the aim of developing a method for the evaluation of its antiplatelet effects. Consequently, we established that platelet aggregation at a final concentration of 1.0 μg/mL was able to assess the response to collagen as a platelet aggregating agent by light transmission (LT). Various platelet function tests and point-of-care assays are available and increasingly utilized. However, assessment of platelet function to evaluate the efficacy of various treatments has not been decided. 8 Presently, the LT aggregometry represents the gold standard of laboratory-based methods to evaluate platelet function. 9 In the present study, we attempted to establish a methodology by which the antiplatelet effects of aspirin in vivo could be predicted from those determined in vitro.
Methods
Methodology for the Prediction of Antiplatelet Effects of Aspirin In Vivo From In Vitro Results
We enrolled 5 healthy volunteers (4 males, 1 female) after obtaining their consent. The study protocol and informed consent form were reviewed and approved by the ethics committee of the Tokai University of Hachioji Hospital. The subjects were judged to be in good health based on their medical history, physical examination, vital signs, and routine laboratory test findings. None had a history of aspirin-induced asthma, diabetes mellitus, or hyperlipidemia. The subjects were instructed not to take any medicine within 1 week before the study commencement and no food within 4 hours of the examination on the day of the study. Subject's physical finding and laboratory test data are shown in Table 1.
Subject Characteristics.
Abbreviations: ALT, alanine aminotransferase; AST, aspartate aminotransferase; BUN, blood urea nitrogen; DBP, diastolic blood pressure; Glu, glucose; HDL-C, high-density lipoprotein cholesterol; HR, heart rate; LDL-C, low-density lipoprotein cholesterol; SBP, systolic blood pressure; Scr, serum creatinine; TC, total cholesterol; TG, triglyceride.
In Vitro Experiment
The final concentrations of aspirin solution used in the in vitro experiment were 5.6, 16.7, 27.8, 55.5, 111.0, 166.5, and 555.5 μmol/L. The platelet aggregating agent used was collagen (Collagen Reagent Horm; Nycomed Pharma GmbH, Ismaning, Germany) at a final concentration of 1.0 μg/mL.
Blood samples were obtained from the subjects, and then the platelet counts in platelet-rich plasma (PRP) samples were determined and adjusted to 25 × 104 μL−1 using platelet-poor plasma (PPP). The time period for determination was standardized to within 2 hours from blood collection, and it was performed at room temperature. Aggregation response was measured using LT 7 with a PA-200 (Kowa Co, Ltd, Japan). Measurements were performed after adding 30 μL of collagen to 270 μL of PRP incubated for 1 minute in a thermostat bath at 37°C with agitation, which produced blank values. In the experiment with aspirin, PRP was incubated for 1 minute in a thermostat bath at 37°C with agitation, and then measurements were performed after adding 30 μL of collagen at 2 minutes after the addition of 2 μL of aspirin solution to PRP with agitation. The period of measurement was 7 minutes. The platelet aggregation reaction was evaluated based on the rate of antiplatelet aggregation, which was determined by subtracting the value of the rate of aggregation of each sample from the blank and was then divided by the value of the blank.
In Vivo Experiment
Measurement of Platelet Aggregation
The subjects were given 2 aspirin tablets (Bufferin 81 mg tablets, lot no. 61071; Bristol-Myers Squibb, New York, USA) with 200 mL of water. Blood sampling was performed until the maximum drug concentration time of the aspirin tablets, which was before and 10, 20, and 30 minutes after administration. Blood was collected from the alternate antecubital media vein from the right to the left a total of 4 times. Measurements of platelet aggregation before and after administration of aspirin were performed using the same method to produce blank values in the in vitro experiment. The platelet count of the PRP sample was determined and adjusted to 25 × 104 μL−1 with PPP before administration of aspirin. The platelet aggregation reaction was evaluated as the rate of antiplatelet aggregation, which was determined by subtracting the value for the rate of aggregation of the value of each sample from the blank and was then divided by the value of the blank.
Determination of Aspirin and Salicylic Acid in Human Plasma
Simultaneous measurements of aspirin and salicylic acid in human plasma were performed using a modified version of the method reported by Kees et al, 10 as follows. The plasma sample was shock frozen with dry ice and hexane, and then stored at −80°C until the assay. Frozen plasma samples were thawed in an ice water bath. Plasma of 500 μL was added to 500 μL of internal standard solution (5 μg/mL of 2-methylbenzoic acid in a 50:50 mixture of 0.2 mol/L hydrochloric acid and 0.2 mol/L orthophosphoric acid) and vortex mixed for 1 to 2 seconds. Acetonitrile of 1000 μL was added, and the solution was mixed again. After 15 minutes, at 4°C the mixture was centrifuged (1 minute, 10,500g) to separate the precipitated proteins. The supernatant was transferred to 10-mL tubes containing 270 mg sodium chloride, and then briefly vortex mixed and incubated at 4°C for 10 minutes. After vortex mixing and centrifuging again (1 minute, 10,500g), 400 μL of the upper organic layer was transferred into autosampler vials, and 100 μL was injected into the chromatograph. Separation was performed using a TSK-GEL ODS-80TS QA (250 × 4.6 mm2 ID, particle size 5 mm; Tosoh Co Ltd, Japan). The mobile phase was water, 85% phosphoric acid, and acetonitrile (740:0.9:416, v/v/v) delivered at a flow rate of 0.8 mL/min. Chromatographic separation was performed at 30°C and monitored at 235 nm. The limits of quantification of aspirin and salicylic acid were 0.1 ng/mL and 0.1 μg/mL, respectively.
Analysis
The relationships between drug concentrations and antiplatelet aggregation were analyzed using a sigmoid E
max model (equation 1), where E
max (%) was the maximum inhibition rate of platelet aggregation, EC50 (μmol/L) was the 50% effective concentration (EC50), C (μmol/L) was the drug concentration, E was the inhibition rate of platelet aggregation, and γ was the Hill coefficient.
We hypothesized that the γ values were equal for both in vitro and in vivo. Then, the EC50 values for in vitro and in vivo as well as γ were estimated by simultaneous substitution of the relationship between the rate of antiplatelet aggregation and the measured values of the drug concentrations obtained in vitro or in vivo using a nonlinear least-squares method, as shown in equation 1, with MLAB software (Civilized Software Inc., Maryland, USA). The PPP and PRP were used as controls for 100% and 0% LT, respectively. The maximum inhibition rate of platelet aggregation (E max) was set at 100%.
Aspirin binds to COX-1 in an irreversible manner in the mesenteric or portal vein after gastrointestinal absorption and before its appearance in the systemic circulation. Therefore, the concentration of aspirin in vivo was used as the sum concentration of aspirin and salicylic acid in plasma for indication of concentration in the mesenteric vein or portal vein before appearing in the systemic circulation.
Prediction of Antiplatelet Effects of Aspirin In Vivo Based on In vitro Findings
We examined the ratio of EC50 in vivo to EC50 in vitro (EC50 in vivo/EC50 in vitro). Accordingly, the individual antiplatelet effect of aspirin was predicted using the following equation, with the EC50 in vitro value.
Verification of the Prediction Method
Blood samples were collected for a total of 4 times within 30 minutes, which was a severe condition for the subjects. Hence, the prediction method was established with 5 subjects, and verification was done with 17 additional healthy volunteers. Blood sampling was performed before and 20 minutes after administration of aspirin, because that time point was considered sufficient to determine the relationship between the antiplatelet effect and the concentration of aspirin in plasma. Measurements of platelet aggregation and aspirin concentration in plasma were performed. The EC50 in vivo value predicted from the EC50 in vitro value and plasma concentration of aspirin was substituted in equation 2 to estimate the inhibition rate of platelet aggregation. The physical findings and laboratory test data of the subjects are shown in Table 1.
Results
Relationship Between Aspirin Concentration and Rate of Inhibition of Platelet Aggregation In Vitro
Figure 1 shows the relationship between aspirin concentration and inhibition of platelet aggregation in each subject, along with fitted curves obtained from equation 1. The fitted curves were well matched with the values obtained in the experiment. Table 2 shows the EC50 value in vitro for each subject.
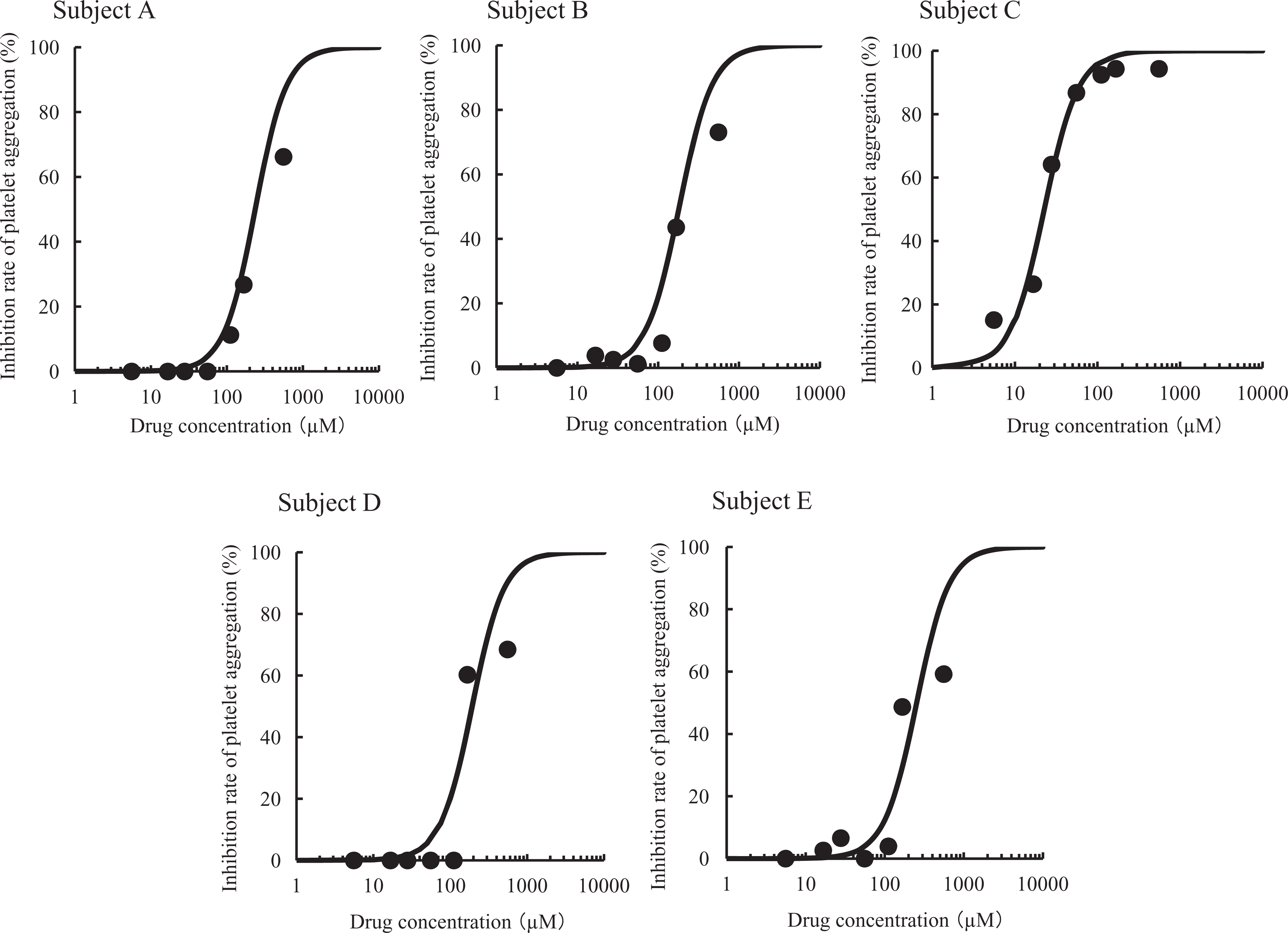
Relationships between drug concentrations (aspirin) and rate of inhibition of platelet aggregation in vitro. Symbol represents actual value; curve represents fitted curve.
Estimated Values of EC50, EC50 Ratio, and γ (n = 5).a
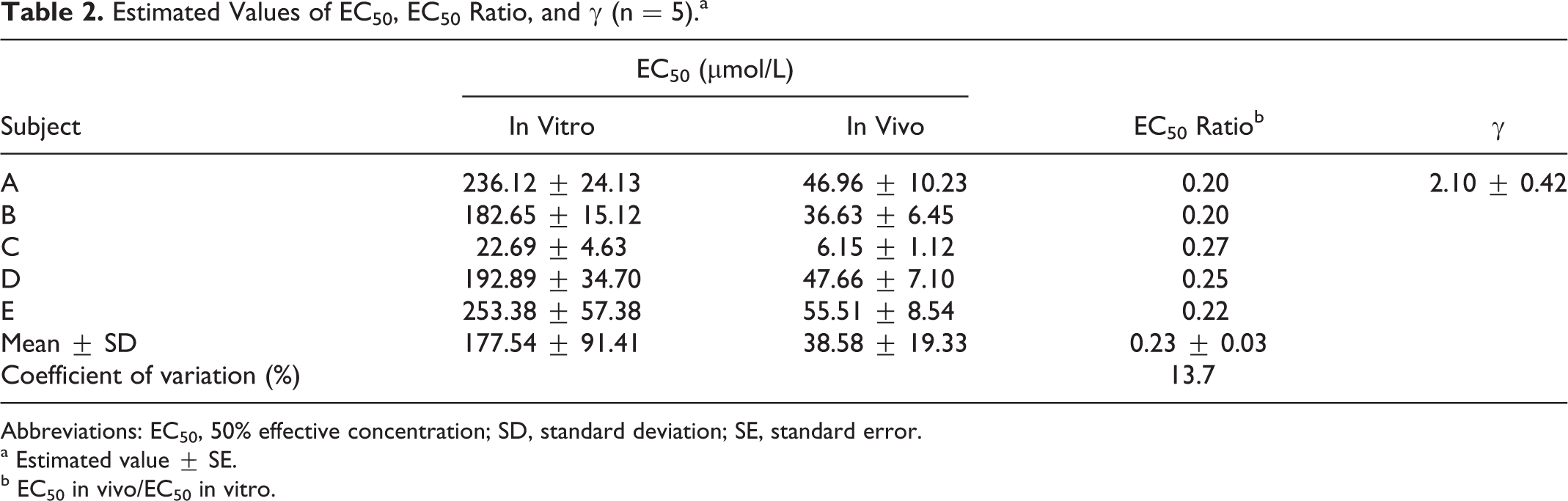
Abbreviations: EC50, 50% effective concentration; SD, standard deviation; SE, standard error.
a Estimated value ± SE.
b EC50 in vivo/EC50 in vitro.
Relationship Between Drug Concentration in Plasma and Rate of Inhibition of Platelet Aggregation After Aspirin Administration In Vivo
Figure 2 shows the relationship between drug concentration (aspirin + salicylic acid) in plasma and inhibition of platelet aggregation in each subject, along with fitted curves obtained from equation 1. The fitted curves were well matched with the values obtained in the experiment. Table 2 shows the EC50 values for each subject in vivo.
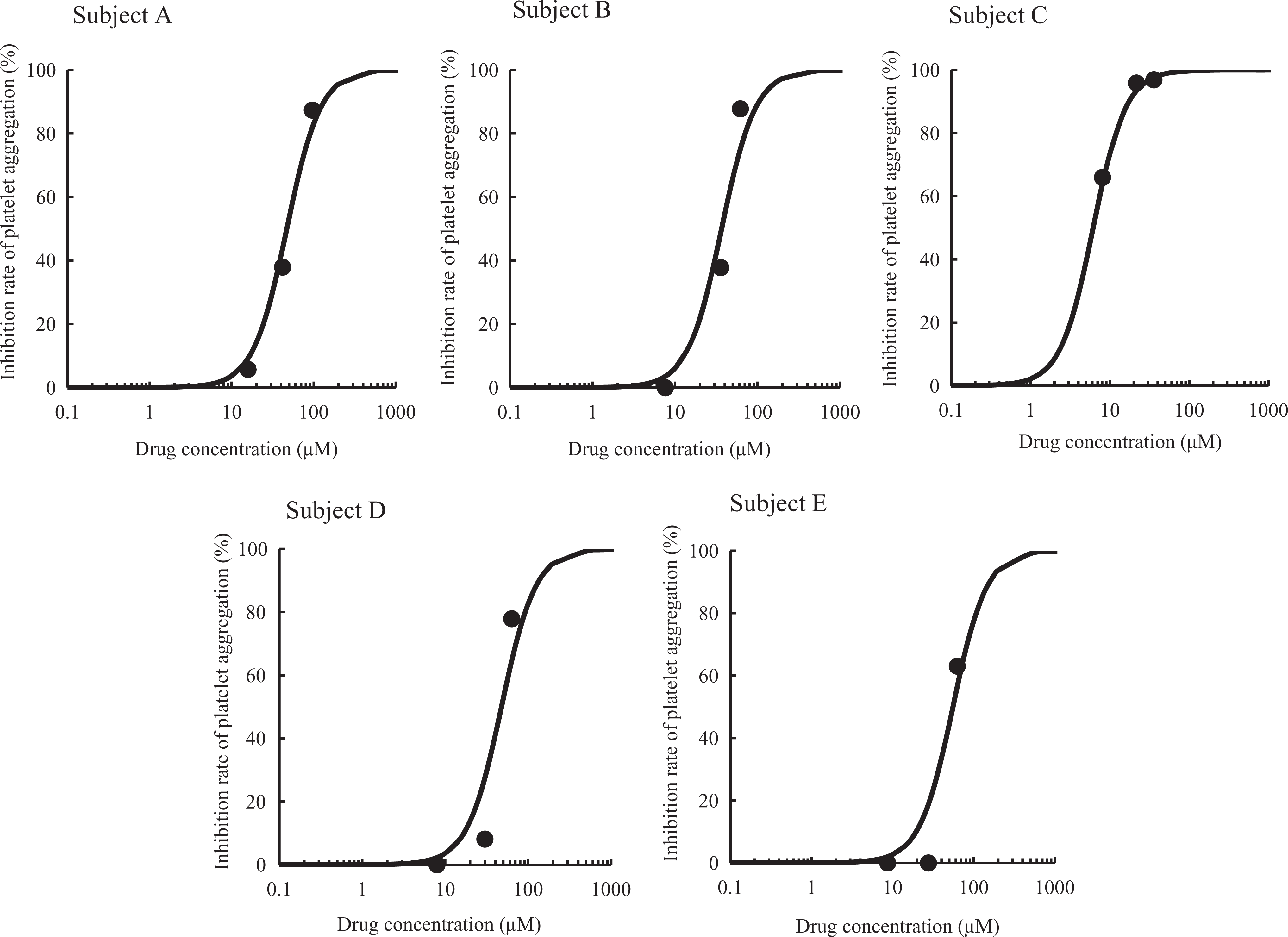
Relationships between drug concentrations (aspirin + salicylic acid) and rate of inhibition of platelet aggregation in vivo. Symbol represents actual value; curve represents fitted curve.
Relationship Between In Vitro and In Vivo Results in Regard to Drug Concentration and Inhibition of Platelet Aggregation
Table 2 shows the ratio of EC50 in vivo to EC50 in vitro (EC50 in vivo/EC50 in vitro), while Figure 3 presents fitted curves for each subject in vitro and in vivo. The value for the ratio of EC50 in vivo to EC50 in vitro was 0.23 ± 0.03 for each subject (coefficient of variation [CV, %], 13.7%). Therefore, we considered that the in vivo EC50 value was relevant to that in vitro.
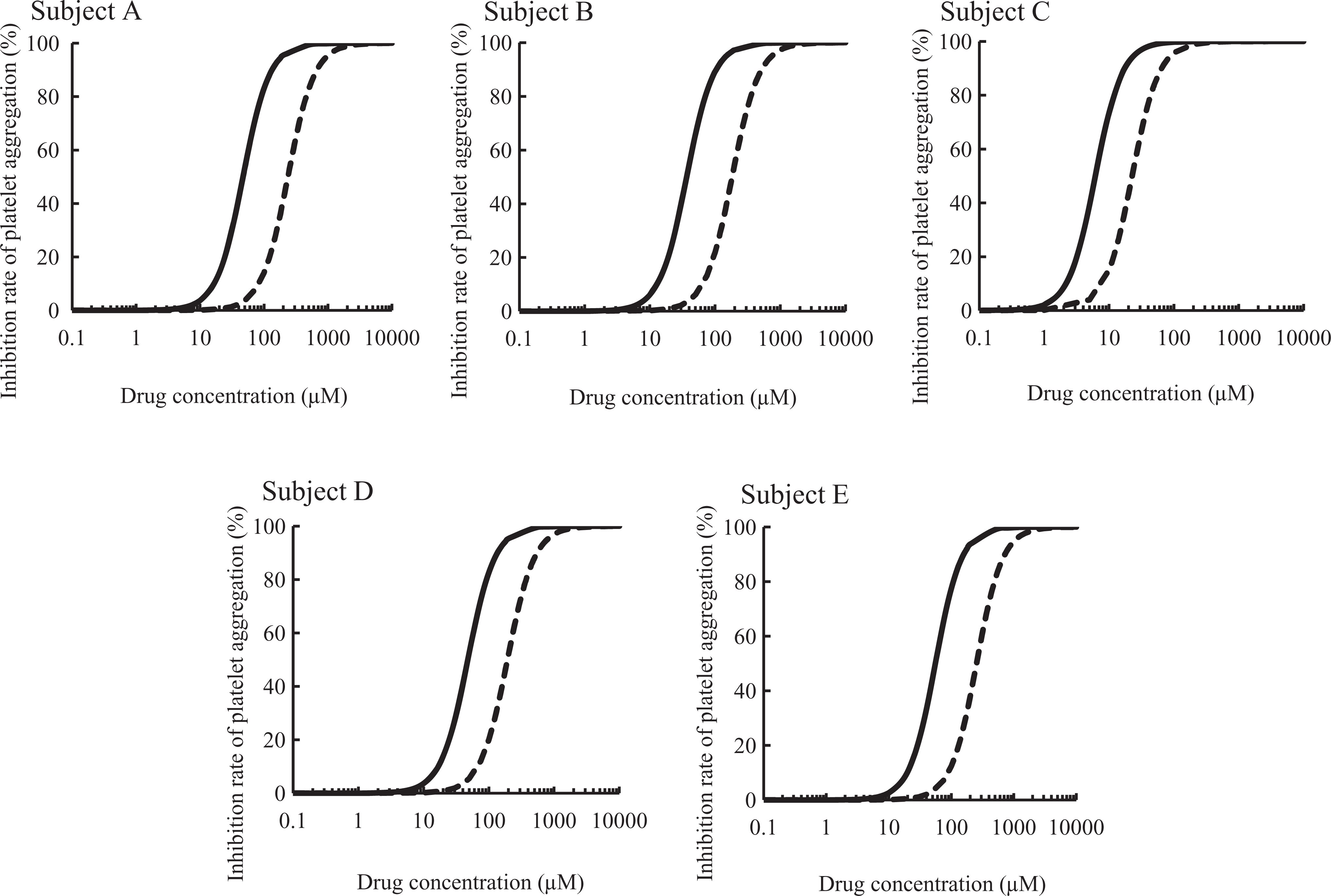
Relationships between drug concentrations and rate of inhibition of platelet aggregation. Dotted curve, in vitro; solid curve, in vivo; drug concentration, aspirin concentration (in vitro), aspirin + salicylic acid concentration (in vivo).
Prediction of EC50 In Vivo From EC50 Value In Vitro
The in vivo EC50 value was predicted by EC50 in vitro, and the mean ratio of EC50 in vivo/ to EC50 in vitro (0.23) was predicted using the following equation:
The predicted value of EC50 in vivo was obtained by substituting EC50 in vitro in equation 3. Figure 4 shows the relationship between the actual and the predicted values. This relationship had a regression equation of y = 1.05x and correlation coefficient of 0.997. Thus, the actual and predicted values of EC50 in vivo had a significant correlation of 1:1 (P < .01). Our results indicate that EC50 in vivo can be predicted from EC50 in vitro prior to aspirin administration.
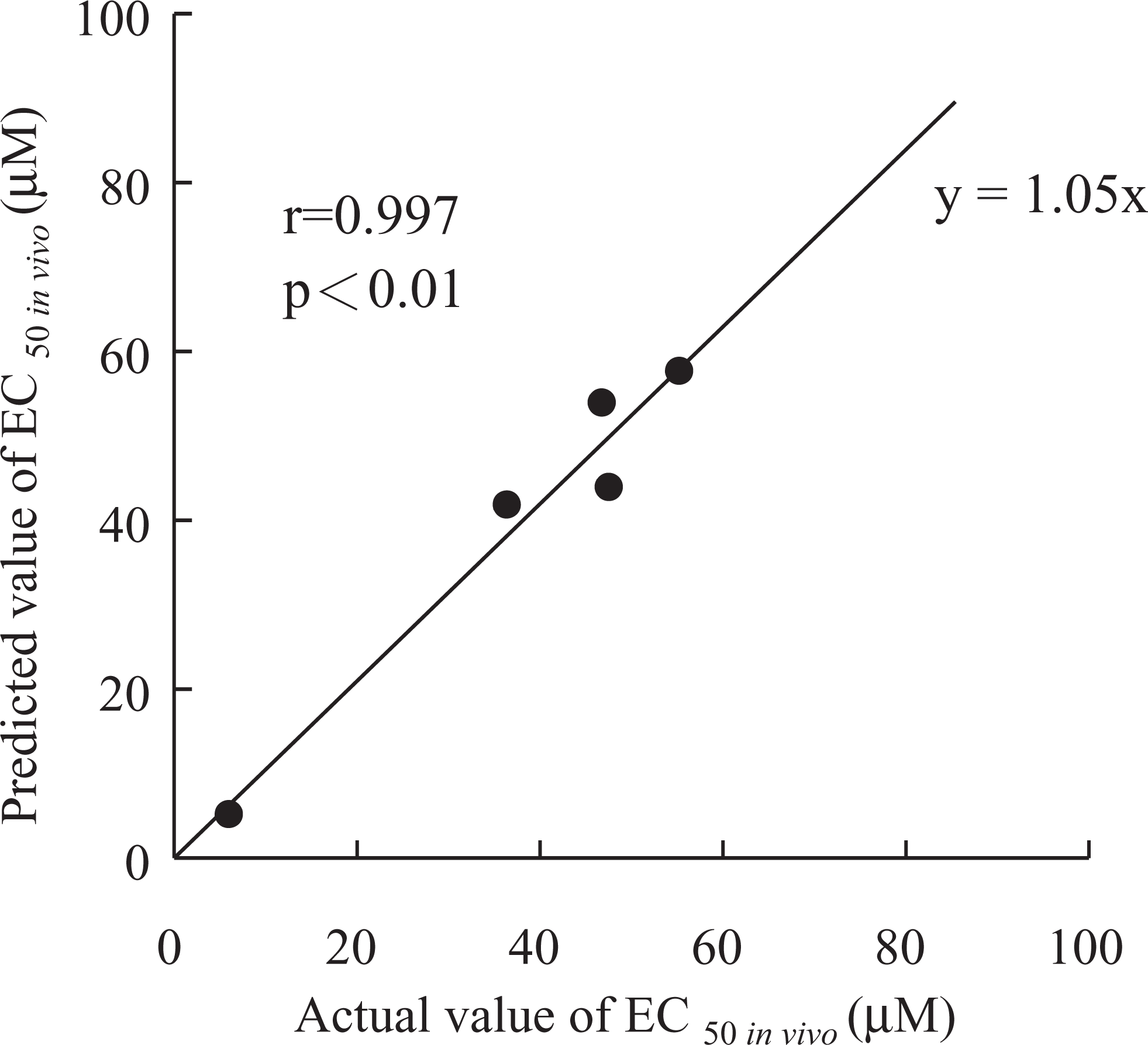
Relationships between actual and predicted values for EC50 in vivo. EC50 indicates 50% effective concentration (n = 5).
Prediction of Antiplatelet Effects of Aspirin In Vivo Based on In Vitro Findings and Verification of Prediction Method
The antiplatelet effects of aspirin in vivo were predicted using equations 2 and 3. Figure 5 shows the relationship between the actual and the predicted values, which had a regression equation of y = 0.98x and correlation of 0.95, which were significant (P < .0001). The median predicted EC50 in vivo value was 36.54 µmol/L (range: 3.92-58.28 µmol/L; n = 17). The median percentages for actual and predicted inhibition rate of platelet aggregation were 80.60% (range: 0.00-95.88%) and 81.82% (range: 14.23-99.83%), respectively. Consequently, these findings verified that the actual measured inhibition rate of platelet aggregation could be predicted from the EC50 in vitro value.
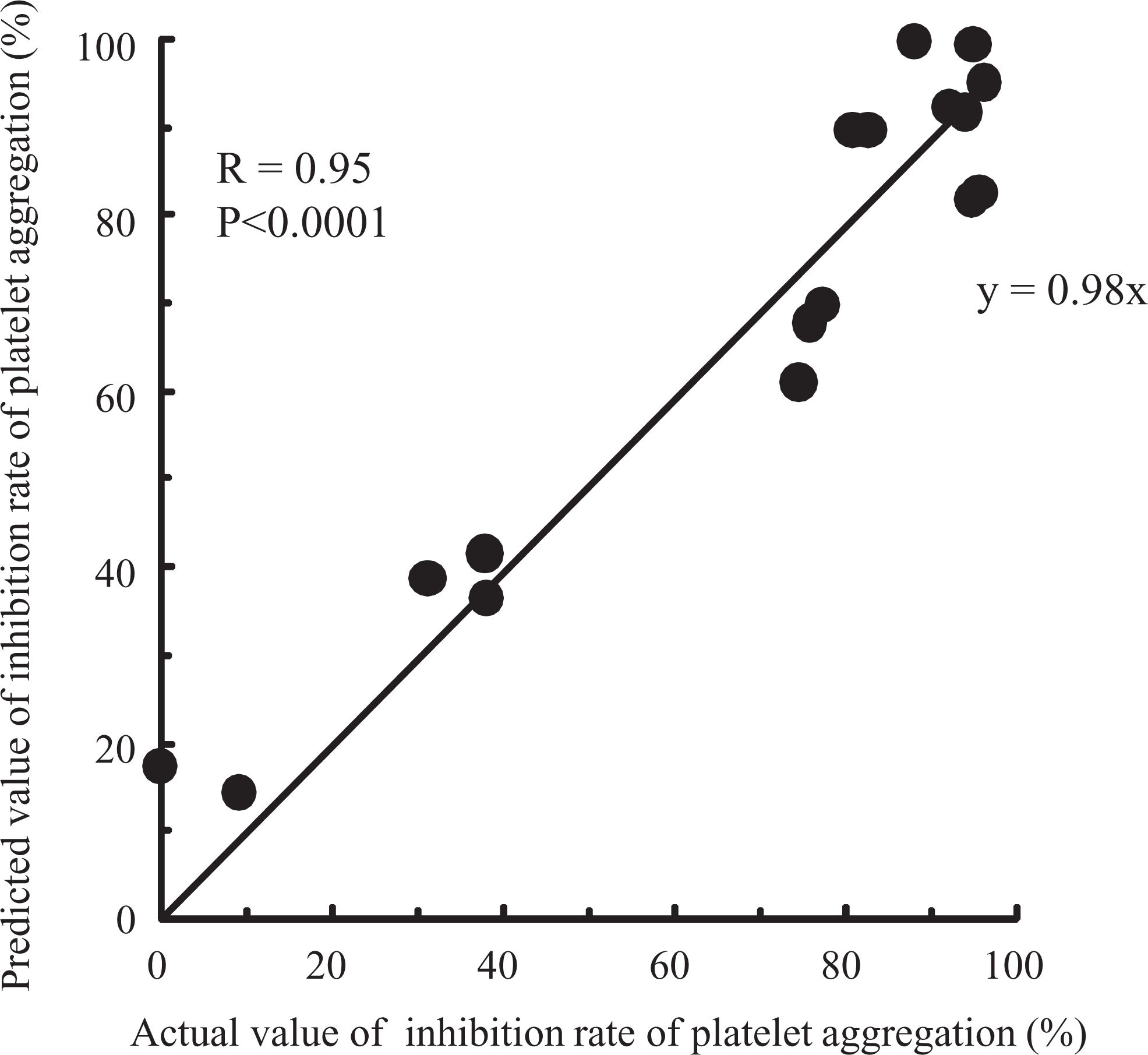
Relationship between actual and predicted values for the rate of inhibition of platelet aggregation (n = 17).
Discussion
Although low-dose aspirin is effective for the prevention against arterial vascular events, 11,12 we considered that changes in dosage or drug may be important, as some patients show aspirin resistance and others with acute coronary syndromes are affected by the antiplatelet effect immediately after administration. In the present study, we attempted to establish a methodology by which the antiplatelet effects of aspirin in vivo could be predicted from in vitro findings.
The half-life of aspirin is quite short at 24.0 ± 7.8 minutes. 13 On the other hand, aspirin binds to COX-1 in an irreversible manner, and the antiplatelet effect is continued for the lifetime of the platelets. Although there are few reports on the relationship between aspirin concentration and its antiplatelet effects, those appear early after administration. Thus, it has been proposed that the effects continue until the maximum drug concentration time (T max, 23.4 ± 8.4 minutes). 13
In the present study, the relationship between drug concentration and inhibition of platelet aggregation was analyzed using a sigmoid E max model within the first 30 minutes. We considered that the use of this model was reasonable, because the antiplatelet effects appeared early and 30 minutes prior to T max. In addition, no other direct actions were considered except for that toward platelets in the in vitro experiments, because the active site of antiplatelet aggregation by aspirin is platelets.
Since the manner in which aspirin reacted with platelets was the same in both the in vitro and the in vivo experiments, we hypothesized that the value for γ was the same in both the conditions. In order to determine the EC50 values in vitro and in vivo as well as that of γ, the relationships between drug concentration and rates of inhibition of platelet aggregation in vitro and in vivo were simultaneously fitted to a sigmoid E max model. The fitted curves corresponded well with the values of EC50 in vitro and in vivo. Hence, it was considered reasonable to fit them simultaneously to the values of in vitro and in vivo. In addition, the value of γ was estimated to be 2.10 ± 0.42 or approximately 2. The value of γ is a parameter that indicates the rising influence of drug concentration for a given effect and corresponds to the value in moles of the active binding site.
Aspirin has a single acetyl group that acetylates an active site serine-529 residue in COX-1. 1 Since COX-1 of platelets exists in a dimer formation, 14 aspirin binds 2 active sites for dimer COX-1. Hence, a value of 2 for γ was thought to be theoretically appropriate.
Aspirin is immediately metabolized to salicylic acid by esterase in the liver. It is thought that aspirin also acts immediately on platelets in the mesenteric or portal vein after gastrointestinal absorption, before metabolism. 15,16 Therefore, we assumed that the sum of aspirin and salicylic acid in plasma was appropriate for the estimation of drug concentration in the mesenteric or portal vein.
The value of γ was estimated to be approximately 12, when the relationship between aspirin concentration alone in plasma and inhibition rate of platelet aggregation was analyzed in vivo for confirmation. This value revealed that the action manner of aspirin with COX-1 was different between the in vitro and the in vivo conditions. Consequently, it supported our hypothesis that the active manner was the same in both in vitro and in vivo.
The aspirin and salicylic acid concentrations in plasma were increased until 30 minutes after oral administration of 162 mg in all subjects, indicating that the absorption of aspirin lasted for 30 minutes. Thus, it was considered reasonable to examine the relationship between the drug concentration in plasma and the rate of inhibition of platelet aggregation for that period of time. Accordingly, all of the values measured in this study were used for the analysis.
The in vitro EC50 values for the present subjects ranged from 22.7 to 253.4 μmol/L, while those for in vivo after aspirin administration were from 6.2 to 55.5 μmol/L, showing a lower shift for the in vivo values. As a reason for these results, it was thought that the drug concentration in plasma after systemic distribution was lower than that in the mesenteric or portal vein.
The ratio of EC50 in vivo to EC50 in vitro was 0.23 ± 0.03, while the CV was under 15%; thus, the EC50 values for both the conditions were relative in each subject. The slope of the line between the predicted values of EC50 in vivo and the actual values were approximately 1, with a significant correlation of 1:1. Our results indicate that EC50 in vivo can be predicted from the value of in vitro.
In addition, the actual and predicted inhibition rates of platelet aggregation were significantly correlated (y = 0.98x, P < .0001, n = 17). Hence, our findings suggest that the antiplatelet effects of aspirin can be predicted from the EC50 value obtained in vitro. Moreover, blood sampling at 20 minutes after aspirin administration was important to determine its plasma concentration and rate of inhibition of platelet aggregation. In the future, we intend to perform a prospective study on patients using the present method.
Conclusion
In conclusion, we established an effective method for the determination of the antiplatelet effects of aspirin in vivo based on in vitro findings (Figure 6). Our technique should be very useful for setting the initial dosage in aspirin therapy. In future, it will be important to study the initial dosage using the predicted value of EC50 in vivo in a prospective manner in patients receiving the therapy.
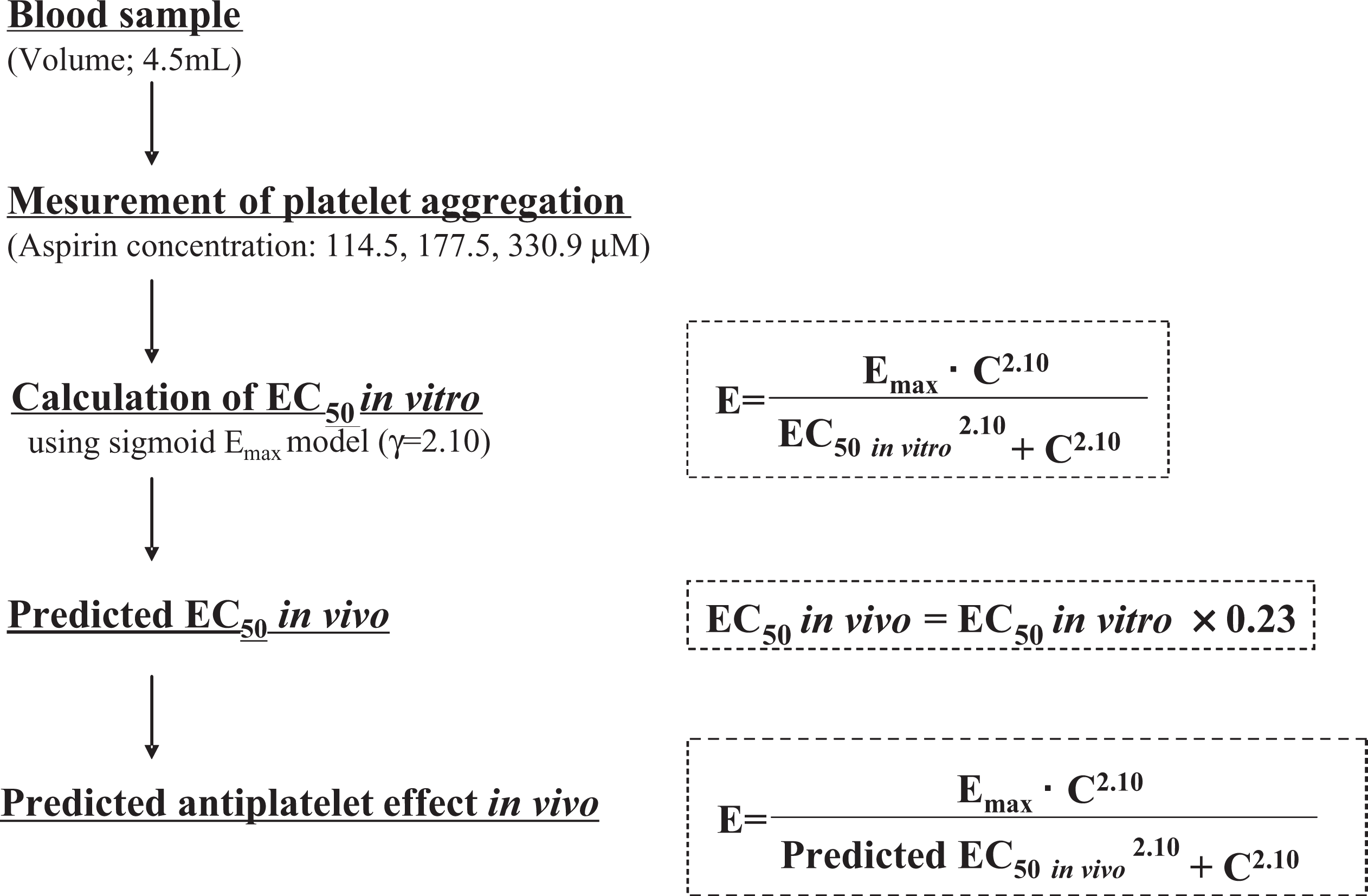
Flowchart for the prediction of antiplatelet effect of aspirin in vivo prior to administration.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.