
Abstract
Background:
Platelets play an important role in the pathogenesis of coronary artery disease (CAD). The importance of dual antiplatelet therapy to prevent recurrent ischemic events in patients who have acute coronary syndrome and who will undergo percutaneous coronary intervention (PCI) is well known and widely accepted as a gold standard. However, despite this apparently effective therapy, incidence of adverse ischemic events could not be decreased enough. Resistance to aspirin/clopidogrel is an important risk factor for adverse ischemic clinical events. Up-to-date studies revealed many risk factors for antiplatelet resistance, one of which is hypertension (HT). Currently, there is no sufficient number of studies evaluating the association between HT and antiplatelet resistance, which is the aim of this study.
Methods:
We enrolled 145 consecutive patients (19 female [13.1%], 126 male [86.9%], mean age 55 ± 10) with stable CAD receiving regular antiplatelet therapy composed of 100 mg/d aspirin and 75 mg/d clopidogrel. All patients had been implanted nondrug-eluting coronary stent and/or stents at least 1 month ago. The HT was diagnosed by 24-hour blood pressure (BP) monitoring. Clopidogrel and aspirin resistance was measured by impedance aggregometry method.
Results:
We included 49 patients with HT and 96 nonhypertensive patients with stable CAD. Aspirin resistance was detected in 22 (16.4%) of 134 patients who received aspirin. Clopidogrel resistance was detected in 55 (37.9%) of 145 patients who received clopidogrel. Prevalance of aspirin and clopidogrel resistance was significantly higher in the hypertensive group than in the nonhypertensive group (P = .030 and P = .007, respectively). Correlation analysis revealed weak but significantly positive correlation between clopidogrel resistance and serum uric acid levels, mean platelet volume, platelet count, and 24-hour mean systolic BP (r = −.180, P = .030; r = .189, P = .016; r = .226, P = .006; and r = .200, P = .016, respectively).
Conclusion:
We demonstrated higher incidence of antiplatelet resistance in patients with HT. Upon this finding, which is emerged from an actual group of patients with HT, cardioprotective effect of antiplatelet therapy in patients with HT should be argued.
Background
Platelets play a momentous role in the pathogenesis of coronary artery disease (CAD). 1 The activation and aggregation of platelets are involved in the process of intracoronary thrombus proliferation, following atherosclerotic plaque rupture and/or mechanical disruption in the coronary artery due to percutaneous coronary intervention (PCI). 1 Before all else, platelets adhere to collagen and von Willebrand factor on the ruptured plaque and create a platelet monolayer. Subsequently, they secrete secondary agonists such as thromboxane A2 and adenosine diphosphate (ADP) that stimulate other platelets with the help of thrombin, which is the last product of the coagulation cascade. 2
Antiplatelet therapy is a standard therapy in CAD. 1 Antithrombotic Trialists' Colleboration meta-analysis revealed a 25% decrease in recurrent serious vascular events in patients with high-risk CAD with antiplatelet therapies. 1 However, the same antiplatelet effect is not observed in all patients, and some patients experience recurrent thromboembolic events despite regular drug use. 1 These group of patients are defined as aspirin and/or clopidogrel resistant and are at increased risk of recurrent ischemic events. 1 Currently, several published studies revealed anemia, female sex, advanced age, diabetes, and high triglyceride levels as risk factors for antiplatelet resistance. However, there is no sufficient number of studies evaluating the association between hypertension (HT) and antiplatelet resistance. 1,3 –11 Therefore, we aimed to investigate the association of aspirin and clopidogrel resistance with HT diagnosed by ambulatory tension holter.
Methods
Patients
We enrolled 145 consecutive patients (19 [13.1%] female, 126 [86.9%] male, mean age 55 ± 10) in follow-up of our outpatient clinic with stable CAD. They received regular dual antiplatelet therapy, 100 mg/d aspirin and 75 mg/d clopidogrel. All patients had been implanted nondrug-eluting coronary stent and/or stents at least 1 month ago. Written informed consent was obtained from all the patients, and local ethical committee approved this study. The demographic and clinical features of all patients were recorded. Patients who had renovascular HT, primary hyperaldosteronism, pheochromocytoma, hyperthyroidism, Cushing syndrome, heart failure, renal failure, cardiac arrhythmia, unstable coronary disease, and implanted drug-eluting stent were excluded.
Blood Pressure Monitoring
Blood pressure (BP) was measured for 24 hours by the cuff-oscillometric method with the General Electric Tonoprt V monitor device (General Electric Milwaukee, USA). The recorder was programmed to record BP every 20 minutes during the day (07:00
Clopidogrel and Aspirin Resistance
Venous blood samples from all the patients receiving clopidogrel were collected to test tubes containing hyrudin. Clopidogrel antagonists were measured by impedance aggregometry method with multiple electrode aggregometry device (Dynabyte, GmbH, Germany). Impedance aggregometry method is based on the principle that platelets are nonthrombogenic in the resting phase; however, when activated they uncover receptors on their surfaces which help them adhere to vessel walls and artificial surfaces. Thrombocytes increase the resistance through the sensor when binded to sensor wires in the activator-added multiplate test bathtubes. Increased impedance due to platelets adhered to multiplate sensors is converted into aggregation unit (AU), and an AU versus time graphic is created. Clopidogrel resistance is evaluted by area under the curve (AUC). Aspirin resistance is also studied and evaluated by the same method. A value of 500 AUC minutes is considered as the minimal resistance value for patients under dual antiplatelet therapy and 470 AUC minutes for patients receiving aspirin or clopidogrel alone. 12
Statistics
Statistical analyses were performed using the SPSS software version 17. Descriptive analyses were presented as mean ± standard deviation (SD), and categorical variables were expressed as percentages. The variables were evaluated using visual (histograms, probability plots) and analytical methods (Kolmogorov-Simirnov/Shapiro-Wilk test) to determine whether they are normally distrubuted or not. Nonnormally distributed parameters were compared by Mann-Whitney U test. Categorical variables were assessed using chi-square or Fisher test. Spearman test was used for correlation and statistical analysis of nonnormally distributed parameters. P values below .05 were considered as statistically significant.
Results
We included 49 patients with HT and 96 nonhypertensive patients with stable CAD. Clinical and demographic features, medications, and laboratory findings were similar among patients with and without HT (Table 1). As expected, BP monitoring measurements were higher in the HT group than in the nonhypertensive group (P < .001; Table 2).
Demographic Features, Medication use Laboratory Findings, and Antiplatelet Drug Resistance in Patients With and Without Hypertension.
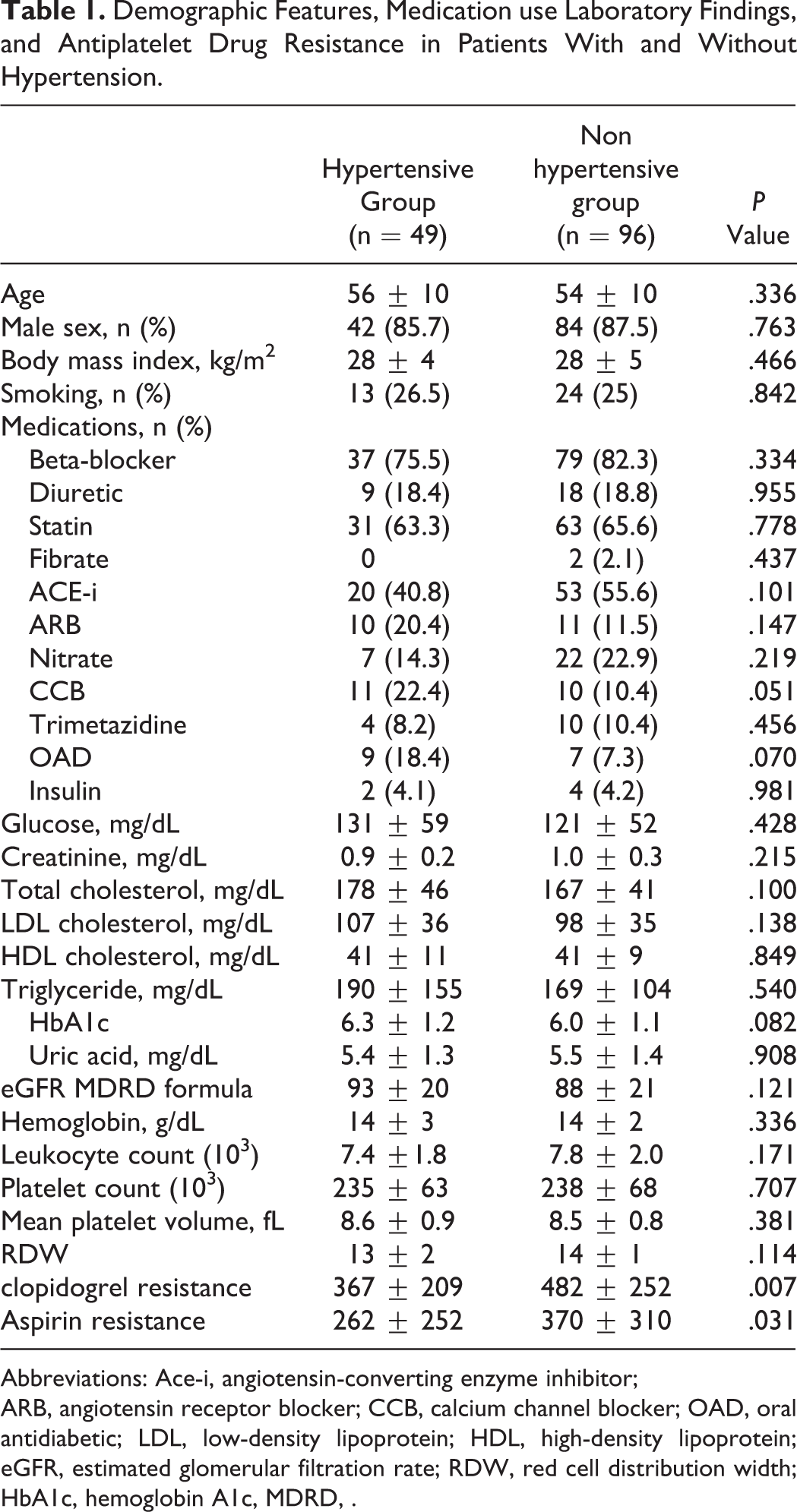
Abbreviations: Ace-i, angiotensin-converting enzyme inhibitor;
ARB, angiotensin receptor blocker; CCB, calcium channel blocker; OAD, oral antidiabetic; LDL, low-density lipoprotein; HDL, high-density lipoprotein; eGFR, estimated glomerular filtration rate; RDW, red cell distribution width; HbA1c, hemoglobin A1c, MDRD, .
Twenty-Four-Hour Blood Pressure Monitoring Measurements of the Patients.

Correlation Analysis Between Clopidogrel Resistance and Other Parameters.
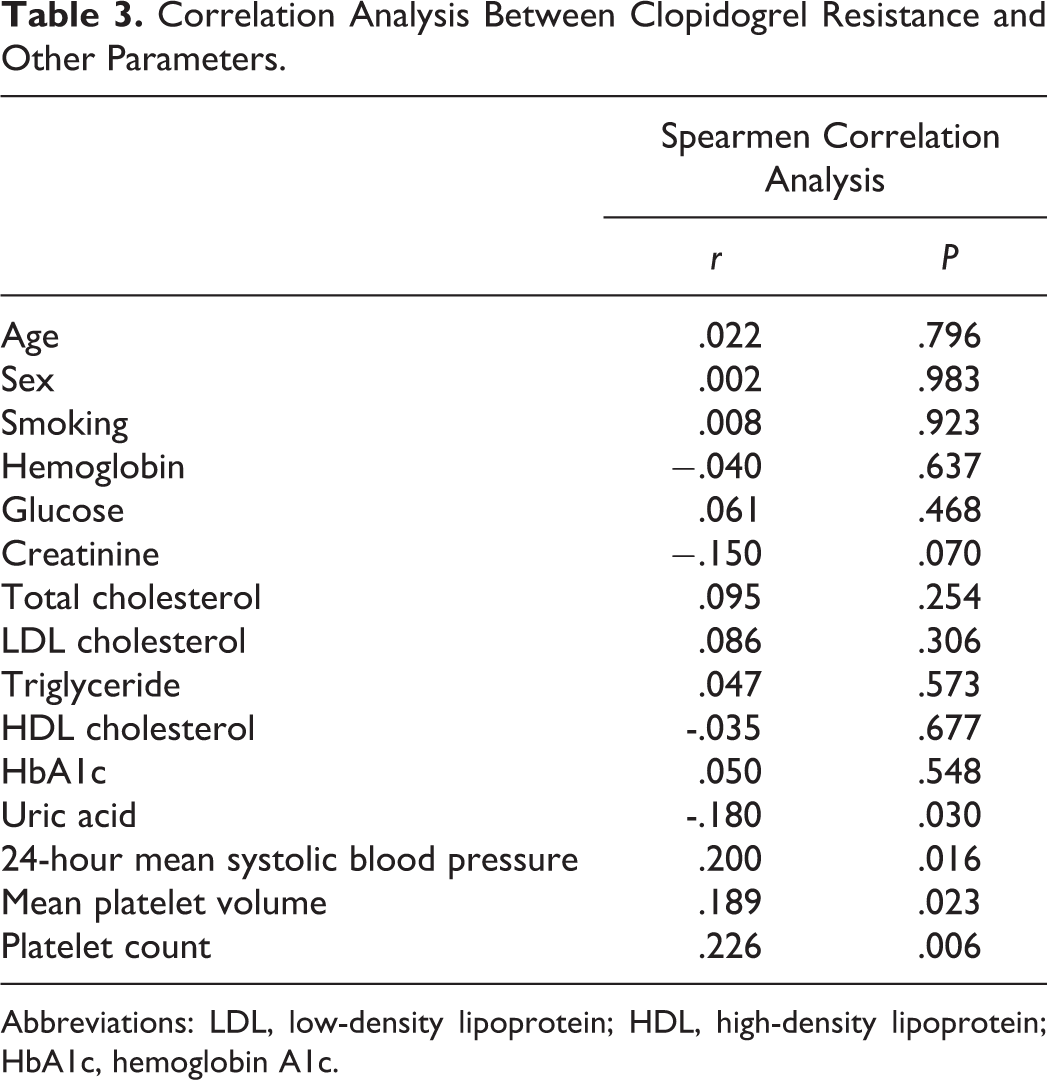
Abbreviations: LDL, low-density lipoprotein; HDL, high-density lipoprotein; HbA1c, hemoglobin A1c.
Although all of the 145 patients were treated with clopidogrel, 134 of them received aspirin. Aspirin resistance was detected in 22 (16.4%) of the 134 patients. On the other hand, clopidogrel resistance was detected in 55 (37.9%) of the 145 patients. Prevalence of aspirin and clopidogrel resistance was significantly higher in the hypertensive group than in the nonhypertensive group (P = .030 and P = .007, respectively).
Correlation analysis between clopidogrel resistance and clinical and laboratory parameters revealed weak but statistically significant positive correlation between clopidogrel resistance and serum uric acid level, mean platelet volume, platelet count, and 24-hour mean systolic BP (r = −.180, P = .030; r = .189, P = .016; r = .226, P = .006; and r = .200, P = .016, respectively, Table 3).
Discussion
The importance of dual antiplatelet therapy to prevent recurrent ischemic events in patients who have acute coronary syndrome and who will undergo PCI is well known and widely accepted as a gold standard therapy in current The American College of Cardiology /The American Heart Association and European Society of Cardiology guidelines. 13,14 Although clopidogrel and aspirin are both antiplatelet agents, they impede platelet aggregation by inhibiting different pathways. Therefore, combined therapy has additive beneficial effect. 13 However the incidence of adverse ischemic events, including the most catastrophic one—stent thrombosis, could not been lessened as desired. 13,14 Upon this, investigators researched on the reasons of this phenomenon and revealed that resistance to aspirin/clopidogrel is an important risk factor for the adverse ischemic clinical events. 15
Unfortunately, a single pathway is not responsible for the thrombotic events, so inhibition of one receptor may not prevent all of the thrombotic complications. 13 Antiplatelet resistance should be defined as the inability of the drug to act on its target receptor. Not only the clinical adverse event occurrence but also a laboratory test should confirm the ineffectiveness for the diagnosis. 13 However, none of the platelet function tests available today is valid enough, and there is no standardization. 1 Therefore, exact antiplatelet resistance definition is not possible up to date.
Aspirin irreversibly inhibits cyclooxygenase 1 (Cox-1) activity and reduces thromboxane A2 production. It is absorbed from the stomach, observed in plasma for 10 minutes, and steady-state plasma concentrations are achieved in 30 to 40 minutes. 1,16,17 Aspirin, metabolized by esterases in blood and liver, has a bioavailability of 50% and a half-life of 15 minutes. Salicylate, the main metabolite of aspirin, has a half-life of 3 to 6 hours. 17 The antithrombotic effect of aspirin is via the reduced production of thromboxane A2, a prothrombotic and vasoactive agent. 2
Although there are many aspirin resistance definitions, it is mainly described as the low sensitivity of Cox-1 to inactivation by aspirin. 17,18 The absolute aspirin resistance mechanism is not known yet. 2 Smoking, drug interactions, and inappropriate dosing are possible extrinsic factors. On the other hand, structural variabilities that prevent Cox-1 acetilization and thromboxane production from nonplatelet cells are intrinsic factors that are accused up to date. 2
Due to a meta-analysis of 145 randomized trials performed in patients with cerebrovascular and cardiovascular diseases, 10% to 20% of the patients receiving aspirin with a history of thrombotic event experienced recurrent thrombotic event. 3 The given incidence of aspirin resistance according to the published studies performed in different patient populations such as patients with cardiovascular and/or cerebrovascular diseases, diabetes, hyperlipidemics, and patients with metabolic syndrome is 5.5% to 60%. 3 –11 However, there are no sufficient number of studies evaluating the association between aspirin resistance and HT.
Wang et al studied aspirin resistance in patients with stable cardiovascular and cerebrovascular disease and determined HT and diabetics as relative risk factors for aspirin resistance. 19,20 Abci et al demonstrated an association between HT and aspirin resistance in patients with stable CAD and diabetes. 20 Ozben et al investigated the prevalence of aspirin resistance in patients with HT and found significantly higher aspirin resistance in patients with poorly controlled HT than patients with controlled HT (25.6% vs 17.8%, P = .030). They concluded that platelet reactivity related to increased arterial stiffness, shear stress, and endothelial dysfunction may be the reason for aspirin resistance in the hypertensive group. 4 We also revealed similar results in this study.
On contrary, Feher et al found higher HT prevalence among aspirin-sensitive patients with cardiovascular disease. 21 However, they did not mention whether HT was well controlled or not. In fact, those patients also received more β-blockers and angiotensin-converting enzyme (ACE) inhibitor medications, and the investigators declared that these medications may have such a positive effect. 21 Many studies have investigated the association among antihypertensives, mostly calcium channel blockers (CCB), β-blockers, ACE inhibitors, and platelet aggregation. 22 The antiaggregant effect of nifedipin, verapamil, and diltiazem is widely accepted. Desai et al and Altman et al showed the additive antiaggregant effect of nifedipin and diltiazem on activity of aspirin. 23,24 Meser et al 25 investigated the effect of different ACE inhibitors on platelet aggregation and revealed lower aspirin resistance with fosinopril and kaptopril. Kalinowski et al determined that losartan and valsartan inhibits platelet adhesion and aggregation both in vivo and in vitro. 26 Winter et al found that pindolol may be more antiaggregant than metoprolol and propranolol. 27 Finally, Punda et al revealed that propranolol inhibits platelet aggregation more than atenolol. 28 Although there is no statistically significant difference among the drugs taken by the patients of both the groups in the present study, patients receiving CCB were slightly higher in the hypertensive group than in the normotensive group (22.4% vs 10.4%, P = .051).
The ADP that plays role in platelet activation binds to platelets by its G-protein-related receptors, P2Y1 and P2Y12. Stimulation of P2Y12 causes thromboxane A2 production, secretion of thrombocyte α-granule ingredients, and expression of P-selectin on the platelet cell wall. 13,16 Clopidogrel is a selective and irreversible blocker of P2Y12 receptor that effectively inhibits platelet activity and aggregation. 13,16 Additionally, clopidogrel inhibits collagen- and thrombin-induced aggregation. 13 It is quickly absorbed from the intestine and converted to its active thiol metabolite by cytochrome-P450 isoenzymes, CYP3A4, CYP3A5, and 2C19. 13 Clopidogrel has been increasingly used, since its additive clinical benefit when combined with aspirin has been shown by large randomized studies. 13 Effect of clopidogrel is time and dose dependent. 2 The steady state of platelet antiaggregation activity is achieved within 4 to 7 days with 75 mg/d clopidogrel and within 4 to 24 hours with 300 to 600 mg/d loading doses. 2
Antiplatelet response to clopidogrel varies from patient to patient. 14 Clopidogrel resistance, though not absolutely defined yet, is best determined by the platelet activity before and after the treatment and measuring the degree of ADP-induced platelet aggregation in vitro. 13 The definite causes of clopidogrel resistance are not known. However, several possible mechanisms have been proposed. They include intrinsic factors such as differences in intestinal absorption and in the capability of converting clopidogrel into active metabolite, inappropriate dosing (eg, insufficient drug dose due to increased body surface area), and drug interactions. Some other extrinsic factors claimed are P2Y12 receptor variability, excessive number of receptors, the polymorphism of genes that codes cytochrome P450 enzymes, especially CYP2C19 allele polymorphism, increased secretion of ADP, and upregulation of platelet-activation pathways. 2,13,14
The prevalence of clopidogrel resistance in various populations with cardiovascular diseases is given as 4% to 44%, depending on the dosing, definition, laboratory method, and the timing of blood sample collection. 1,13,14 Resistance rates are higher in patients who received 300 mg loading dose than in patients who received 600 mg loading dose. 29,30 However, platelet inhibition is not significantly different between 600 mg and 900 mg loading doses. 31 Gurbel et al study demonstrated the time-dependent feature of clopidogrel resistance. They showed that the incidence of clopidogrel resistance had a tendency to decrease over time; 53% to 63%, 30%, and 13% to 21% of the patients had clopidogrel resistance at 2nd hour, 11th day, and 30th day of the therapy, respectively. 31 They mentioned the induction of the cytochrome system and increase in the bioavailability of the active metabolites as the likely cause of this result. 31 Also, patients with diabetes have higher clopidogrel resistance rates than nondiabetics. 32 Other factors that have been associated with clopidogrel resistace in the literature are stent length and stent localization. 31,32
We found higher prevalence of clopidogrel resistance in patients with HT than without HT (P = .007). Weak but statistically significant positive correlation has also been demonstrated between clopidogrel resistance and serum uric acid, mean platelet volume, platelet count, and 24-hour mean systolic BP (r = −.180, P = .030; r = .189, P = .016; r = .226, P = .006; and r = .200, P = .016, respectively). Similarly, Kim et al defined high systolic and diastolic pressures as risk factors for clopidogrel resistance in patients with stable cardiovascular and cerebrovscular diseases. 1 They suggested that high adhesivity and aggregability in patients with HT may be responsible for antiplatelet resistance.
In parallel with Ozben et al 4 and Kim et al, 1 we also believe that increased vascular shear stress due to HT reactivates platelets in a manner that impairs antiplatelet response. However, further investigation is needed to answer the question “What shall we do after once identified biochemical antiplatelet resistance?” Unfortunately there is no single response. In fact, the exact association between biochemical resistance and thrombotic events is also not clear. 13
Study Limitations
There are some limitations in this study. First of all, it was designed as single-center study and consisted of relatively small patient population size making the power of the study limited. We did not follow-up patients. Indeed, long-term follow-up would reveal recurrent ischemic events and more precious data about clinical outcomes of the patients. We only measured aspirin/clopidogrel resistance once; however, some investigators suggest measuring resistance more than once. 4 We defined the antiplatelet resistance biochemically but not clinically. We could not make genetic testing for clopidogrel resistance because of lack of foundation. Drug compliance was only orally questioned; we neither count the pills nor measure the serum levels of the drugs.
Conclusion
Although lots of studies can be found in the literature about aspirin and clopidogrel resistance performed in different patient groups, there are still many questions. There is no consensus on the definition, reasons, and risk factors. We demonstrated higher incidence of antiplatelet resistance in patients with HT. Upon this finding which is emerged from an actual group of patients with hypertension, cardioprotective effect of antiplatelet therapy in patients with HT should be argued. Patient-specific factors like HT should be defined and corrected in order to overcome this problem. Physicians should consider the individual risk profile of their patient when starting antiplatelet therapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article