
Abstract
The effects of graduated compression stockings (GCSs) on venous blood velocity were measured in 26 hospitalized medical patients while supine at rest. Peak blood velocity in the right femoral vein was 21.6 cm/s without GCS and 23.0 cm/s with GCS [not significant (NS)]. Peak blood velocity in the right popliteal vein was 12.5 cm/s without GCS and 15.0 cm/s with GCS (NS). Mean blood velocity in the right femoral vein did not increase significantly with GCS, but mean blood velocity in the right popliteal vein increased marginally from 5.0 cm/s to 5.8 cm/s (P = .05). Among 11 patients with venous insufficiency (refilling time ≤19 s), neither peak nor mean blood velocity in the femoral or popliteal veins increased significantly with GCS. In conclusion, thigh-length GCS in hospitalized patients had little or no effect on popliteal or femoral vein blood velocity while supine at rest, irrespective of whether the patients had venous insufficiency.
Thigh-length graduated compression stockings (GCSs) have been shown not to increase venous blood velocity in healthy young men while resting quietly in a supine position. 1 Healthy normal young participants, however, may differ from hospitalized patients, particularly because hospitalized patients are typically older and are likely to have a higher prevalence of venous insufficiency. Venous insufficiency of the deep veins occurs in 21% of the men and 12% of the women >50 years. 2 In the present investigation, therefore, we evaluated the effects of GCS on venous blood velocity in hospitalized patients while resting quietly in a supine position. We tested the hypothesis that GCS may not increase venous blood velocity while supine at rest, irrespective of venous insufficiency.
Methods
Right femoral vein and right popliteal vein time-averaged peak and mean blood velocity were measured using pulsed Doppler ultrasound in 26 hospitalized medical patients before and during the application of thigh-length-fitted venous GCS. Exclusions were those who were critically ill, unstable, unable to give informed consent, pregnant, prisoners, those with leg incisions or leg ulcers, and patients with acute deep venous thrombosis (DVT). This investigation was approved by the hospital’s institutional review board.
Measurement of Blood Velocity
Measurements of blood velocity were obtained while supine at rest with the head elevated 30° during quiet respiration with shoes and socks removed. Patients rested 5 minutes before measurements after applying the stocking. For measurement of popliteal vein blood velocity while wearing GCS, a hole in the size of the probe (4.5 × 1.5 cm2) was cut in the stocking over the region of the popliteal vein.
Pulsed wave Doppler recordings of blood velocity in the right popliteal and femoral veins were made using a Philips iU22 ultrasound system (Bothell, Washington) and L9-3 broadband linear array transducer with an extended operating frequency range of 9 to 3 MHz. The settings (gain, contrast, and rejection) were optimized after initial evaluations and then maintained constant. The threshold was maintained constant at 50%. A 2-mm sample volume was positioned at the center of the color signal to create a 45° and 60° angle of insonation between the direction of flow and the Doppler beam. Values of blood velocity were obtained from the computer measurements on the recording system.
Venous Reflux Photoplethysmography
Venous reflux was assessed by venous reflux photoplethysmography prior to measurements of blood velocity. Refilling times of >25 seconds without a tourniquet were interpreted as normal. 3,4 Some, however, interpreted a normal venous refilling time as ≥24 seconds, 5 ≥20 seconds, 6 and ≥19 seconds. 7 Refilling times of ≤19 seconds were considered indicative of venous insufficiency by some. 5,6 Stücker et al considered refilling times of 20 to 25 seconds as mild, 10 to 19 seconds as moderate, and <10 seconds as severe venous insufficiency. 3
Measurements of venous reflux were obtained in the right leg using a Parks Flo-Lab Model 2100 PPG (Aloha, Oregon). Measurements were made with the patient in the sitting position, with the legs freely dependent and not weight bearing. The photoplethysmography probe was firmly affixed 2 inches above the medial malleolus. The lower calf was squeezed for approximately 1 second and then fully released for 2 seconds. After 2-second interval, calf squeezing and relaxation were repeated for further 6 cycles.
Filling times were measured from the time when the calf squeezing and relaxation maneuver was stopped to the point where the refilling curve reaches a plateau. If the plateau point was not defined clearly, the refilling end point was assumed to be where the curve recovered to baseline.
If the refilling time was ≤20 seconds, a blood pressure cuff was placed just above the ankle, and the test was repeated with the cuff inflated to 60 mm Hg. If the refilling time remained <20 seconds, the photoplethysmography transducer was placed approximately 1 inch more proximally and more posteriorly, and the test was repeated in 9 of the 10 patients to confirm the short refilling time.
If the filling time normalized after application of a tourniquet, we interpreted the test to indicate valvular insufficiency of the superficial veins. If filling time did not normalize after application of a tourniquet, we interpreted the test to indicate valvular insufficiency of the deep veins.
The GCS
New thigh-length Thrombo Embolic Deterrent (TED) stockings (Kendall, Tyco Healthcare Group LP, Mansfield, Massachusetts) were used in each patient. Stockings of appropriate size as recommended by the manufacturer were selected based on thigh and calf circumference. According to the manufacturer, the pressure pattern in these stockings is 18 mm Hg at the ankle, 14 mm Hg at the calf, 8 mm Hg at the knee, 10 mm Hg at the mid-thigh, and 8 mm Hg at the upper thigh. This gradient is thought to be optimal for elastic stockings used by patients who spend substantial time in bed. 8
Statistical Analysis
A paired t test was used to assess differences of means within each category of patients with and without GCS using InStat version 3.0, GraphPad Software (San Diego, California). The 95% confidence intervals (CIs) were also calculated with InStat version 3.0, GraphPad Software. P < .05 was considered statistically significant.
Results
Twenty-six patients were included. Patients were aged 59
Refilling times were >25 seconds (normal) in 7 (26.9%) of the 26, 20 to 25 seconds (mild venous insufficiency) in 8 (30.8%) of the 26, 10 to 19 seconds (moderate venous insufficiency) in 8 (30.8%) of the 26, and <10 seconds (severe venous insufficiency) in 3 (11.5%) of the 26 patients. One of the patients with moderate venous insufficiency had insufficiency of the superficial veins. All others had venous insufficiency of the deep veins.
Peak blood velocity in the right femoral vein without GCS among all the 26 patients was 21.6 cm/s (95% CI = 5.4-37.9 cm/s), and it did not increase significantly with GCS, 23.0 cm/s (95% CI = 1.9-44.1 cm/s; NS; Table 1). Mean blood velocity in the right femoral vein also did not increase significantly with GCS (Table 1).
Blood Velocity in Right Femoral and Right Popliteal Vein Without and With Thigh-Length Graduated Compression Stockings.
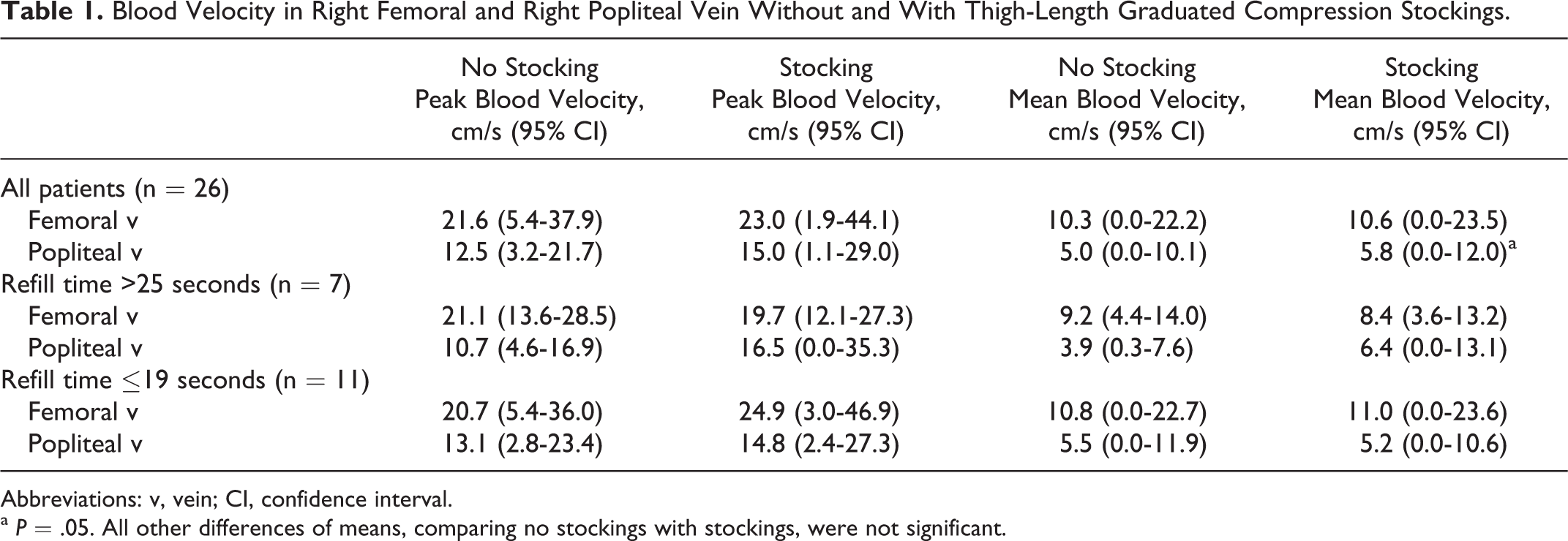
Abbreviations: v, vein; CI, confidence interval.
a P = .05. All other differences of means, comparing no stockings with stockings, were not significant.
Peak blood velocity in the right popliteal vein among all 26 patients was 12.5 cm/s (95% CI = 3.2-21.7 cm/s) without stockings, and it did not increase significantly with GCS, 15.0 cm/s (95% CI = 1.1-29.0 cm/s; NS; Table 1). Mean blood velocity in the right popliteal vein showed a clinically marginal increase from 5.0 to 5.8 cm/s (P = .05; Table 1).
Among 11 patients with moderate or severe venous insufficiency (refilling time ≤19 s), neither peak nor mean blood velocity in the femoral or popliteal veins increased significantly with GCS (Table 1). Among 7 patients with no venous insufficiency (refilling time >25 s), neither peak nor mean blood velocity in the femoral or popliteal veins increased significantly with GCS, although mean velocity in the popliteal vein increased nearly to a statistically significant value (Table 1).
Discussion
Fitted thigh-length GCS did not increase peak blood velocity in the femoral veins or popliteal veins of hospitalized medical patients while supine at rest, irrespective of whether they had venous insufficiency. Mean velocity in the popliteal vein among all patients, however, showed a clinically marginal increase. Although the number of included patients was small, and CIs were wide, it is clear that no large increments of blood velocity were shown. These observations are compatible with observations by others which suggest that GCS have no benefit in hospitalized patients. Our observations would not be applicable to patients confined to a chair.
We are not aware of the measurements of blood velocity in patients with venous insufficiency measured in the supine position. In the upright position, patients with venous insufficiency showed an increased peak velocity in the popliteal vein, but this was not shown in the common femoral vein. 9
We previously showed that peak blood velocity and mean blood velocity in the popliteal veins of healthy male volunteers did not change with GCS while supine at rest. 1 Although GCS resulted in no increased venous blood velocity while supine at rest, we previously showed that repetitive dorsiflexion of the foot more than doubled the time-averaged peak velocity in the popliteal vein. 10 The application of thigh-length GCS did not augment the increased blood velocity caused by ankle exercise. 1
Several previous investigations showed inconsistent findings regarding the effects of GCS in supine patients. Macklon and Greer in 10 women showed that popliteal vein time-averaged peak velocity while supine was 6 ± 1 cm/s (mean ± standard error of mean) without stockings and it was comparable, 9 ± 2 cm/second, with stockings. 11 They also found no change in blood time-averaged peak velocity in the femoral vein with GCS (16 ± 4 cm/s vs 15 ± 2 cm/s). 11 Keith et al showed that peak blood velocity in the proximal superficial femoral vein while supine in normal participants was not increased by GCS, 23.8 ± 1.6 cm/s (mean ± standard error of mean) versus 22.5 ± 3.7 cm/s. 12 Peak blood velocity in the proximal superficial femoral vein in postoperative patients also did not increase significantly with GCS, 21.8 ± 1.7 cm/s versus 26.4 ± 3.0 cm/s. 12 Norgren et al, in women in late pregnancy, showed no difference in maximal blood velocity in the common femoral vein while supine, comparing measurements without GCS (5 cm/s) and measurements with GCS (4 cm/s). 13
Some showed an increased blood velocity with GCS while supine. Jamieson et al showed that mean blood velocity in the common femoral vein increased from 10.0 to 13.9 cm/s with GCS in supine women during the postnatal period. 14 Büchtemann et al showed an increased mean blood velocity in the superficial femoral vein in the 30° reversed Trendelenburg position in women 4 to 5 weeks postpartum, but no change was shown during pregnancy. 15 Sigel et al showed that average femoral blood velocity increased 138% with thigh-length GCS. 8 Benkö et al, using venous occlusion strain gauge plethysmography in supine patients, showed a 77.8% mean improvement in venous outflow among 200 preoperative orthopedic patients with either thigh-length or knee-length elastic compression stockings. 16
The rate of clearance of contrast material during venography 17 and the rate of passage of radiopaque contrast material 18 suggested an increased blood velocity with venous compression. Measurement of transit time with radioactive Hippuran (iodohippurate sodium131I) also showed increased blood velocity with calf compression. 19
The definition of normal venous filling we used, refilling times >25 seconds without a tourniquet, 3,4 was strict and led to a high proportion of patients defined as having venous insufficiency. A venous refill time of >20 seconds has been suggested as normal venous filling. 20 If this definition was used, 12 (46.2%) of the 26 patients would have had venous insufficiency. The prevalence of venous insufficiency is age dependent. Our patients, on average, were aged 59 years. Among patients aged 55 to 64 years, 51% of the men and 27% of the women had chronic venous insufficiency based on clinical evaluation. 21 Over 80% had reticular varicose veins that are classified as mild venous insufficiency. 22
Whether there is a clinical benefit of GCS continues to be unresolved. Wilkins et al in 1952, among 5426 postoperative patients, reported fewer pulmonary embolism in those who were assigned elastic stockings. 23 Wells et al, in a meta-analysis of controlled studies of GCS, showed a 68% risk reduction in postoperative venous thromboembolism (VTE) in 11 studies of moderate risk surgical patients but showed no benefit in 1 study of patients who underwent orthopedic surgery. 24 Agu et al, in a meta-analysis of randomized controlled trials of GCS, showed a 64% reduction in relative risk of DVT in general surgical patients and 57% reduction in relative risk reduction following total hip replacement. 25 Some investigations, however, showed no beneficial effect of GCS. 26–28
Graduated compression stockings were recommended in the American College of Chest Physicians Evidence–Based Clinical Practice Guidelines, 9th Edition, 2012, alone or in combination with anticoagulants for the prevention of DVT in a variety of circumstances. 29 On the contrary, however, the American College of Physicians in their 2011 Clinical Practice Guideline recommended against the use of GCS for the prevention of VTE. 30
Strengths of this investigation are observations in patients with and without venous insufficiency. Weaknesses were wide 95% CIs of measurements and small number of patients with moderate or severe venous insufficiency. Mean values of popliteal vein blood velocity, however, were comparable to previous measurements in healthy participants, 1 and mean values of femoral vein velocity were comparable to measurements in the superficial femoral vein by others. 12
In conclusion, hospitalized patients showed no increased popliteal or femoral vein peak blood velocity with thigh-length GCS while supine at rest irrespective of whether venous insufficiency was present. Mean velocity in the popliteal vein among all patients, however, showed a clinically marginal increase.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.