Disseminated intravascular coagulopathy (DIC) is a serious disease with fatal consequences. We prospectively analyzed Innovance d-dimer immunoturbidimetric assay in 68 patients diagnosed with DIC on the background of malignancy (22), severe infection (20), or multitrauma (26) at a single institution between January 2010 and January 2011. Median age was 61 years (range 20-89). All patients were assessed according to the International Society of Thrombosis and Haemostasis (ISTH) DIC score. Applying a threshold of Innovance d-dimer of 10 mg/L fibrinogen equivalent unit (normal <0.5) was correlated with the highest sensitivity in malignancy (86%) and trauma/surgery (80%) compared to 54% in infection. The specificity remained high at 97% in infection, 81% in trauma and 77% in malignancy with a negative predictive value of 97% in trauma and malignancy, and 88% in infection. Our data suggest that Innovance d-dimer is a useful and simple tool that enhances the ISTH DIC diagnostic criteria. Further studies to confirm these findings are warranted.
Disseminated intravascular coagulation (DIC) is a serious complication of many clinical scenarios including infection/sepsis, malignancy, and also in the massive hemorrhage setting that is associated with trauma or surgery.1–3 Disseminated intravascular coagulation carries a considerable mortality rate, and once established, it is difficult to reverse.3–6 Disseminated intravascular coagulation remains a clinical diagnosis supported by laboratory data but with no universally accepted diagnostic algorithm.5 However, the Scientific and Standardization Committee on DIC at the International Society of Thrombosis and Haemostasis (ISTH) proposed a DIC scoring system based on 4 laboratory parameters and the presence of a predisposing condition.1 Increase in a fibrin-related marker, such as d-dimer, represents an element of the ISTH algorithm, which also scores elevations in prothrombin time (PT) and reductions in platelet count or fibrinogen concentration.1,7–9
Rationale
A sensitive immunoturbidimetric d-dimer assay would probably provide an excellent sensitivity and negative predictive value for the diagnosis of DIC. The Innovance d-dimer assay is a new class of automated d-dimer test based on immunoturbidimetric techniques with a promising performance in terms of high sensitivity and specificity. Little is known about the performance of Innovance in the context of patient evaluation for suspected DIC in different clinical settings as proposed in our trial. Therefore, we are evaluating both the analytical and clinical performance of the Innovance (Siemens, Marburg, Germany) immunoturbidimetric d-dimer assay in the different DIC clinical settings including infection, sepsis, trauma, surgery, and malignancy at a single institution.
Aims and Objectives
The main aim of this study is to evaluate the diagnostic performance of the new Innovance d-dimer immunoturbidimetric assay as a part of the diagnostic scoring system of the ISTH for DIC in different clinical scenarios associated with DIC.
Patients and Methods
We prospectively studied 68 patients who were diagnosed with DIC according to the ISTH criteria.1 These patients presented to the Launceston General Hospital (LGH), a major tertiary referral hospital for Northern Tasmania, during the period of January 2010 to January 2011.
The trial was approved by the Tasmanian Human Research Ethics Committee, Australia. The study was registered in the Australia and New Zealand Clinical Trial Registry (ANZCTR) under trail No: ACTRN12611001259932. Web address of the trial: http://www.ANZCTR.org.au/ACTRN12611001259932.aspx.
Eligibility Criteria
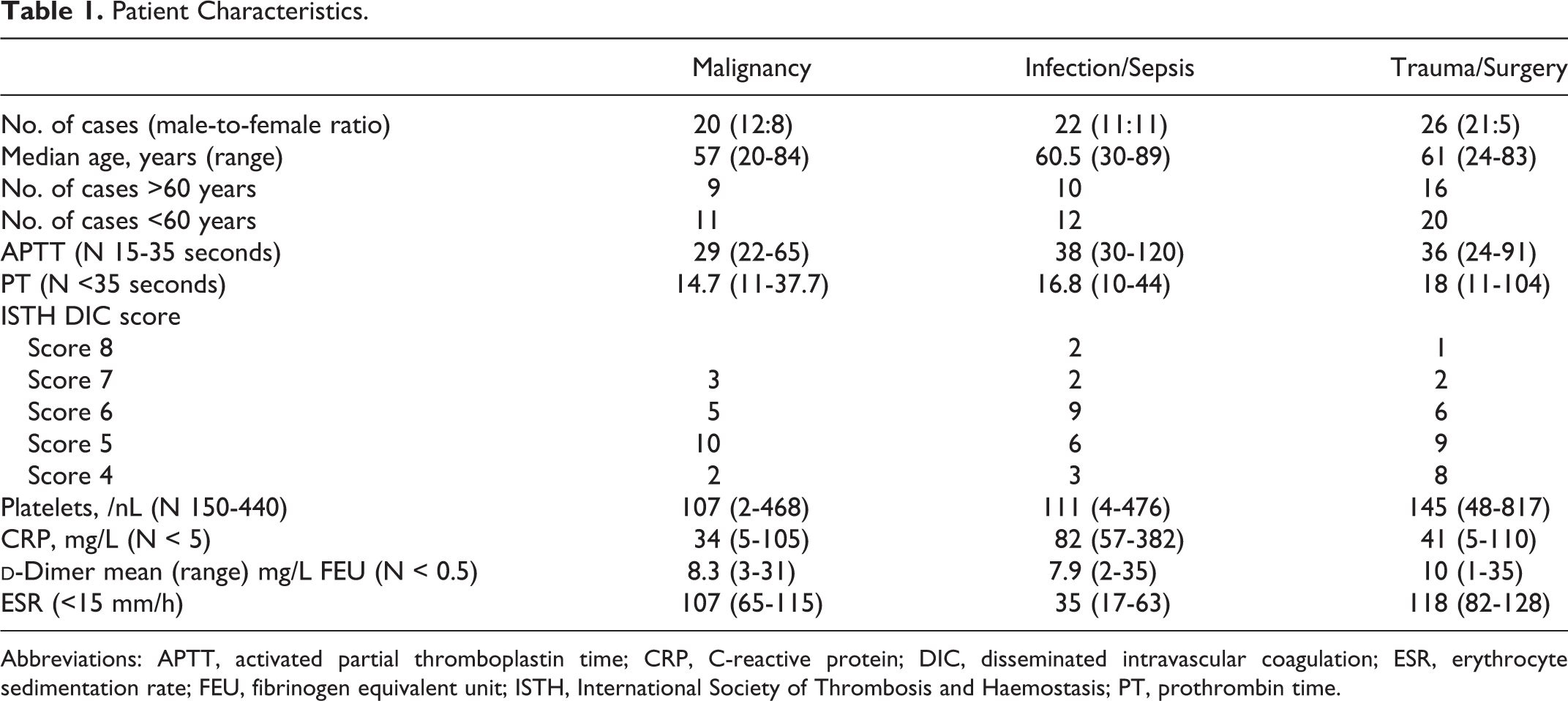
Patients with suspected DIC who presented to the LGH Oncology ward, intensive care unit (ICU), Surgery, and Emergency Departments were recruited for the trial (Tables 1 and 2). These patients had a clinical condition associated with DIC and were clinically suspected to have DIC together with an abnormal coagulation profile and other laboratory tests in line with the ISTH-scoring system of diagnosis of DIC. We used the DIC definition and diagnostic criteria of the ISTH as a reference in this study.1
Methods
The blood specimens were analyzed consecutively as per our protocol and included platelet count, PT, activated partial thromboplastin time (APTT), fibrinogen level, and Innovance d-dimer test (Siemens). All specimens were analyzed routinely within 2 hours of collection. Innovance d-dimer, PT, and APTT were tested using a Sysmex® CA1500 coagulation analyzer (Sysmex, Kobe, Japan). The conversion factor between “d-dimer Units” and “FEU” is 2, which is based on the fact that the molecular mass of both d-epitopes is equivalent to that of the E-epitope. Sixty-eight patients with clinical DIC were recruited in this study. The patients’ median age was 61 years and ranged from 20 to 89 years. The male-to-female ratio was 42:26. The male-to-female ratio was equal in the infection setting, 3:2 in malignancy, and 4:1 in trauma patients (Table 1).
Of the 68 patients analyzed, 22 had underlying malignancy, 26 patients had recent trauma or major surgery, and 20 patients had infection/sepsis associated with fever. Patients who had malignancy or trauma and developed sepsis were excluded from the study as they cannot be categorized under a specific group and may create bias in the analysis.
Patient Characteristics.
Malignancy
Infection/Sepsis
Trauma/Surgery
No. of cases (male-to-female ratio)
20 (12:8)
22 (11:11)
26 (21:5)
Median age, years (range)
57 (20-84)
60.5 (30-89)
61 (24-83)
No. of cases >60 years
9
10
16
No. of cases <60 years
11
12
20
APTT (N 15-35 seconds)
29 (22-65)
38 (30-120)
36 (24-91)
PT (N <35 seconds)
14.7 (11-37.7)
16.8 (10-44)
18 (11-104)
ISTH DIC score
Score 8
2
1
Score 7
3
2
2
Score 6
5
9
6
Score 5
10
6
9
Score 4
2
3
8
Platelets, /nL (N 150-440)
107 (2-468)
111 (4-476)
145 (48-817)
CRP, mg/L (N < 5)
34 (5-105)
82 (57-382)
41 (5-110)
d-Dimer mean (range) mg/L FEU (N < 0.5)
8.3 (3-31)
7.9 (2-35)
10 (1-35)
ESR (<15 mm/h)
107 (65-115)
35 (17-63)
118 (82-128)
Abbreviations: APTT, activated partial thromboplastin time; CRP, C-reactive protein; DIC, disseminated intravascular coagulation; ESR, erythrocyte sedimentation rate; FEU, fibrinogen equivalent unit; ISTH, International Society of Thrombosis and Haemostasis; PT, prothrombin time.
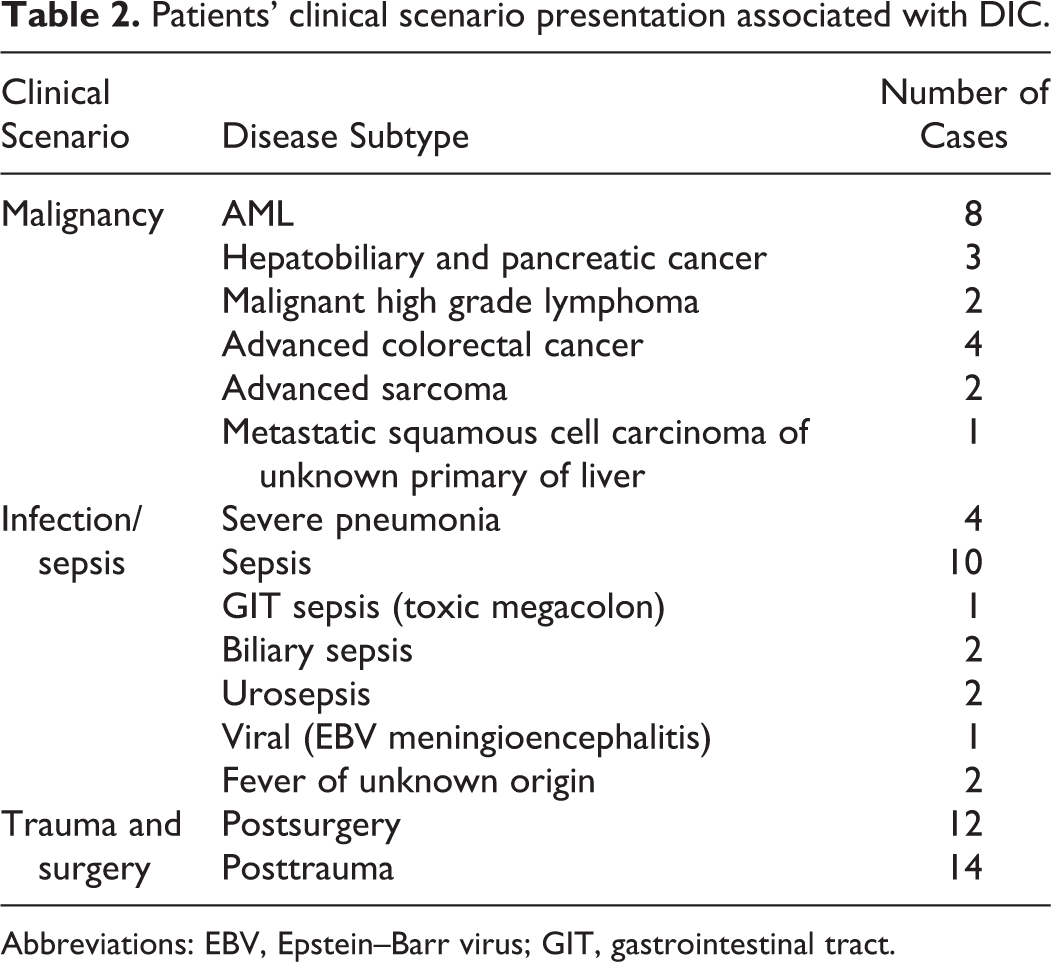
Patients' clinical scenario presentation associated with DIC.
Clinical Scenario
Disease Subtype
Number of Cases
Malignancy
AML
8
Hepatobiliary and pancreatic cancer
3
Malignant high grade lymphoma
2
Advanced colorectal cancer
4
Advanced sarcoma
2
Metastatic squamous cell carcinoma of unknown primary of liver
Another 48 age- and sex-matched inpatients from medical and surgical wards for whom coagulation testing was ordered as a part of their routine care and who had normal PT and APTT values without clinical history of DIC were also analyzed for the same parameters and served as an active control group.
Furthermore, 30 samples from normal healthy Red Cross volunteer donors were obtained for the reference range validation study of the d-dimer test in the normal population, where a cutoff value below 0.5 mg/L fibrinogen equivalent unit (FEU) was considered as normal.
Outcome Measures
Patients were classified as having or not having DIC according to the ISTH score.1 This included occurrence of low platelet count (platelet count >100/nL = 0; <100/nL = 1; <50/nL = 2), prolonged PT (PT <3 seconds = 0; >3 but <6 seconds = 1; >6 seconds = 2), low fibrinogen level (>1.0 g/L = 0; <1.0 g/L = 1), and raised d-dimer level (no increase = 0; moderate increase = 2; strong increase = 3).1 Accordingly, the ISTH score was calculated and interpreted as if the overall score was ≥5, it would be compatible with overt DIC. The score was repeated daily until improvement or patient discharge. If the score was <5, it would be suggestive (not affirmative) for nonovert DIC. Therefore, the score was repeated in the subsequent 1 to 2 days. If the score continues to be <5 it is most likely not diagnostic for DIC.
Statistical Analysis
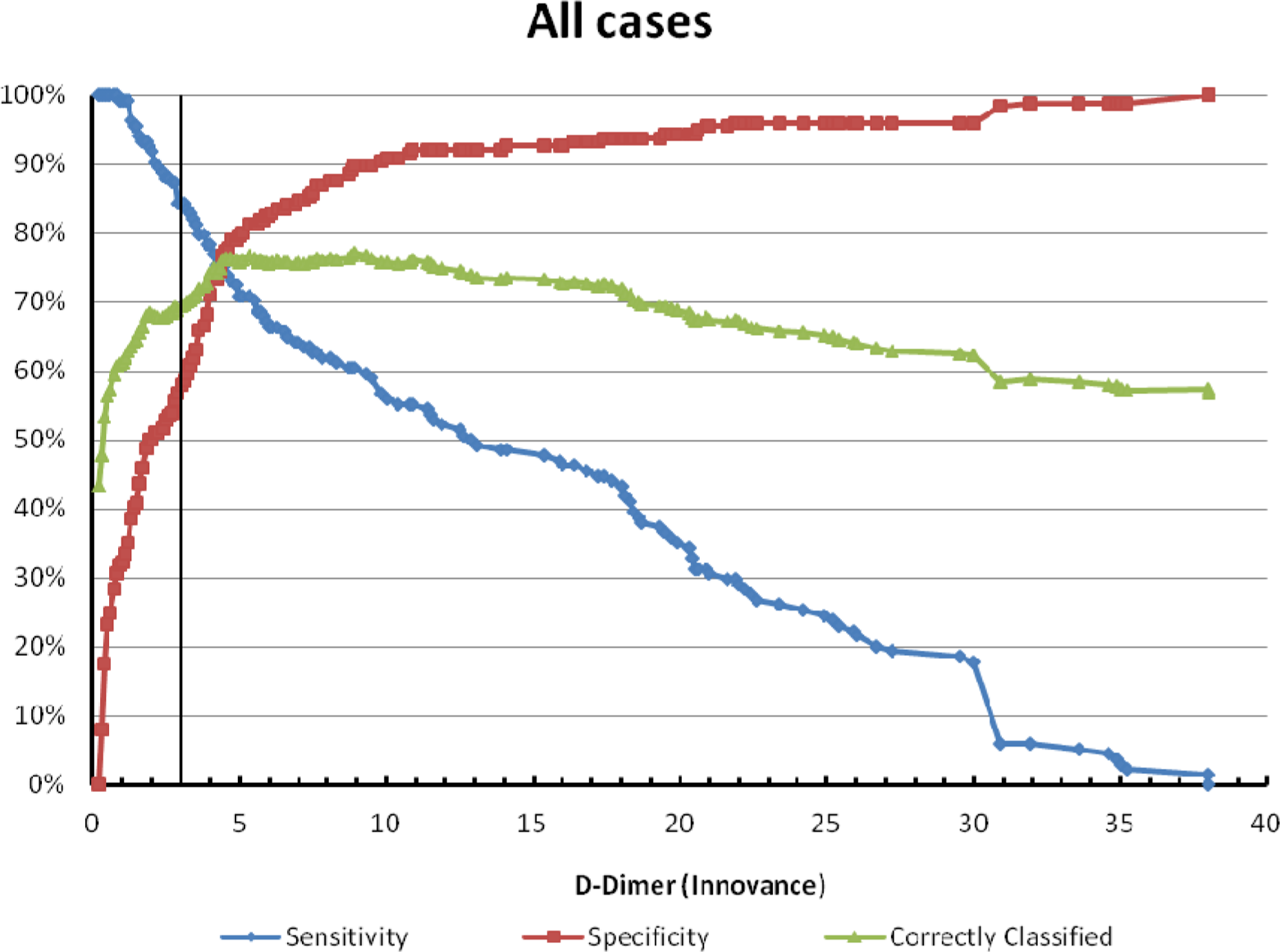
Receiver–operating characteristic curves were constructed from the maximum d-dimer measurement for each patient and the occurrence of DIC in that patient. Three possible diagnostic whole-number threshold levels were identified, and the sensitivity, specificity, positive, and negative predictive values for those thresholds calculated. These thresholds were then analyzed to estimate the likelihood of occurrence of DIC using binomial regression: relative risk ([RR]; 95% confidence intervals; P values) for each diagnostic group (malignancy, trauma/major surgery, and infection). All analyses were performed using Stata SE11 for Windows (StataCorp, College Station, Texas).
Results
Since this is a cross-sectional study, the follow-up occurred during hospital admission only.
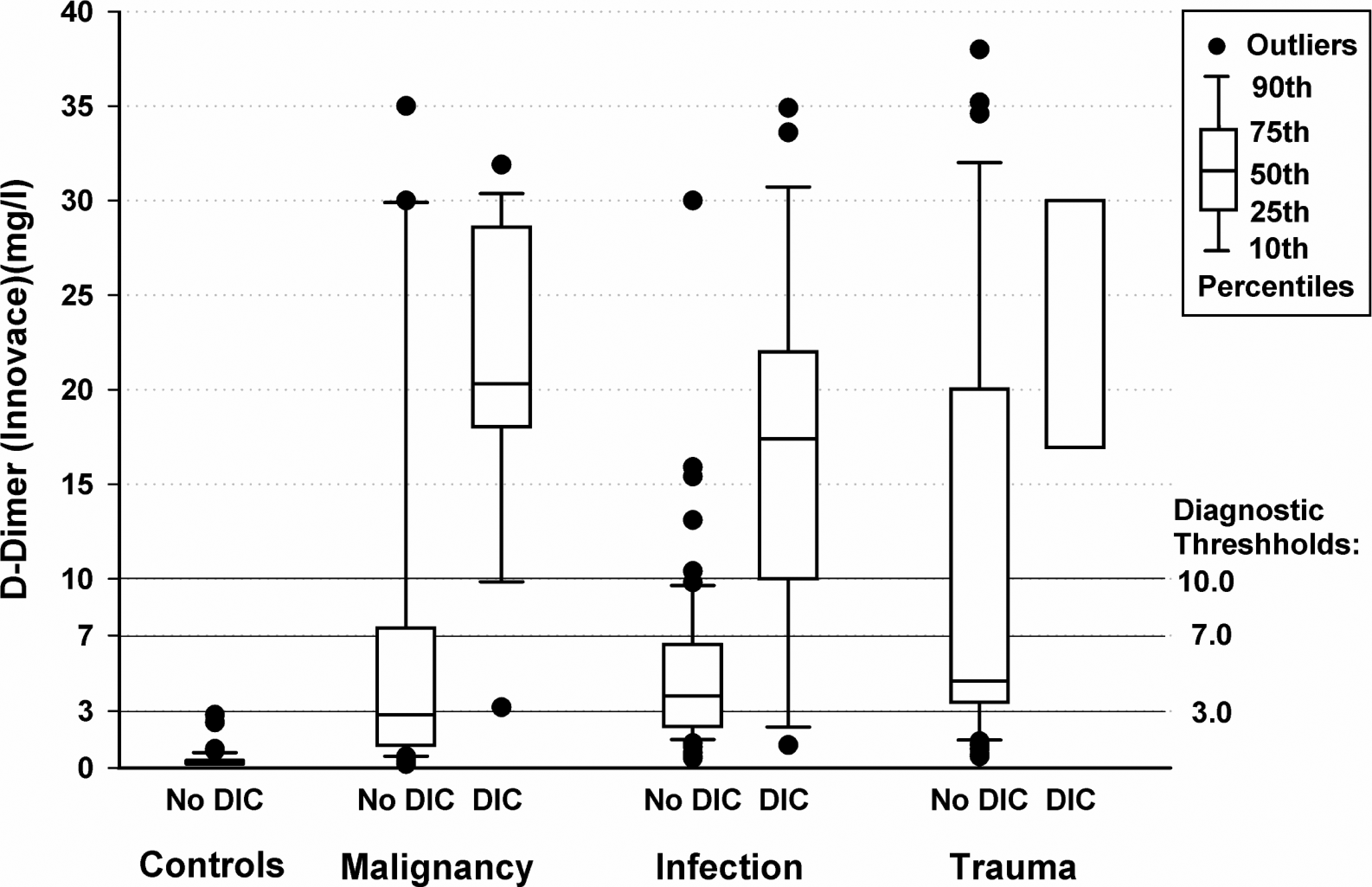
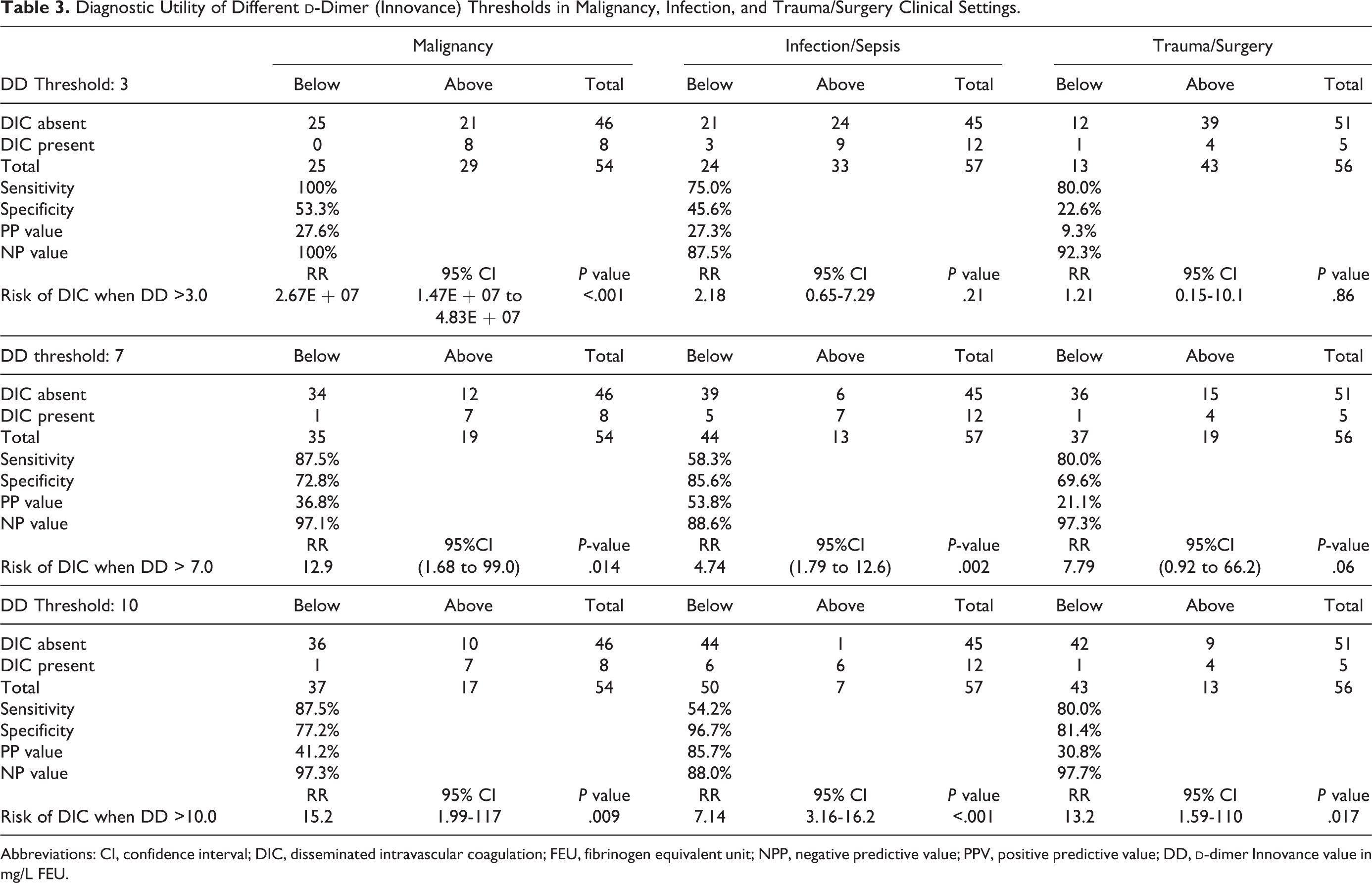
A d-dimer threshold prior to diagnosis of 3 mg/L FEU (normal <0.5) showed high sensitivity in malignancy (100%), infection (75%), and surgery/trauma (88%), with a high negative predictive value (Figure 1). However, the specificity was low, with a low positive predictive value. A threshold of 7 mg/L FEU reduced the sensitivity in malignancy (88%) and infection (58%) while remaining high in trauma (80%), but the negative predictive value remained high. In the meantime, the specificity was improved to 73% in malignancy, 86% in infection, and 70% in trauma. Increasing the threshold of d-dimer to 10 mg/L FEU showed highest sensitivity in malignancy (86%) compared to 80% in trauma and 54% in infection while again retaining a high negative predictive value (Figure 2). The specificity remains high in infection (97%) and trauma (81%) and also in malignancy (77%).
Most of the patients in the infection (90%) and malignancy (87%) groups scored 5 and above according to the ISTH score for DIC, while 70% scored 5 and above in the trauma group versus 30% with score of 4. The CRP level was elevated across all groups; however, with significant and greater increase in the infection group with mild elevation in trauma and malignancy that most likely reflected an acute phase reactant rather than concomitant infection evident by absence of clinical signs of infection such as fever. The platelet count was significantly lower in the malignancy (144 vs 216; difference 72; 95% CI −143 to −1; P = .048) and infection (143 vs 216; difference 71; 95% CI −141 to −1; P = .048) groups compared to trauma/surgery (Table 3). The erythrocyte sedimentation rate was significantly higher in the surgery and malignancy groups in comparison to infection (P = .03). Both PT and APTT were significantly higher in trauma and infection groups compared to malignancy (P = .001). The negative predictive value with the different d-dimer levels at 3, 7, and 10 mg/L FEU cutoff values remains high for malignancy, infection/sepsis, and trauma/surgery settings and was above 87% (Figure 1). Analysis of influence of sex or age on the d-dimer level showed no statistical significances.
Different Innovance d-dimer thresholds (mg/L fibrinogen equivalent unit [FEU]) in association with disseminated intravascular coagulation (DIC) in different clinical settings.
All Innovance d-dimer levels (mg/L fibrinogen equivalent unit [FEU]) analyzed with receiver–operating characteristic (ROC) analyses for sensitivity and specificity of detecting disseminated intravascular coagulation (DIC) according to the International Society of Thrombosis and Haemostasis (ISTH) criteria.
Diagnostic Utility of Different d-Dimer (Innovance) Thresholds in Malignancy, Infection, and Trauma/Surgery Clinical Settings.
Laboratory evidence of coagulopathy should be sought before DIC becomes evident so that an appropriate and effective management plan can be taken to address the underlying cause.8,9 Fibrin-related markers including d-dimer, fibrin degradation product, and fibrin monomer are useful tools for prediction and follow-up of the severity of DIC.10d-Dimer has the advantage of being a product of secondary fibrinolysis of fibrin and hence may be considered sensitive in the diagnosis of DIC. Fibrin monomer is usually produced early on from fibrinogen due to the action of thrombin in a hypercoagulable state and considered as a DIC marker together with the d-dimer in the clinical DIC score.1,10 Nevertheless there are limited data that evaluate the diagnostic performance of different types of fibrin monomers. In this regard, there is no definitive cutoff value of fibrin monomer in the diagnosis of DIC. Therefore, it is important to establish an easy, reproducible laboratory diagnostic and prognostic tool with d-dimer for DIC with therapeutic relevance and implication for clinical progress in line with the ISTH guidelines. In an ICU study, d-dimer was used for moderate and strong increases to diagnose DIC.9 Lack of sensitivity and specificity remain an issue with high d-dimer levels with an ongoing need to standardize methods and techniques to measure accurately fibrin end product with adequate sensitivity and specificity. In this sense, a precise cutoff remains to be defined.11,12 We noticed in our cohort study that a d-dimer cutoff value of 10 mg/L FEU is associated with a significantly higher positive predictive value in the infection group compared to malignancy and trauma groups (P < .001). This reflects that a very high d-dimer level is correlating significantly with infection with a higher specificity in contrast to mild-moderate d-dimer increase, which may represent nonspecific results in this cohort of patients.
It is worth noting that there are no data available regarding Innovance immunoturbidimetric assay in correlation with the diagnosis of different DIC clinical settings. We have demonstrated high sensitivity in malignancy and trauma settings with least in infection, and corresponding high negative predictive values for all groups with the Innovance d-dimer assay in association with DIC. An explanation for the improved sensitivity with the Innovance d-dimer assay compared to other assays is that it utilizes a monoclonal antibody (8D3) specific for epitopes contained on the cross-linked d-domains of fibrin derivatives. The antibody is covalently linked to polystyrene particles with the added advantage of the reagent also containing a blocking agent to heterophilic antibodies. A value <0.50 mg/L FEU is proposed as a threshold for the exclusion of DIC. Our trial had prospectively analyzed hospitalized patients who were not suspected of having DIC, serving as a control group compared to patients with suspected clinical DIC from the Oncology ward, ICU, surgical theater/ward or emergency department. This allowed testing of different d-dimer cutoff values in correlation with the scoring of DIC within the ISTH algorithm that may require to be assay specific.1
Our analysis identified a prospective cutoff that maximizes sensitivity and specificity of the Innovance d-dimer assay at different levels of 7 and 10 mg/L FEU. This may have a clinical implication for applying different treatment strategies in each situation in order to reduce morbidity and mortality associated with DIC.12–15 The negative predictive value was high in all groups (>87%), indicating the correlation of d-dimer assay and DIC as demonstrated in previous studies.10,11 Nevertheless, it remains a challenge to optimize d-dimer assays to have a clinical significance for individual patients.
It is worth noting that comparison of values determined with different d-dimer assays are limited due to the following facts: (a) “d-dimer” in samples is not only d-dimer but fibrin degradation products exhibiting “d-dimer” reactivity, such as large, medium size, small degradation products, and as the smallest product d-dimer. (b) Every patient sample has its own specific mixture of fibrin degradation products. (c) The assays are using different monoclonal antibodies, recognizing specific d-dimer epitopes, and, when recognizing similar epitopes, then it would be with different sensitivity. Most of the limitations of Innovance d-dimer are due to the previously described facts. Others may be caused by the technology used, for example, particle enhanced immunoturbidimetry.
Although method comparisons between assays are demonstrating systematical differences due to different standardization (leading to a slope different to 1.0) and different reactivity of single patient samples due to different mixtures of fibrin degradation products of the individual sample combined with the specific sensitivity of the monoclonal antibody used, the Innovance d-Dimer, has an acceptable correlation with Vidas d-dimer exclusion assay and to Stratus CS d-dimer assay as well as STA Liatest d-dimer assay.16 This could be achieved by aligning the standardization of these assays. Comparison of 23 quantitative d-dimer assays as basis for the development of d-dimer calibrators was performed by Dempfle and colleagues.17 However, due to the lack of comparability of d-dimer results obtained with different assays, clinical efficiency of every single assay has to be proven in corresponding studies. Assuming a good correlation between different d-dimer assays, such reference values might have been “transferred” from studies with other assays by multiplying the values with a certain conversion factor.
Our study has a few shortcomings. First, it has a relatively small number of patients; however, they form unique different groups with appropriate clinical scenarios that would justify the clinical implication of setting a cutoff value of d-dimer against the standard ISTH DIC-score. Second, it is difficult to conduct a randomized trial owing to the inherent difficulties of recruiting the targeted acute critically ill patients. Therefore, we used a dedicated control group of age- and sex-matched hospitalized patients as a point of reference.
In summary, our data suggest that the Innovance d-dimer assay is a useful and simple screening tool in the DIC diagnostic criteria with variable sensitivity and specificity and high predictive negative value according to the cause of DIC. Increasing the cutoff of the test was associated with higher specificity and reasonable sensitivity in diagnosing DIC. Accordingly, our study suggests that the d-dimer at a particular threshold is helpful in the diagnostic strategy of DIC. Furthermore, d-dimer assay is an easy test to perform with diagnostic performance showing an excellent correlation with the ISTH diagnostic algorithm for DIC. Our study suggests that the use of Innovance d-dimer may enhance the prognostic power of the ISTH-DIC score in different clinical scenarios that are associated with DIC. However, the d-dimer diagnostic threshold should be understood as a technique and test dependent and specific. Further studies to confirm our findings are warranted.
Footnotes
Authors’ Note
This manuscript is submitted for oral presentation at the Annual Scientific Meeting of the Australia and New Zealand Society of Thrombosis and Haemostasis, 2012 meeting, Melbourne, Australia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: the Clifford Craig Medical Research Trust, Launceston, Tasmania, Australia. Clifford Craig Medical Research Trust is a local community organization in Tasmania, Australia that supports medical research by providing monetary funds without interference in the research design or outcome. Clifford Craig Medical Trust Fund has no influence in the study design; subject, methods, data collection, analysis, interpretation of data; writing the research report; or the decision to submit the manuscript for publication. The grant was used to support the statistical analysis.
References
1.
TohCHHootsWK, SSC on Disseminated Intravascular Coagulation of the ISTH. The scoring system of the Scientific and Standardisation Committee on Disseminated Intravascular Coagulation of the International Society on Thrombosis and Haemostasis: a 5-year overview. J Thromb Haemost. 2007;5(3):604–606.
LeviMTohCHThachilJWatsonHG. Guidelines for the diagnosis and management of disseminated intravascular coagulation. British Committee for Standards in Haematology. Br J Haematol. 2009;145(1):24–33.
4.
MandolfinoTCancigliaATarantoF. Outcome of iatrogenic injuries to the abdominal and pelvic veins. Surg Today. 2008;38(11):1009–1012.
5.
WiedermannCJEgiM. Scoring of disseminated intravascular coagulation (DIC) in intensive care medicine [abstract]. Clin Ther. 2008;159(4):275–281.
6.
BickRL. Disseminated intravascular coagulation: a review of etiology, pathophysiology, diagnosis, and management: guidelines for care. Clin Appl Thromb Hemost. 2002;8(1):1–31.
7.
MatsumotoTWadaHNishiokaY. Frequency of abnormal biphasic aPTT clot waveforms in patients with underlying disorders associated with disseminated intravascular coagulation. Clin Appl Thromb Hemost. 2006;12(2):185–192.
8.
KanekoTWadaH. Diagnostic criteria and laboratory tests for disseminated intravascular coagulation. J Clin Exp Hematop. 2011;51(2):67–76.
9.
BakhtiariKMeijersJCde JongeELeviM. Prospective validation of the International Society of Thrombosis and Haemostasis scoring system for disseminated intravascular coagulation. Crit Care Med. 2004;32(12):2416–2421.
10.
GrisJCFaillieJLCochery-NouvellonELissalde-LavigneGLefrantJY. ISTH overt disseminated intravascular coagulation score in patients with septic shock: automated immunoturbidimetric soluble fibrin assay vs. d-dimer assay. J Thromb Haemost. 2011;9(6):1252–1255.
11.
CauchiePCauchieCBoudjeltaKZ. Diagnosis and prognosis of overt disseminated intravascular coagulation in a general hospital-meaning of the ISTH score system, fibrin monomers and lipoprotein-C-reactive protein complex formation. Am J Hematol. 2006;81(6):414–419.
12.
DhainautJFYanSBJoyceDE. Treatment effects of drotrecogin alfa (activated) in patients with severe sepsis with or without overt disseminated intravascular coagulation. J Thromb Haemost. 2004;2(11):1924–1933.
13.
KienastJJuersMWiedermannCJ. Treatment effects of high-dose antithrombin without concomitant heparin in patients with severe sepsis with or without disseminated intravascular coagulation. J Thromb Haemost. 2006;4(1):90–97.
14.
DempfleCEWurstMSmolinskiM. Use of soluble fibrin antigen instead of d-dimer as fibrin-related marker may enhance the prognostic power of the ISTH overt DIC score. Thromb Haemost. 2004;91(4):812–818.
15.
GrisJCBouvierSCochery-NouvellonEFaillieJLLissalde-LavigneGLefrantJY. Fibrin-related markers in patients with septic shock: individual comparison of d-dimers and fibrin monomers impacts on prognosis. Thromb Haemost. 2011;106(6):1228–1230.
16.
ParkSJChiHSChunSHJangSParkCJ. Evaluation of performance including influence by interfering substances of the Innovance d-dimer assay on the Sysmex coagulation analyzer. Ann Clin Lab Sci. 2011;41(1):20–24.
17.
DempfleCEZipsSErgülHHeeneDL; FACT study group. The fibrin assay comparison trial (FACT): correlation of soluble fibrin assays with d-dimer. Thromb Haemost. 2001;86(5):1204–1209.