
Abstract
The previously reported activated intravascular coagulation system in the acute phase of respiratory distress syndrome (RDS) has not been evaluated in the long term. We assessed the activities of coagulation system of a cohort of premature infants with RDS in comparison with healthy premature infants (HPIs), healthy mature infants (HMIs), and pediatric laboratory controls over a 6-month period. Cord and venous blood samples were taken at birth, at the first month and sixth month. Protein C (PC), free protein S (f-PS), and antithrombin (AT) activities, thrombin–antithrombin (TAT) complex, prothrombin fragment 1 + 2 (PF1 + 2), and fibrinogen levels were measured. Mean PC, f-PS,
Introduction
Proteins that have anticoagulant activity such as protein C (PC), free protein S (f-PS), and antithrombin (AT) are low in neonates but increase to normal levels within months. 1,2 Neonates have a delicate balance of hemostasis with low levels of anticoagulant and fibrinolytic activity and a significantly increased tendency to thrombosis. An intravascular thrombosis may lead to further decrease in these proteins and fibrinogen levels due to consumption. 3 –5 Activated coagulation system is confirmed with high levels of thrombin–antithrombin (TAT) complex and prothrombin fragment 1 + 2 (PF1 + 2). 6 Disorders such as respiratory distress syndrome (RDS), sepsis, and pulmonary hypertension may easily trigger a coagulative state. 1,2,7
Respiratory distress syndrome (RDS) is an acute pulmonary disorder occurring as a result of surfactant deficiency in immature lungs. 3 On the other hand, fibrin polymerization in extravascular compartment of the lungs may inhibit surfactant function. Interstitial and alveolar fibrin deposition as well as thrombin formation could increase inflammation and fibrosis, which in turn might contribute to the development of chronic pulmonary disease. 8,9 Activation of intravascular coagulation system also plays an important role in the pathogenesis of RDS and has a good correlation with the disease severity. Abnormalities in the fibrinolytic system seem to facilitate the deleterious effects of activated coagulation. 4,10 –12 There have been a limited number of studies on premature infants with RDS, evaluating coagulation and fibrinolytic system activation during the active RDS period. 4,5,7,10,13 However, there is no follow-up study in the current literature evaluating those patients following the active period of the disease.
This study aimed to assess the coagulation parameters of a cohort of premature infants with RDS in comparison with healthy premature and mature infants over a 6-month period.
Materials and Methods
Healthy premature infants (HPIs) and healthy mature infants (HMIs) born at Obstetrics Department of Ege University Hospital, as well as premature infants with RDS who were admitted to the neonatal intensive care unit of Ege University Hospital during the study period were enrolled into the study.
Healthy mature infant group consisted a total of 10 mature infants (5 males and 5 females) delivered at 38 to 40 weeks (mean 38.8 ± 0.42 weeks) of gestational age. A total of 11 (6 male and 5 female) infants delivered at 29 to 35 weeks (mean 32 ± 1.7 weeks) of gestational age formed the HPI group. Premature RDS group consisted of 13 (7 male and 6 female) infants delivered at 28 to 31 weeks (mean 29.5 ± 1.2 weeks) of gestational age. Respiratory distress syndrome was diagnosed by reticulogranular appearance in chest x-ray and arterial blood gas findings. Patients with severe RDS with an arterial to alveolar partial oxygen tension ratio of <0.22 were included in the study. 3 They were treated with surfactant and mechanical ventilation according to service protocols. The laboratory normal values of coagulation studies were obtained by enrolling 50 healthy children between the ages of 2 and 15 years, followed at Ege University Healthy Children Outpatient Clinic (control).
The criteria for exclusion were sepsis, metabolic disorders, congenital malformations, chromosomal abnormalities, congenital infection, cyanotic heart diseases, and clinically suspected venous thrombosis. During the course of the study, 3 infants (2 male and 1 female) in premature infant RDS group had a positive blood culture (coagulase-negative staphylococcus). These infants diagnosed with bacterial sepsis were excluded from the study. The demographic and perinatal characteristics of the study groups were summarized in Table 1 .
Demographic Characteristics of the Study Group Infants.
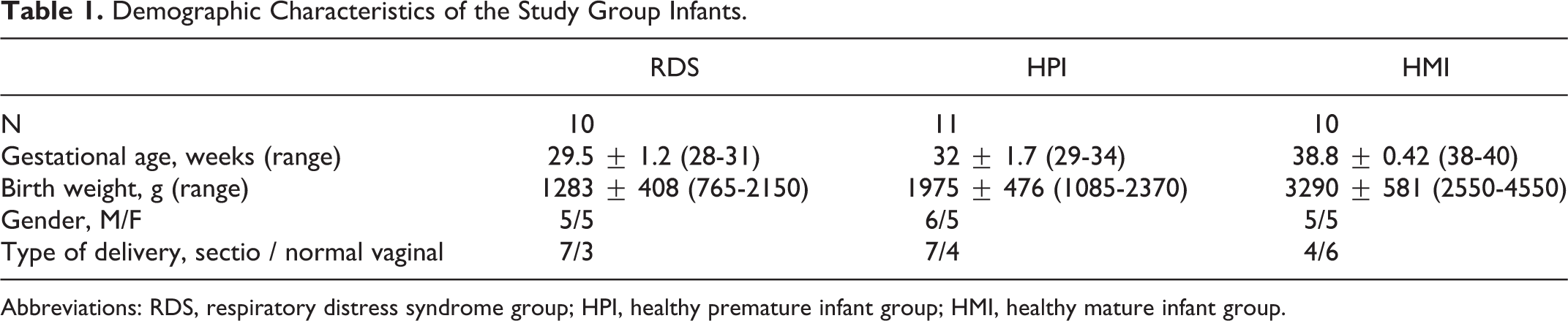
Abbreviations: RDS, respiratory distress syndrome group; HPI, healthy premature infant group; HMI, healthy mature infant group.
The study was approved by the Ethical Committee of the Ege University Medical Faculty, and parental informed consent was obtained.
Cord blood samples taken at birth were established to be the baseline values. Intravenous citrated blood samples were obtained with needle without using a tourniquet at the end of first and sixth month. The plasma samples were stored at −80°C for a maximum period of 3 months. Protein C, f-PS and AT activities, TAT, PF1 + 2, fibrin fragment D (
The baseline, the first month, and sixth month PC, f-PS, AT activities, fibrinogen,
The SPSS-15 package program was used for the statistical analysis. Results were expressed as mean ± standard deviation. Wilcoxon rank test, χ2, and Fischer exact tests were used to compare the study groups. P value less than .05 was considered significant.
Results
Mean baseline AT and PC activities were significantly lower in the HPI group than those of the HMI group but became similar after the first month. Fibrinogen,
The Anticoagulant Activities and Markers for Thrombin Formation in the Study Groups.a
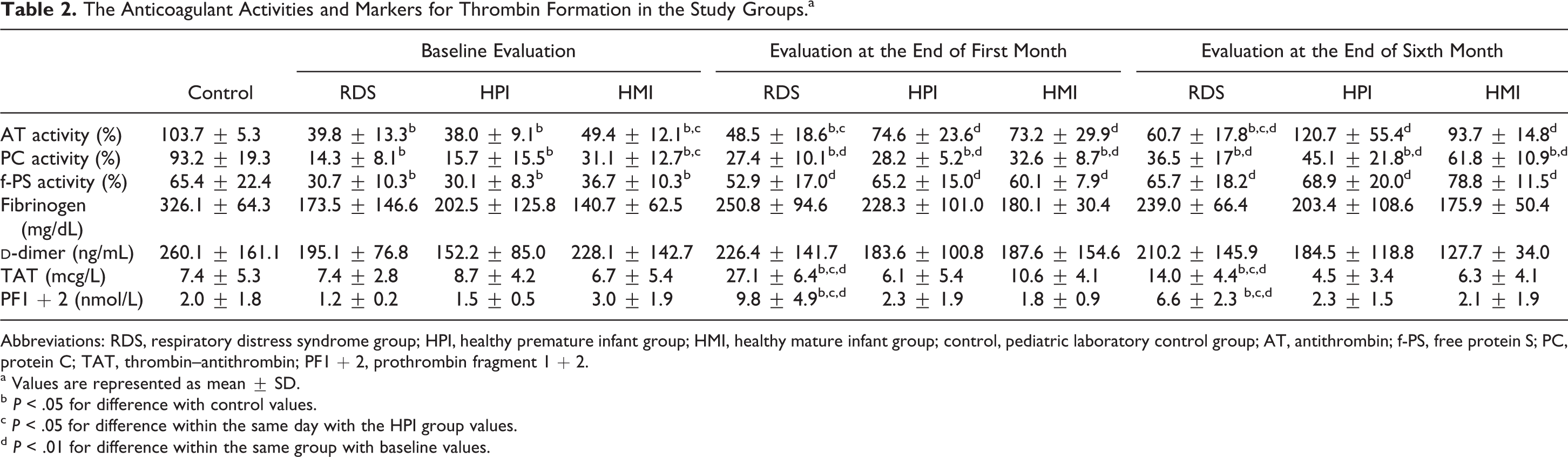
Abbreviations: RDS, respiratory distress syndrome group; HPI, healthy premature infant group; HMI, healthy mature infant group; control, pediatric laboratory control group; AT, antithrombin; f-PS, free protein S; PC, protein C; TAT, thrombin–antithrombin; PF1 + 2, prothrombin fragment 1 + 2.
a Values are represented as mean ± SD.
b P < .05 for difference with control values.
c P < .05 for difference within the same day with the HPI group values.
d P < .01 for difference within the same group with baseline values.
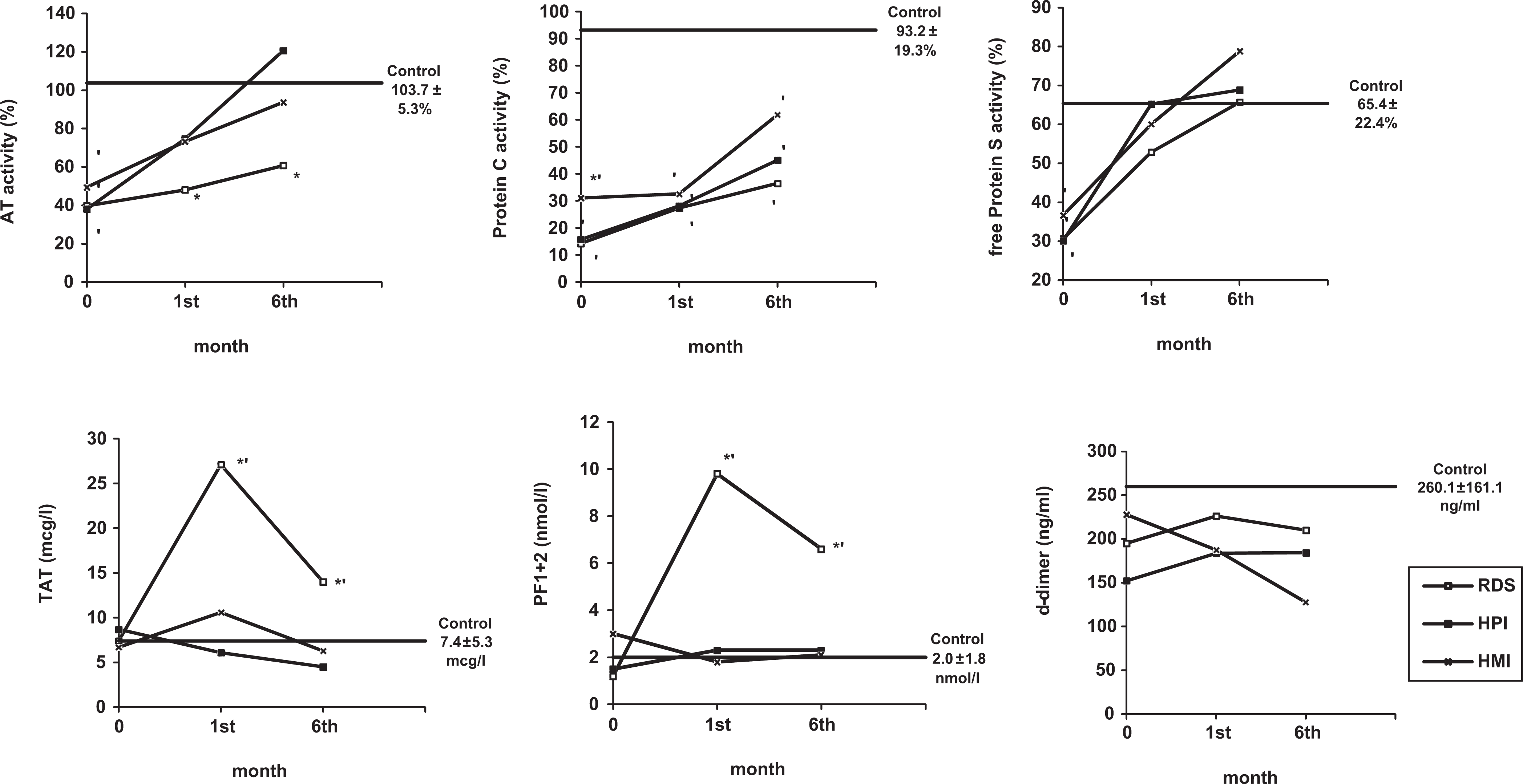
Changes in the activities of anticoagulants and levels of the markers for thrombin formation in the patients with respiratory distress syndrome (RDS), healthy mature infant (HMI), healthy premature infant (HPI), and pediatric laboratory control (control). *P < .05 for difference within the same day in the HMI group; ′P < .05 for difference with control group.
When comparing HPI and RDS groups, the mean values of
Mean PC, f-PS, and AT activities increased significantly in all groups by the sixth month with respect to the baseline values but the fibrinogen and
Baseline PC, f-PS, and AT activities were significantly lower than the laboratory normal values for pediatric patients in all 3 study groups. Especially, PC activity remained significantly lower at the sixth month but the mean f-PS activities reached to normal levels at the first month in all 3 study groups. Antithrombin activity also reached the pediatric laboratory normal values at the first month in HPI and HMI groups but remained significantly lower in RDS group (Table 2; Figure 1).
Discussion
Newborns have a physiologic hypofunction in anticoagulant and fibrinolytic systems and under pathologic conditions the hemostatic balance may easily turn in favor of thrombosis. Spontaneous thromboembolic events are much more frequent in neonatal period than any other period in life, which is explained by the activation of coagulation during birth. 14 –16
In the present study, neonatal baseline PC, f-PS, and AT activities were significantly lower both in healthy premature and mature infants when compared to healthy pediatric controls. Mean PC, f-PS, and AT activities increased significantly by the sixth month with respect to baseline values in all study groups. Mean f-PS and AT activities reached the pediatric normal levels at the first month; however, PC activity remained significantly lower even at the sixth month. In HPIs, only the mean baseline AT and PC activities were significantly lower than the mature infants but reached similar values at the first month.
In premature infants with severe RDS, extravascular and intravascular fibrin depositions related with the activation of coagulation system are reported. This activation may lead to the consumption of coagulation factors and lower levels of fibrinogen, PC, f-PS, and AT. Fibrin itself initiates the fibrinolytic activity which degrades fibrin to
Decreased AT and increased TAT and PF1 + 2 levels are reported in the active period of RDS. Peters et al 11 report that very low levels of AT are associated with poor outcome in newborn infants with RDS. A prospective study on 81 premature infants indicates that low levels of AT are highly suggestive for RDS in premature infants less than 30 weeks of gestational age. 21 Schmidt et al 12 report higher TAT levels and lower AT activities in the patients with severe RDS and conclude that these findings are consistent with increased thrombin formation resulting in AT consumption. 6
We did not observe any significant differences between the RDS and HPI groups regarding the cord blood PC, f-PS, AT activities and TAT, PF 1 + 2, fibrinogen, and
Our study did not aim to investigate the well-defined effects of RDS on the coagulation system during the acute stage, but a prospective observation for the same patients since there is no prospective cohort study showing the long-term outcome of this pathologic hemostatic state. In our study, AT activity values of the RDS group increased significantly by sixth month when compared with the baseline values; however, they were still significantly lower than those of the HPI and laboratory pediatric controls both at the first and sixth month. The TAT and PF1 + 2 values of the RDS group were significantly higher than HPI and HMI groups at the first month. Despite a slight decrease in these parameters, the difference with control groups remained significant throughout the 6-month study period, showing a higher tendency for thrombin generation in infants who previously had RDS. These findings may be explained by an ongoing low stage coagulopathy which develops in the active stage of RDS, with only a slight resolution. Antithrombin activity levels increase with time but never reach the levels of HPI group because of this ongoing consumption of coagulation factors. So, the AT levels of HPI group increased more rapidly between 1 and 6 months of postnatal age, and they were significantly higher at 6 months when compared to HMI group. This may be due to the smaller postconceptional ages of HPI group at 6 months, and we may speculate that these high levels would return to similar ranges of HMI and control group in the same postconceptional age of 6 months. However, larger scale studies may be helpful to confirm our findings.
It is more appropriate to evaluate this report that involves a limited number of cases, as a preliminary analysis of an ongoing prospective study. Since the study population consists of sick premature infants, we could not collect blood samples in the acute stage of severe RDS. Therefore, the cord blood and the first and sixth month samples were prospectively evaluated.
However, this study demonstrated for the first time in the literature that elevated TAT and PF1 + 2 levels and decreased activity of AT, which shows an activation of coagulation system resulting in consumption coagulopathy during RDS were not confined to the active period of the disease and that they in fact carried on after the disappearance of the symptoms for the next 6 months. Further studies including other parameters of coagulant, anticoagulant, and fibrinolytic system including both acute phase and long-term analysis of larger groups of patients are necessary to confirm these results.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.