
Abstract
Background:
Cyclooxygenase 1 (COX-1), COX-2, and HO-1 are involved in the process of aspirin’s effect. The genetic susceptibility of these enzymes to aspirin resistance (AR) is unclear. Methods: A total of 431 patients took aspirin. Using arachidonic acid-induced light transmittance aggregation combined with adenosine diphosphate-induced light transmittance aggregation, 36 participants served for AR, 164 participants for semi-AR, and 231 participants for aspirin sensitivity (AS). The AR with 9 single-nucleotide polymorphism in COX-1, COX-2, and HO-1 genes was investigated.
Results:
COX-1 rs1330344 (−1676A>G) is associated with AR. G-Allele carriers significantly increased the risk of AR. For patients with AS as control, P is .02 (odds ratio [OR] = 1.77, confidence interval [CI]: 1.07-2.92). For patients with semi-AR as control, P is .05. HO-1 rs2071746 (−413A>T) is associated with AR. T-Allele carriers significantly increased the risk of AR. For patients with AS as control, P is .04 (OR = 1.70, CI: 1.02-2.79). For patients with semi-AR as control, P is .05 (OR = 1.68, CI: 1.00-2.80).
Conclusion:
rs2071746 in HO-1 gene, rs1330344 in COX-1 gene contribute to AR.
Keywords
Introduction
Nowadays, atherothrombotic diseases have become the leading cause of death in elderly Chinese. Aspirin is still the cornerstone of treatment and prevention for these diseases. 1 However, epidemiological surveys 2 have discovered that 0.4% to 70.1% patients are poor response to aspirin application, known as aspirin resistance (AR). Platelet aggregation measured by platelet function tests cannot be effectively inhibited after taking aspirin, known as laboratory AR. Prospective analysis in clinical events has shown that patients with laboratory AR have an increased risk of adverse clinical outcomes. 3 –6 Therefore, investigating the mechanism of laboratory AR may aid in the clinical use of aspirin. The Framingham heart study found that the heritable factors are the key determinants for platelet aggregation. 7 We hypothesized that the genetic susceptibility may be the key to aspirin sensitivity (AS), despite other acquired determinants.
For aspirin-resistance genetic screening, the methods used to describe the phenotype must be reliable. Aspirin is a nonselective and irreversible inhibitor of cyclooxygenase (COX), which exists in 2 main isoforms, COX-1 and COX-2. The antiplatelet effect of aspirin is recognized as being due to the irreversible inhibition of platelet COX-1 and reduction in thromboxane A2 (TXA2) production. This function can be detected by arachidonic acid (AA)-induced light transmittance aggregometry (LTA) in vitro, which is regarded as “gold standard.” 8 However, another study found that the adenosine diphosphate (ADP)-dependent pathway allows platelets to remain active in some aspirin-treated patients. 9 Thus in our study, AA-induced light transmittance aggregation combined with ADP-induced light transmittance aggregation was selected for screening AR phenotype.
Hemoxygenase-1 (HO-1) is another enzyme that has been shown to be involved in the antithrombotic effects of aspirin. 10 Therefore, we proposed that genetic variants of HO-1, in addition to COX-1 and COX-2, might also determine aspirin responsiveness. The genetic polymorphisms of these 3 enzymes might be involved in AR. We screened these 3 genes for polymorphisms looking at 9 single-nucleotide polymorphisms (SNPs) with the Sequenom iPlex platform.
Methods
Patients
For this study, information and DNA samples were obtained from consecutive patients who presented between April 2008 and June 2010 and took part in physical examination every year in Chinese PLA General hospital, Beijing 309 hospital, and Navy General Hospital in Beijing with coronary artery disease (CAD), stroke, and peripheral arterial occlusive disease (PAOD) who had been receiving regular aspirin therapy (75-160 mg daily) for at least 4 weeks. Inclusion criteria were ≥65 years of age. Exclusion criteria included the use of clopidogrel, ticlopidine, dipyridamole, or other nonsteroidal anti-inflammatory drugs, heparin or low-molecular-weight heparin; acute vascular events; platelet count <150 000 000/L or >450 000 000/L; and hemoglobin <8 g/dL. Any patients that admitted noncompliance or intermittent compliance were excluded from the analyses. The study was approved by the Scientific and Ethics Review Board of the First Geriatric Cardiology Division, Chinese PLA General Hospital (Beijing, People’s Republic of China). All patients provided written informed consent before inclusion in the study.
Following the screening procedures, 431 patients on aspirin therapy were enrolled. By the LTA diagnostic criteria detailed below, there were 36 patients with AR, 164 patients were partial AR or semi-AR, and 231 patients with AS. These 3 groups are comparable.
Blood Sampling
Blood samples were obtained from patients between 7
Light Transmittance Aggregation
Platelet aggregation was assessed in platelet-rich plasma at 37°C by LTA. Samples were centrifuged at 800 rpm for 5 minutes to obtain native platelet-rich plasma. The platelet count was assessed using a standard cell counter. Platelet-poor plasma was obtained by the centrifugation of remaining blood at 4000 rpm at room temperature for 8 minutes. Aggregation was measured with a ChronoLog Aggregometer (Chronolog, Havertown, Pennsylvania). Aggregation was expressed as the maximal percentage change in light transmittance from baseline after the addition of AA (0.5 mmol/L) and ADP (10 μmol/L), with platelet-poor plasma used as the reference. On the basis of this platelet aggregation assay, the definition of AR was the aggregation of ≥70% with 10 μmol/L ADP and of ≥20% with 0.5 mg/mL AA. 9,11 Aspirin sensitivity was indicated by neither of these criteria being met; AR by both criteria being met; only one of the 2 criteria met was deemed partial AR or semi-AR.
Single-Nucleotide Polymorphism Detection
DNA samples were extracted from peripheral blood obtained from all the patients with AR and AS by a standard phenol–chloroform method. The SNP detection was performed by the use of the Sequenom MassARRAY iPLEX platform (Sequenom, California and USA). 12 The assay consists of an initial locus-specific polymerase chain reaction (PCR), followed by single-base extension that uses mass-modified dideoxynucleotide terminators of an oligonucleotide primer. The PCR primers and single-base extension probes were designed by the Assay Design 3.1 software from Sequenom. The genes and their respective haplotypes as well as the primer pairs and probes are listed in Table 1 . The SNPs were genotyped by the Sequenom MassArray system according to the instructions of the manufacturer. The PCR was performed using iPlex chemistry according to the recommendations of the manufacturer as found in the MassArray iPlex standard operating procedure. Data analysis was performed with the MassArray Typer software version 4.0.
Details of the Primers and Probes for the Candidate Genes.
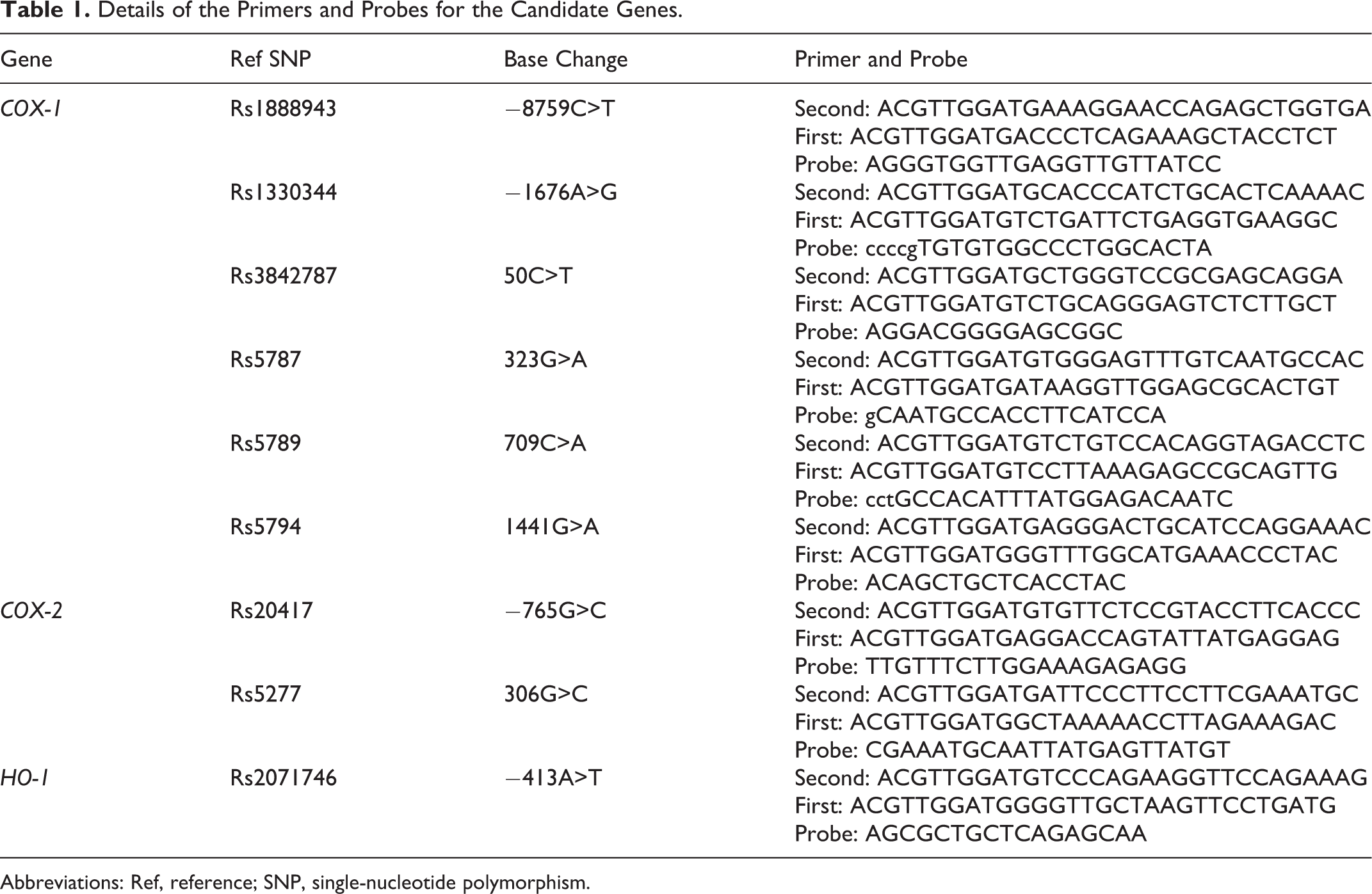
Abbreviations: Ref, reference; SNP, single-nucleotide polymorphism.
Statistical Analysis
Comparisons of the continuous variables were made using the analysis of variance (ANOVA) test or Wilcoxon rank sum test, dependent upon the distribution of the data. Normal data are presented as mean ± standard deviation, data of skewness distribution are presented as median (Q R), Q R = Q 3 − Q 1. All SNPs evaluated in this study were tested for deviation from the Hardy-Weinberg equilibrium with the use of a chi-square test by Haploview 4.2 software. Genotype and allele differences between the SNPs used Pearson chi-square test or Fisher exact test by THESIS software. The associations between HO-1 polymorphisms, COX-1 polymorphisms, and AR were analyzed in logistic regression models after the adjustment of age and gender by SNPstats in Web. The odds ratio (OR) and 95% confidence interval (CI) were used to estimate the associations of allele, genotype, and haplotype between the case and control. P < .05 was considered statistically significant.
Results
Characteristics of the Patients
The study analysis included 431 patients on aspirin therapy. Baseline clinical characteristics are shown in Table 2 . Based on the criteria of the AA-induced aggregation and ADP-induced aggregation, 231 (53.60%) patients were shown to be sensitive to aspirin, while 164 (38.05%) patients were classified as semi-AR and 36 (8.35%) patients were classified as AR. These 3 groups were comparable. No significant differences were found among the 3 groups with respect to age, sex, body mass index (BMI), smoking habits, alcohol, hypertension, CAD, cerebrovascular disease, PAOD, use of calcium-channel blockers, platelet count, Blood urea nitrogen (BUN), creatinine, glucose, cholesterol, high density lipoprotein (HDL), low-density lipoprotein (LDL), HCY, hs-CRP, ATIII activity, PAC-1, and CD62P. In contrast, a significant difference was observed in those patients who take angiotensin-converting enzyme inhibitors/angiotensin receptor blockers (P = .014) and nitrates (P = .003).
Demographic Details for the Patients.
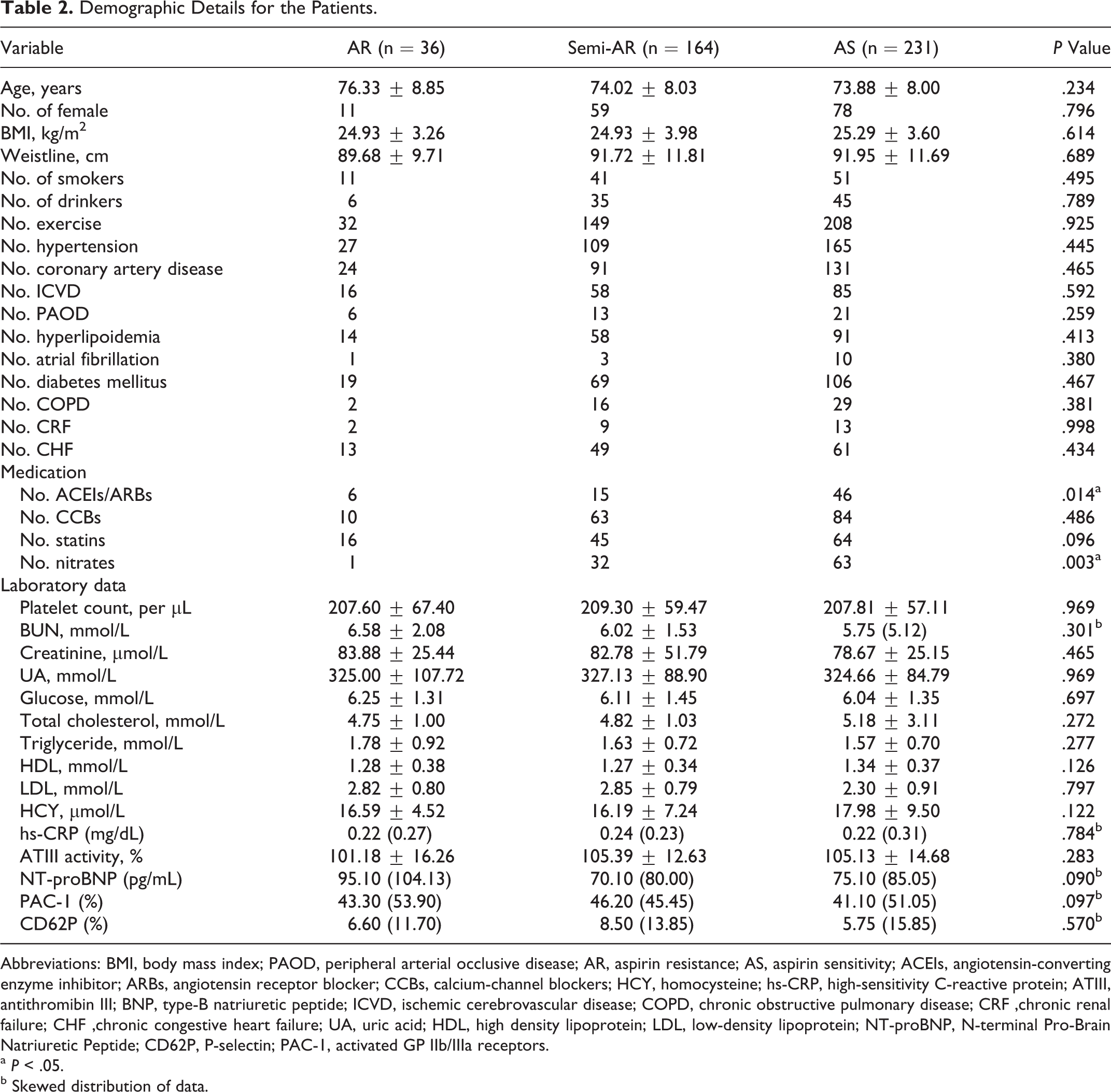
Abbreviations: BMI, body mass index; PAOD, peripheral arterial occlusive disease; AR, aspirin resistance; AS, aspirin sensitivity; ACEIs, angiotensin-converting enzyme inhibitor; ARBs, angiotensin receptor blocker; CCBs, calcium-channel blockers; HCY, homocysteine; hs-CRP, high-sensitivity C-reactive protein; ATIII, antithromibin III; BNP, type-B natriuretic peptide; ICVD, ischemic cerebrovascular disease; COPD, chronic obstructive pulmonary disease; CRF ,chronic renal failure; CHF ,chronic congestive heart failure; UA, uric acid; HDL, high density lipoprotein; LDL, low-density lipoprotein; NT-proBNP, N-terminal Pro-Brain Natriuretic Peptide; CD62P, P-selectin; PAC-1, activated GP IIb/IIIa receptors.
a P < .05.
b Skewed distribution of data.
Allelic and Genotype Frequencies
The allelic and genotypic frequencies of COX-1_rs1888943, COX-1_rs3842787, COX-1_rs5787, COX-1_rs5789, COX-1_rs5794, COX-2_rs5277, and COX-2_rs20417 variants did not differ significantly among all the patients with AR, semi-AR, and AS. However, between the patients with AR and AS or with semi-AR, the frequencies of the COX-1_rs1330344 variant alleles, HO-1_rs2071746 variant alleles, and HO-1_rs2071746 variant genotypes differed significantly (Table 3 ).
Distribution of SNPs in HO-1, COX-1 and COX-2 Genes Among the 3 Groups.
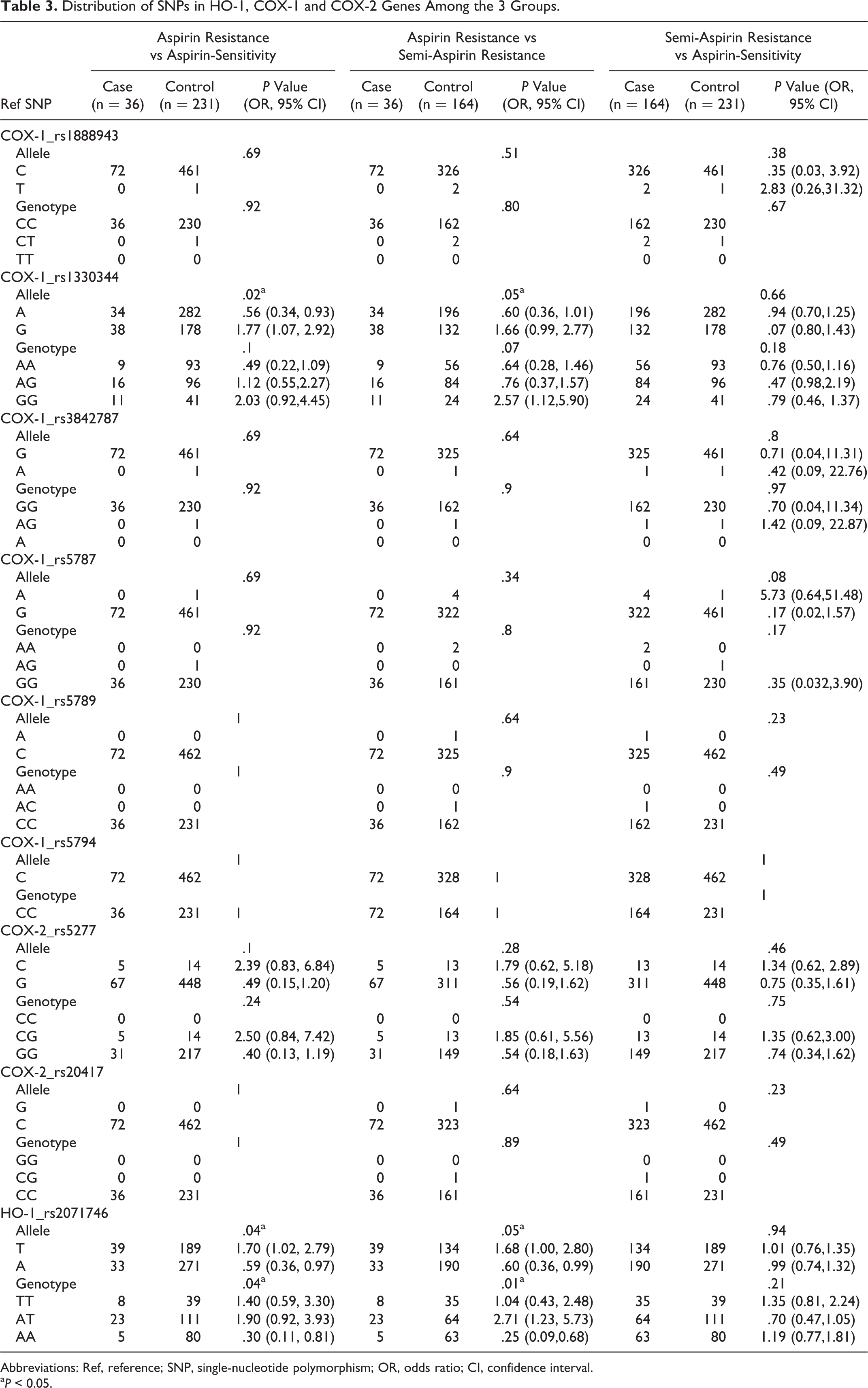
Abbreviations: Ref, reference; SNP, single-nucleotide polymorphism; OR, odds ratio; CI, confidence interval.
a P < 0.05.
HO-1 rs2071746 (−413A>T) Associated With AR
The T allele of HO-1 in rs2071746 (−413A>T) was associated with AR, when compared with not only AS patients but also with semi-AR patients (P = .04 and .05; OR = 1.70 and 1.68; CI = [1.02, 2.79] and [1.00, 2.80], respectively). In contrast, the T allele in rs2071746 (−413A>T) was not associated with semi-AR (P = .94, OR = 1.01, CI = [0.76, 1.35]), when compared with patients with AS (Table 3). Patients who were homozygous or heterozygous for the T allele were significantly more likely to have aspirin resistance (genotype AT or TT) in the HO-1 gene compared with the AA wild-type genotype, the AT and TT genotypes significantly increased the risk of AR, while patients with AS acting as a control, P is .0077 (OR = 3.31, CI = [1.24-8.83]); adjusted by age and sex, P is .0058 (OR = 3.47, CI = [1.29-9.34]). Patients with Semi-AR acting as a control, P is .0024 (OR = 3.95, CI = [1.46-10.68]); adjusted by age and sex, P is .0022 (OR = 4.03, CI = [1.48-10.96]; Table 4 ).
Genotype of rs2071746 (A>T) Responses to Aspirin Resistance.
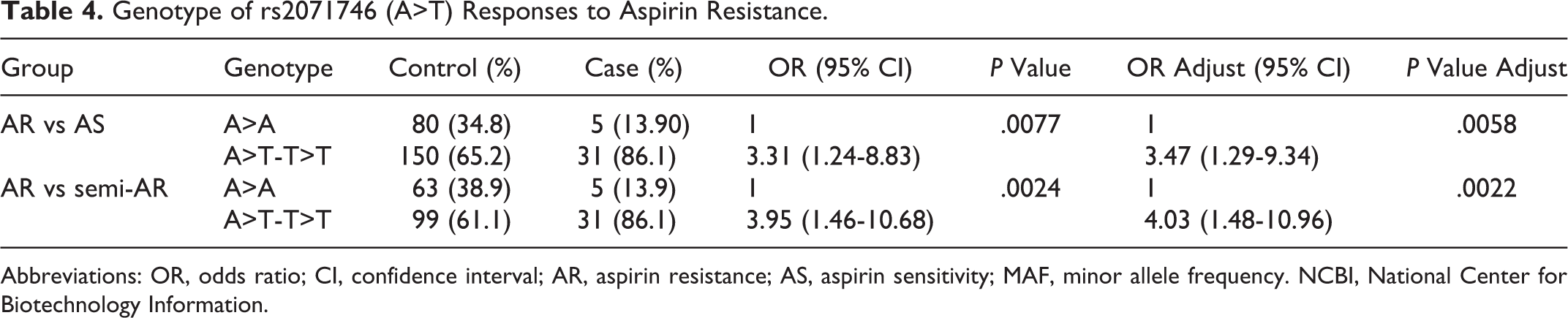
Abbreviations: OR, odds ratio; CI, confidence interval; AR, aspirin resistance; AS, aspirin sensitivity; MAF, minor allele frequency. NCBI, National Center for Biotechnology Information.
COX-1 rs1330344 (−1676A>G) Associated With AR
The G allele of COX-1 rs1330344 (−1676A>G) was associated with AR, when compared with not only the AS patients but also with semi-AR patients (P = .02 and .05, OR = 1.77 and 1.66, CI = [1.07, 2.92] and [0.99, 2.77], respectively]). In contrast, the G allele of COX-1 rs1330344 (−1676A>G) was not associated with semi-AR, P = .66, OR = 1.07, CI = [0.80, 1.43], when compared with patients with AS (Table 3). However, the P value of genotype frequencies of COX-1 rs1330344 and allele frequencies were not consistent (Table 3). The AA, AG, and GG genotypes showed no differences among the 3 groups. In a recessive genetic model, compared with semi-AR, the GG genotype was significantly associated with aspirin resistance, P = .0032, OR = 2.57, CI = 1.12-5.89, adjusted by age and sex, P = .031, OR = 2.59, CI = 1.12-5.98 (Table 4).
COX-1 Haplotype Associated With AR
Six SNPs in COX-1 were selected. Both rs 1888943 and rs1330344 are in the promoter region of COX-1 gene, the other 5 SNPs in the exons of COX-1 gene (information from http://www.ncbi.nlm.nih.gov/SNP). Besides rs 1330344, the other SNPs are rare in the Chinese Han population (Table 5 ). The COX-1 haplotype is dominated by rs1330344. Patients who carried the variant haplotype CGCGCG in COX-1 gene compared with the COX-1 wild-type haplotype were more likely to have AR. When patients with AS act as control, P = .032, OR = 1.69, CI= 1.05-2.71. When patients with semi-AR act as control, P = .044 OR = 1.72, CI = 1.02-2.92 (Table 6 ).
Information of Selected SNPs in COX-1 Gene.
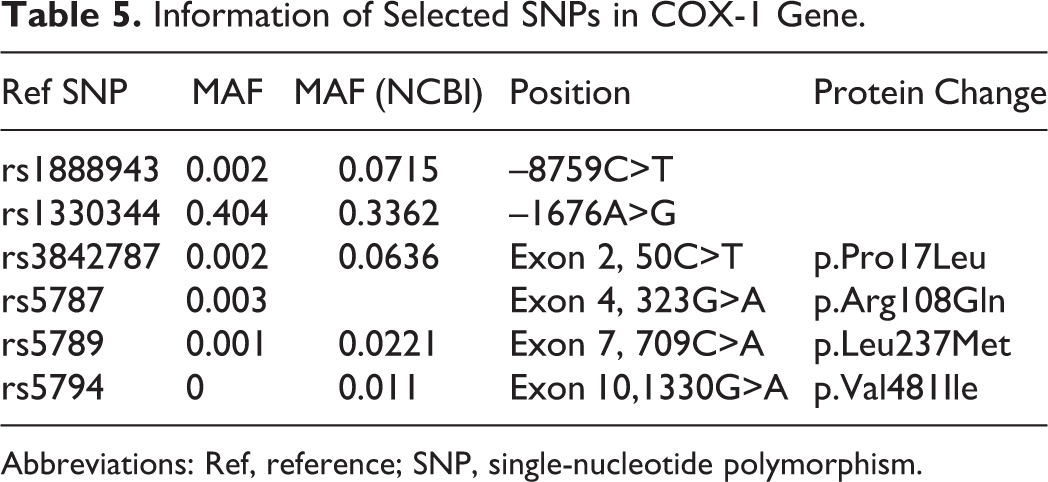
Abbreviations: Ref, reference; SNP, single-nucleotide polymorphism.
COX-1 Haplotype Responses to Aspirin Resistance.

Abbreviations: OR, odds ratio; CI, confidence interval; AR, aspirin resistance; AS, aspirin sensitivity.
COX-2 Genetic Association With AR
The alleles and genotypes of rs5277 and rs20417 showed no differences among the 3 groups (Table 3). The minor allele frequency of rs20417 is also rare in the Chinese Han population.
Discussion
There are plenty of reports about genetic susceptibility to AR. Genetic variants of uridine 5'-diphosphate-glucuronosyltransferase (UGT1A6), cytochrome P450 2C9 (CYP2C9), acyl-CoAsynthetase medium-chain family member 2 (ACSM2), COX-1, COX-2, platelet glycoproteins GPIα, GPIbα, GPIIIbα, ADP platelet receptors P2RY1 and P2RY12 , coagulation factor XIII (FXIII), and TXA2 receptor have been reported in AR. 13 –17 However, the results are poorly reproducible perhaps due to race and different diagnostic methods. To improve the diagnostic specificity of AR, AA-induced LTA combined with ADP-induced LTA was therefore used for this study.
Platelet aggregation at the sites of atherosclerotic plaque plays a role in the thrombosis. COX-1, COX-2, and HO-1 are overexpressed in atherosclerotic lesions, mainly by macrophages and endothelial cells 18,19 and are involved in the process of arterial thrombosis. Due to the lack of a nuclear structure in platelets and the inducible expression properties of HO-1 and COX-2, platelets do not generate COX-2 and generate trace HO-1 in the adult. 20 The COX-1, COX-2, and HO-1 are all target molecules of aspirin. The difference is that COX-1 is constitutively expressed in many tissues and cells including platelets. The sites of action of aspirin on COX-2 were deduced to be in the vascular wall, especially in atherosclerotic plaques (Figure 1). The present study aimed to determine whether previously identified SNPs of COX-1, COX-2, and HO-1 are associated with laboratory AR, which was diagnosed through platelet function test methods in vitro.
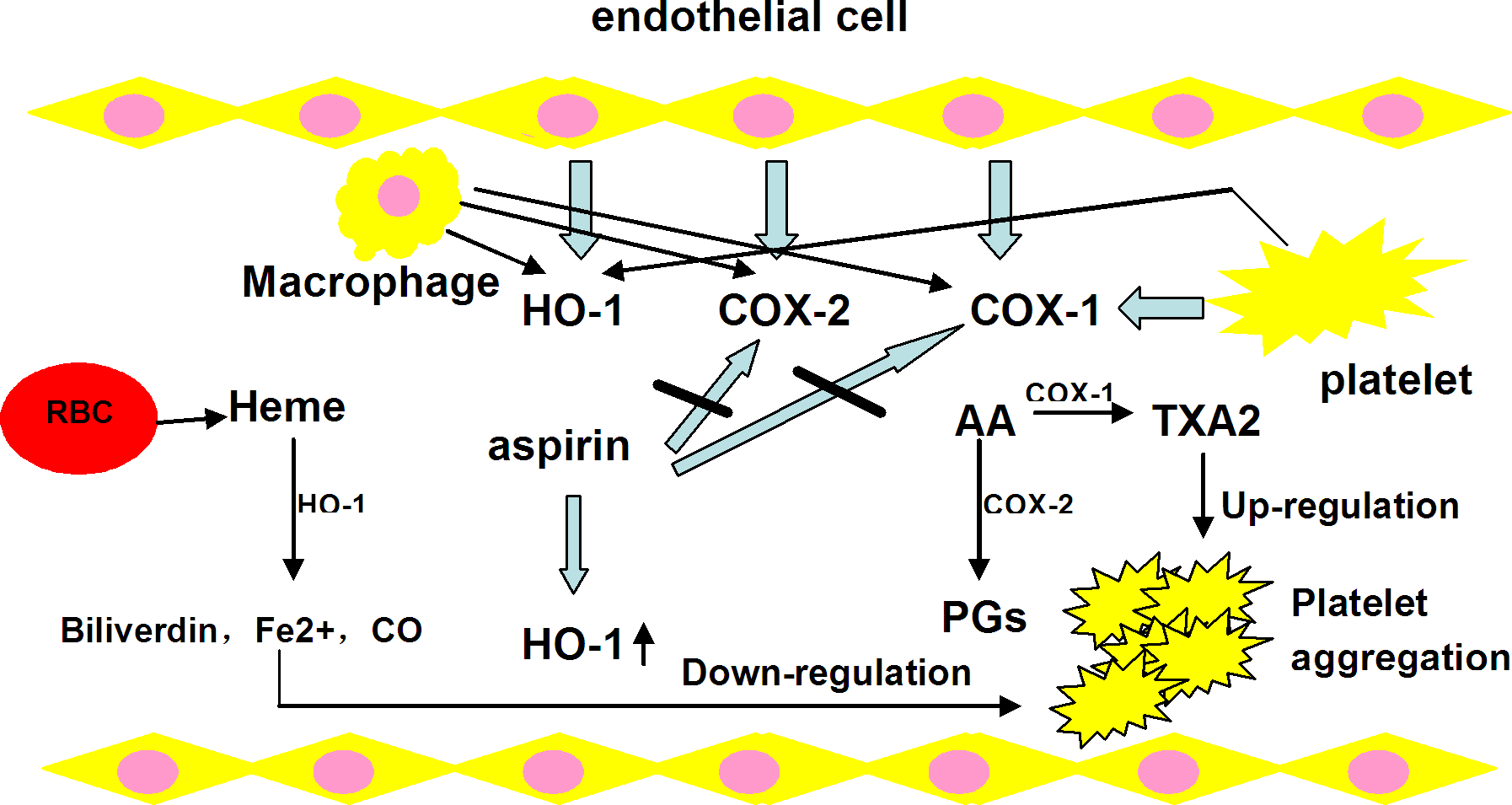
Effects of aspirin via HO-1, COX-1, and COX-2 pathways on platelet aggregation. HO-1 indicates hemoxygenase-1; COX-1/2: cyclooxygenase-1/2.
The highly conserved COX-1 gene serves as house-keeping gene and the function is important to life. The human COX-1 gene encodes more than 20 SNPs, and most of them are rare. 21 The COX-1 gene polymorphisms are of potential importance because individual SNPs or their haplotypes may affect the action of the enzyme as well as its interaction with aspirin. 22 We investigated 6 common SNPs of COX-1 and found that the rs1330344 (−1676A>G) polymorphism of the COX-1 gene promoter and COX-1 haplotype are significantly associated with the development of AR. The promoter −1676 G allele appears to contribute significantly to an AR haplotype. The other 5 SNPs are rare in Chinese Han population. The genetic differences associated with AR significantly vary with race. Data from a review by Agúndez et al suggested that the alleles of COX-1 associated with AR are rs3842787 and rs5789 for European individuals and rs3842789 and rs3842792 for African individuals. 13 Our research shows that rs1330344 has a high prevalence in the Chinese population. The frequency of the minor allele, −1676G is 0.40. The GG homozygosity is associated with AR and occurs in 17.67% of the Chinese Han population (Table 3). In the Japanese population, rs1330344 is also highly prevalent, the −1676C allele has a protective function against functional dyspepsia in Japanese women 23 and −676A is a risk factor for aspirin-induced peptic ulcer in Japanese. 24 On the other hand, the T-1676C promoter polymorphism was reported to be essential for COX-1 transcription. It is, therefore, proposed that G-allele carriers upregulate COX-1 expression and that low-dose aspirin may be an ineffective therapy for GG homozygotes. Another SNP of COX-1, rs3842787 (C50T), which demonstrates complete linkage disequilibrium with the other polymorphism A-842G, is found with minor frequency in Caucasians (8.6%). The C50TPr°–Leu allele, which is present in the signal peptide at position 17, has been depicted as a determinant of pharmacological response to aspirin treatment. However, our study showed the frequency of the minor allele in rs3842787 (50C>T), which was markedly lower (0.2%) in Chinese than in Caucasians. The same result was reported in the Japanese. In our study, the frequency of the minor allele in rs5789 (709C>A) was also markedly lower (0%). Moreover, between the Chinese and Japanese populations, the gene differences for COX-1 are highly consistent. Thus, rs1330344 may be a common tag SNP in COX-1 gene associated with aspirin resistance in Asians.
Unlike COX-1, COX-2 is an induced enzyme, and COX-2 messenger RNA and protein synthesis are induced in a time- and dose-dependent manner in inflammation by endothelial cells and macrophages. Atherosclerosis is now understood to be a disease characterized by inflammation, with chronic inflammation involved at every stage, from initiation to progression and, eventually, plaque rupture. 25 Aspirin is known to exert its anti-inflammatory effects via COX-2. A study by Patrignani et al 26 found that COX-2 is not involved in thromboxane biosynthesis by activated human platelets and consequently argue against the involvement of COX-2-dependent pathway in AR. Our results showed that 2 common genetic variations rs5277 and rs20417 in COX-2 gene are not associated with AR in the Chinese Han population. The rs5277 is also a tag SNP for COX-2, as aspirin is a weak COX-2 inhibitor and the low-dose aspirin perform antiplatelet effect than anti-inflammation. So we deduced that COX-2 gene may not contribute to the pathogenesis of AR in Chinese Han population.
Similar to COX-2, HO-1 is the inducible enzyme that is ubiquitously distributed in mammalian tissues and is upregulated by diverse stimuli, which include inflammatory cytokines and factors that promote oxidative stress. Recent studies have found that HO-1 is a target in the mediation of aspirin-dependent cytoprotective and anti-inflammatory effects. 27 –29 The HO-1 is the rate-limiting enzyme in the oxidative degradation of heme to biliverdin, free iron, and carbon monoxide. The effects of HO-1 are mediated by its metabolites. 30 The HO-1 plays an important role in many aspects of human physiology as well as in pathological events such as atherosclerosis. Reports have demonstrated that the c-Jun N-terminal kinase/activator protein-1 (AP-1) signaling pathway is crucially involved in the anti-inflammatory mechanism of HO-1 associated with aspirin 27 and that the cytoprotective action of HO-1 associated with aspirin is mediated by the nitric oxide/Cyclic Guanosine Monophosphate (NO/cGMP).system in the endothelium. 31 Aspirin induces HO-1 expression in endothelial cells in a COX-independent manner. 28 In 2004, Peng et al showed that the induction of HO-1 expression inhibited platelet-dependent thrombosis through its metabolite. Our study suggests that HO-1 has an impact on platelet aggregation and that a genetic polymorphism is associated with AR.
Studies have shown that the major mammalian stress-responsive transcription factors, heat-shock factor, nuclear factor-erythroid 2, AP-1, and the nuclear factor-κB family members, all regulate the HO-1 gene through binding with the sites located within the HO-1 promoter region and increase HO-1 transcription. 32,33 These findings suggest that the structure of the promoter region is vital to gene expression of HO-1. Determining the association between HO-1 polymorphism and AR was a focus of this study. At present, 2 functional polymorphisms in the HO-1 promoter region, a (GT)n microsatellite and rs2071746 (−413T>A) can regulate transcription capability of HO-1. 33 Both a short (GT)n allele and the A-allele have been associated with increased HO-1 promoter activity. Our data for the first time have shown that AT and TT genotypes of the HO-1 promoter polymorphism rs2071746 (−413A>T) are associated with susceptibility to AR. In fact, gene changes in the HO-1 promoter that impact on aspirin responsiveness are not unique; many studies have demonstrated their impact in a variety of disease states, such as CAD, Alzheimer disease, Parkinson disease, cancer, organ transplantation, infection, diabetes mellitus, autoimmune disorder, and acute respiratory distress syndrome. We presume that more evidence will be discovered about the associations of the HO-1 gene polymorphism and disease, owing to the property of HO-1 being a ubiquitous cell-defensive enzyme. The HO-1 seems to be an integral part of the stress response, 34 and the failure to respond to stressful stimuli via HO-1 induction leads to increased susceptibility to diseases.
Conclusion
We examined the association of genetic polymorphisms with laboratory aspirin resistance determined by AA-induced LTA combined with ADP-induced LTA. Our study demonstrated for the first time that rs2071746 (−413A>T) gene polymorphism in HO-1 and rs1330344 (−1676A>G) gene polymorphism in COX-1 are significantly associated with AR in the elderly Chinese Han population. The rs1330344 is a fairly common allele in the Han population. We were unable to find an association with a COX-2 polymorphism. These findings may guide aspirin antithrombotic therapy in China.
Footnotes
Xiao-li Li and Jian Cao equally contributed for this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: supported by the Healthcare Fund (07BJZ01) and the National Science and Technology Support Project (2009BAI86B04).