
Abstract
Background and Aim:
Pulmonary embolism (PE) is a common and serious disease that can result in death unless emergent diagnosis is made and treatment is initiated. In this study, we aimed to identify whether there is still a delay in the diagnosis of PE and to identify the time to delay in diagnosis and factors leading to this delay.
Methods:
This is a prospective observational cohort study performed in an emergency department (ED) of a tertiary care university hospital between September 2008 and September 2010. The rate and cause of delay in diagnosis were analyzed among patients with PE. The “delay” was defined as diagnosing after first 24 hours of symptom onset.
Results:
Among the 53 patients who were diagnosed with PE, a delay in diagnosis was present in 49 (93%) of them. Total delay time was 6.8 ± 7.7 days. In 33 (62%) patients, there was a delay of 4.6 ± 6.5 days due to patient-related factors. Delay in diagnosis after admission to hospital was 2.2 ± 2.9 days in 40 (75%) patients. In multivariate regression analysis, being female and having chest pain and cough were identified as significant factors causing patient-related delay. Unilateral leg edema, recent operation, and previous venous thromboembolism (VTE) history were the significant factors causing PE diagnosis without a delay. On the other hand, systemic hypertension as comorbidity was the only factor leading to physician-related delay.
Conclusion:
The delay in diagnosis of PE in EDs still remains as an important problem. While being female and having chest pain and cough are significantly and independently associated with patient delay in diagnosis, the unilateral leg edema, recent operation, and previous VTE history cause physicians to diagnose on time. On the other hand, having hypertension as comorbidity may lead to physician delay. In order to prevent the delay in diagnosis, hospital-associated factors must be elucidated totally and more interventions must be made to increase public and professional awareness of the disease.
Introduction
Pulmonary embolism (PE) is a common and serious disease that can result with death unless emergent diagnosis is made and treatment is initiated. Most of the deaths from PE occur within first few hours due to unrecognized, lately diagnosed deep venous thrombosis (DVT), and PE. 1,2 In addition to the acute effects, late diagnosis may lead to the development of pulmonary hypertension in the long term and even eventually may lead to death due to right heart failure, years after the occurrence of PE. 3 Diagnosis of PE is frequently made by being suspicious about the disease. Depending on the clinical and laboratory data and the medical histories of the patients, most of the patients with PE are diagnosed in the emergency departments (EDs) either by a pulmonologist or by an emergency physician. 4
Many factors can play a role in the delayed diagnosis of PE and some limited number of studies has highlighted this issue recently. 5 –12 A delay in the diagnosis of PE can be due to patient-related factors. They may delay in seeking medical attention owing to underrating the symptoms (chest pain and dyspnea), attributing these symptoms to other underlying diseases (chronic obstructive pulmonary disease [COPD] or asthma exacerbation and malignancy) and being unable to express their symptoms due to old age. Although some patients seek medical attention immediately there will be a delay of diagnosis due to accompanying factors such as computed tomography (CT) angiography could not be done because of the acute renal failure or the morbid obesity of the patient or ventilation-perfusion (V/Q) scintigraphy could not be performed owing to other pulmonary diseases such as COPD or pneumonia. Besides, a delay in the diagnosis of PE can be due to physician-related factors. They may erroneously evaluate the symptoms of PE and misdiagnose as pneumonia, acute myocardial infarction (MI), acute congestive heart failure, aortic dissection, pneumothorax or exacerbations of COPD, and asthma. 2 Another factor that may delay the diagnosis of PE is the working hours of the radiology department such as not performing CT angiography or V/Q scintigraphy for 24 hours.
In this study, we aimed to identify whether there is still a delay in the diagnosis of PE in an ED of a university hospital in the last 2 years after the introduction of clinical prediction rules and CT angiography into daily practice. We also aimed to identify the time to delay in diagnosis and factors leading to this delay.
Methods
This study was designed as a prospective observational cohort study. It was performed in an ED of a tertiary care university hospital that is Gazi University Medical Faculty Hospital in Ankara in Turkey, between September 2008 and September 2010. It is a reference hospital where patients are accepted from many other hospitals both from the Ankara district and from many other cities near Ankara. The local ethics committee of our institution had approved the study and signed informed consent was received either from patients or from their relatives (if they were unable to sign) before including in the study.
Patient Selection and Evaluation
Inclusion criteria
All patients who were >18 years old were included in the study if they were diagnosed as having PE in ED by an emergency or pulmonary physician.
Exclusion criteria
Patients who did not accept to be included in the study and who were recently pregnant (<6 months) were excluded from the study.
All patients were first evaluated by paramedics before being accepted to the ED. After being accepted, the patient was evaluated by a resident of ED and by an ED specialist. If they clinically suspect from PE, further tests were planned for the diagnosis of PE directly by the ED physicians. For estimating the pretest clinical probability in the diagnosis of PE, Wells prediction rule was frequently used in our ED. 13 A score between 0 and 1 evaluated as low clinical probability, between 2 and 6 as intermediate clinical probability, and ≥7 as high clinical probability. However, patients' history, physical examination, comorbid diseases, and clinicians' predictions also play a key role in assessing pretest probability. If they have any doubt about the diagnosis, they can ask for consultation with the pulmonologist. Pulmonologists used an algorithm for the diagnosis of PE (Figure 1 ). 14 –17 The test that was preferred at first glance for the diagnosis of PE was a 64-slice multislice CT angiography (General Electric, Light speed VCT, 64 slice) in our university hospital. If CT angiography could not be performed because of morbid obesity or elevated renal function tests, then V/Q scintigraphy or venous Doppler ultrasonography (USG) of lower extremities were used for the diagnosis, according to the algorithm.
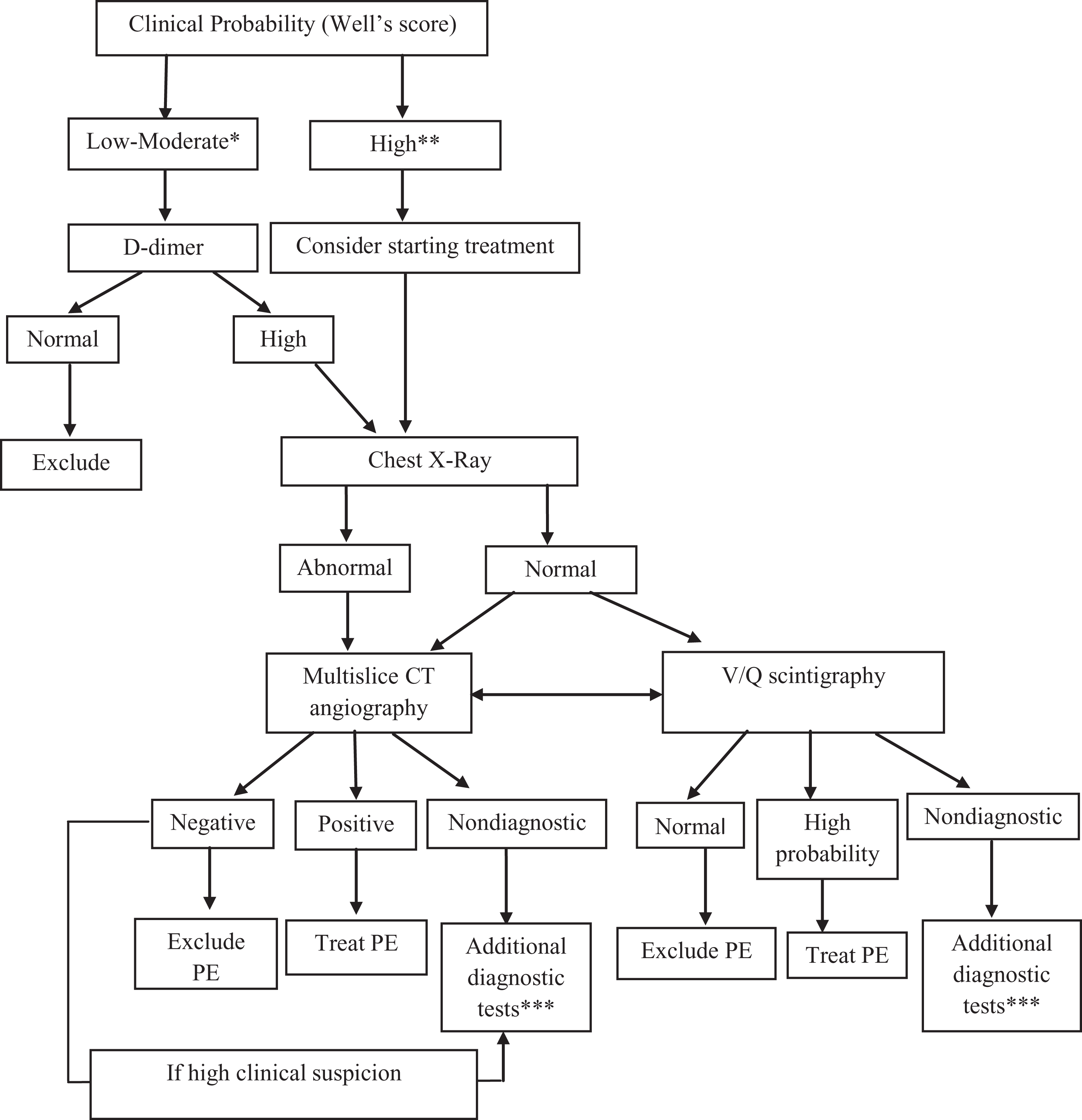
Pulmonary embolism diagnostic algorithm.
All physicians (either from emergency medicine or pulmonary medicine) had decided by themselves to order or not to order for further diagnostic tests of PE. They were not informed about the study and the investigators did not interfere with their decisions.
Data Collection
Following data were recorded for each patient: social and demographic data (age, sex, weight, marital status, living alone or with family, education status), underlying diseases, physical examination, vital findings and symptoms at admission, venous thromboembolism (VTE) risk factors (malignancy, thrombophilia, previous DVT or pulmonary thromboembolism (PTE), immobilization, surgical operation or trauma within the last 4 weeks, pregnancy, etc),
The initiation day of symptoms, the day of admission to hospital, previously consulted hospitals or physicians, previous therapies, the day of diagnosis of PE, and the day of initiating treatment were also recorded. If there was a delay in admission, diagnosis and treatment of PE, the causes of this delay were also recorded.
Definitions
Delay in PE diagnosis due to patient-related factors
In this case, the patient presents to the ED 1 or more days later after the initiation of his or her complaints or symptoms.
Delay in PE diagnosis due to physician-related factors
In this case, a physician orders a diagnostic test for PE 1 or more days after the presentation of the patient to the ED or outpatient clinic.
Delay in PE diagnosis due to hospital-related factors
In this case, the diagnostic tests for PE could not be performed on the same day that the physician ordered, because of the working schedule of the radiology department that is not performing CT angiography or V/Q scintigraphy for 24 hours but for limited time period.
Delay in PE diagnosis after admission to hospital
Apart from the patient-related factors, there is a combination of delay due to physician- and hospital-related factors.
Total delay time for PE
The total delay time for PE includes a combination of the delay from patient-, hospital- and physician-related factors.
Statistics
SPSS for Windows 15.0 software was used for the statistical analysis of the results (SPSS for Windows; Chicago, Illinois). Results are presented as mean ± standard deviation (SD) and percentiles or median (range) values. The independent samples t test, the chi-square, and Mann-Whitney U tests were used for comparison of the categorical and continuous variables. Correlation was investigated with Pearson correlation tests for parametric values. A difference was considered statistically significant when P < .05. Univariate logistic regression analysis was used to identify the risk factors (both patient and physician related) for delay in the diagnosis of PE. Parameters with a P value <.2 were analyzed with multivariate logistic regression analysis.
Results
Patient Characteristics
A total of 120 patients, who were admitted to our ED, were evaluated for the study if there was a suspicion of PE. Among them, 53 (49%) patients diagnosed with PE were included in the study. Demographic and social characteristics and comorbidities of the whole group were summarized in Table 1 .
Demographic, Social Properties, and Comorbidities of the Study Group.

Abbreviations: SD, standard deviation; COPD, chronic obstructive pulmonary disease.
Among the whole study group, 36 (68%) patients were presented first to our ED, 5 (9%) patients to an outpatient clinic of our university, and 12 (23%) patients first presented to another hospital (1 of them to an ED and 11 of them to an outpatient clinic). Thirty-seven (70%) of them were first evaluated by an emergency physician, 6 (11%) by a pulmonologist, 2 (4%) by an internal medicine specialist, 3 (6%) by a general practitioner, and 5 (9%) by other specialists (cardiology, oncology, orthopedics, etc).
Diagnostic Tests
Diagnostic tests were ordered to the entire study group with the suspicion of PE. Thoracic multislice CT angiography was performed in 52 (98%) patients, lower extremity Doppler USG was performed in 4 (8%) patients. Among the whole study group, diagnostic tests were ordered by an emergency medicine resident in 22 (42%), by a pulmonary diseases resident in 27 (51%), by both pulmonary medicine and emergency medicine resident in 2 (4%), and by other physicians in 2 (%4) patients. The reasons for ordering diagnostic tests were high
Delay in Diagnosis
Among the 53 patients with PE, a delay in diagnosis was present in 49 (93%), that is PE diagnosed >1 day after the initiation of symptoms. Mean time of delay was 6.8 ± 7.7 days (median: 4 days, minimum 0 days, and maximum 32 days). In 33 (62%) patients, there was a delay of 4.6 ± 6.5 days (minimum = 0 and maximum = 28 days) due to patient-related factors. In 27 (51%) patients a delay of 0.7 ± 0.9 days (minimum = 0 and maximum = 4 days) was due to hospital-related factors. In 20 (38%) patients a delay due to physician-related factors was 1.5 ± 2.7 days (minimum = 0 and maximum = 12 days). When patient-related delay was completely excluded, delay of 2.2 ± 2.9 days in the diagnosis, due to either hospital-related or physician-related factors, was present in 40 (75%) patients. A delay because of all the 3 factors (patient, hospital, and physician related) was present in 2 (4%) patients. When patient-related delays were concerned, 34% of PE (+) patients had >5 days of delay. When the total delay time for diagnosis is concerned, 20 (38%) patients had >7 days of delay.
The factors that can affect the patient delay were evaluated in Table 2 . Among the demographic characteristics, being single, living alone or in a nursing home, and among the physical findings; higher systolic, diastolic, and mean arterial blood pressure were found as factors significantly contributing to the patient delay (P < .05). In addition to the factors causing patient delay, factors that may affect the physician delay were also investigated and summarized in Table 3 . Low Wells score, unilateral leg swelling, patients having hypertension as a comorbidity, and age >50 were identified as significant factors that affect physician delay (P < .005). Results of multivariate logistic regression analysis both for patient-related delay and for physician-related delay are summarized in Table 4 . Being female and having chest pain and cough as symptoms were identified as significant factors causing patient delay. When the factors related with the physician delay in diagnosing PE were analyzed, leg edema, recent operation, and previous VTE history were found as the significant factors of timely diagnosis but having hypertension as a comorbidity was the only factor found in the multivariate logistic regression analysis that leads physicians to delay (Table 4).
Analysis of the Factors That can Lead to Patient-Related Delay in Patients With Pulmonary Embolism.
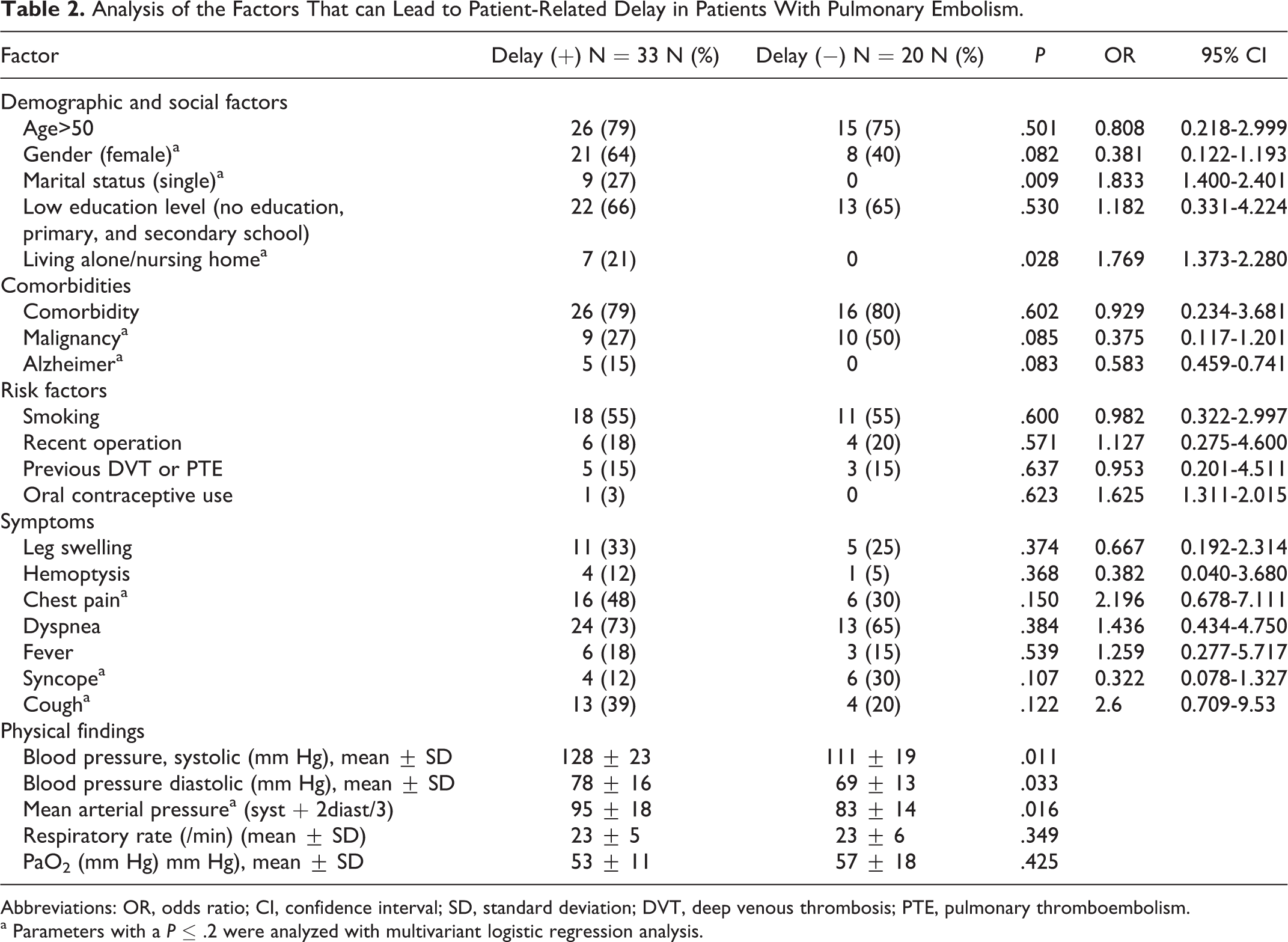
Abbreviations: OR, odds ratio; CI, confidence interval; SD, standard deviation; DVT, deep venous thrombosis; PTE, pulmonary thromboembolism.
a
Analysis of the Factors That can Lead to Physician-Related Delay in Patients With Pulmonary Embolism.
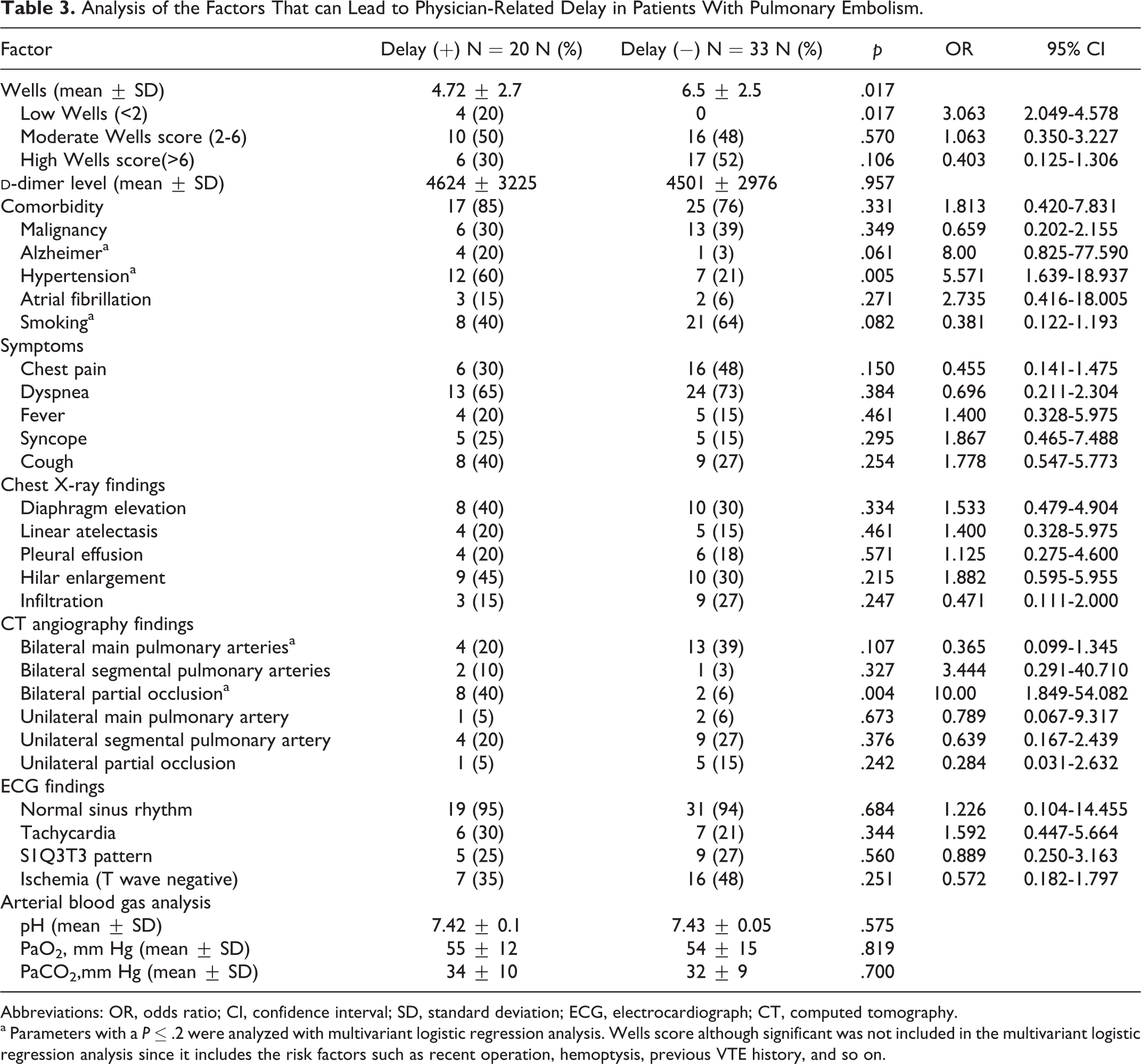
Abbreviations: OR, odds ratio; CI, confidence interval; SD, standard deviation; ECG, electrocardiograph; CT, computed tomography.
a Parameters with a P ≤ .2 were analyzed with multivariant logistic regression analysis. Wells score although significant was not included in the multivariant logistic regression analysis since it includes the risk factors such as recent operation, hemoptysis, previous VTE history, and so on.
Results of Multilogistic Regression Analysis Both for Patient- and Physician-Related Delays.
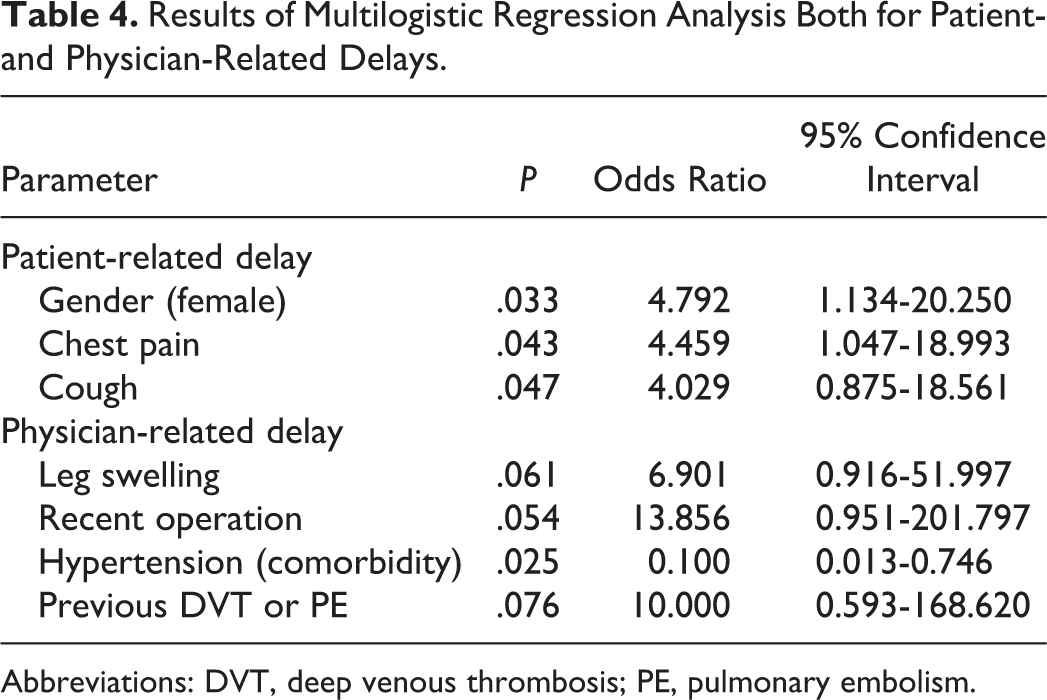
Abbreviations: DVT, deep venous thrombosis; PE, pulmonary embolism.
Discussion
Pulmonary embolism is a common, serious, and potentially fatal disease, and its diagnosis still remains a challenge especially for emergency physicians and also for pulmonary physicians. In the last decade, technology has evolved rapidly and CT angiography has been commonly introduced to our daily practice.
18,19
In addition to this, many algorithms using
In our study, a delay in the diagnosis was present in 49 (93%) patients with acute PE. This high rate of delay was most probably related with our definition that is being diagnosed after first 24 hours of symptom onset. In previous studies, the definition of delay was made as diagnosis after 5 or 7 days of symptom onset; so they reported lower rates of delayed diagnosis. 6,8 –12 When we classify our patients according to their mean time of delay, 34% of PE (+) patients had >5 days of patient-related delay. When the total delay time for diagnosis is concerned, 20 (38%) patients had >7 days of delay. This rate is lower than the rate reported in the study of Ageno et al as 64% of patients being diagnosed in >5 days of symptom onset. 8 But it is known that early diagnosis of VTE and thus early implementation of adequate anticoagulant treatment has the potential to substantially reduce subsequent mortality and morbidity. 23 Kline et al stated in their study that delayed diagnosis is associated with worse outcome in the EDs such as shock, intubation, and death. 7 Hence, we think that it is not true to take the definition of delay as the diagnosis of PE after 5 or 7 days of symptom onset. In order to prevent mortality and morbidity, the diagnosis should be made as soon as possible, especially within the first 24 hours. There are also contrary studies such as that of Jimenez Castro et al, stating that when compared to the others, patients with a diagnostic delay did not have higher risks of recurrent VTE or death during 3 months of follow-up. 6 But they did not look for the long-term results of delayed diagnosis such as chronic thromboembolic pulmonary hypertension.
In our study, in 33 (62%) patients, there was a delay of 4.6 ± 6.5 days (minimum = 0 and maximum = 28 days) due to patient-related factors. Physician-related delay was shorter: 1.5 ± 2.7 days (minimum = 0 and maximum = 12 days) and hospital-related delay was the shortest: 0.7 ± 0.9 days (minimum = 0 and maximum = 4 days). Delay in diagnosis after admission to hospital was 2.2 ± 2.9 days in 40 (75%) patients and the total delay time was 6.8 ± 7.7 days. The consequence of delayed diagnosis of PE was first recognized by Elliott et al. 5 They reported patient-related delay as 3 days and hospital-related delay as 2 days. Their 17% of patients had the diagnosis >1 week later. In the study of Jimenez Castro et al, the effects of this delay in diagnosis on the prognosis was searched and the mean day of delay in diagnosis beginning from the initiation of the symptoms up to the diagnosis was found as 7 days. 6 Like Jimenez Castro et al, 6 a recent study by Ozsu et al also found that the mean time to diagnosis for both medical and surgical patients was approximately as 7 days. 12 The total delay time identified in our study was consistent with these studies. In a recent study by Bulbul et al, 60.3% of patients visited health institution within the first day of symptom onset. 10 According to our definition of delay, they had much lower rate of diagnostic delay when compared with our study. They had also reported a lower patient delay time as 2.4 ± 3.9 days, but longer total delay time as 7.93 ± 10.05 days. They concluded that physician- or health system-related delays were more prominent in their rate of delayed diagnosis. 10 Patient-related delay was the main problem in our study group.
We searched for the factors associated with the patient-related delay. Being a female, being single, and living alone were identified as significant factors increasing the patient delay in the diagnosis. Although statistically not significant, patients with Alzheimer also had a delay in diagnosis since they cannot express their symptoms easily. Again although not statistically significant, patients with low education level delayed more in seeking medical help (63% vs 37%). While having chest pain and cough caused more patient delay, syncope and lower blood pressures caused more rapid admission to hospital. In multivariate regression analysis being female and having chest pain and cough were identified as significant factors causing patient delay. In previous studies it was reported that patients with more severe clinical presentation (syncope, lower blood pressure, tachypnea, fever) presented earlier for diagnosis. 6,8,9 This was also similar in our study. In the only study that evaluated the sociodemographical factors for patient delay, Bulbul et al identified current smoking, a higher education level, and comorbidity were associated with longer patient delay; hypotension, syncope, previous surgery/trauma were associated with shorter patient delay. 10
In previous studies no analysis has been performed to identify the factors for physician-related delays. In our analysis, we identified that unilateral limb edema, recent operation, and previous VTE history were the significant factors causing physician to diagnose on time, without a delay; but having hypertension as comorbidity was the only factor leading to physician delay. It can be speculated that hypertension might mislead the physicians to cardiac causes of dyspnea and chest pain such as decompensated heart failure, acute MI, or aortic dissection. Especially in massive and sometimes in submassive patients with PE, hypotension is expected; so having hypertension might also cause a delay in considering PE as a possible diagnosis.
Another remarkable result of our study was that in 27 (51%) patients there was a delay in diagnosis due to hospital-related factors and when patient-related delay was completely excluded, delay in diagnosis, due to either hospital-related or physician-related factors, was present in 40 (75%) patients. This occurred in our ED because of the working schedule of the radiology department that is not performing CT angiography, V/Q scintigraphy, or lower extremity venous Doppler USG for 24 hours but for limited time period. We believe that it is hard to eliminate the patient- and physician-related delays totally. But with the elucidation of hospital-related delays, earlier diagnosis of acute PE can be possible in 51% of our study population.
There are also some limitations of this study. First, it was performed in a single unit, with low number of patients, so the results cannot be attributed in general. But we believe that it was a good representative of the current status in an ED of a tertiary care university hospital. Second, we also did not follow our patients with PE for the consequences of delayed diagnosis that is how this delay affects the mortality and morbidity of these patients.
As a conclusion, the delay in the diagnosis of PE in EDs still remains as an important problem. This delay can be due to patient-, physician-, and hospital-related factors. Being female and having chest pain and cough were the factors significantly and independently affecting patient delay. The unilateral limb edema, recent operation, and previous VTE history were the significant factors causing physician to diagnose on time, without a delay; but having hypertension as comorbidity was the only factor leading to physician delay. In order to prevent this delay in diagnosis, hospital-associated factors must be elucidated totally and more interventions must be made to increase public and professional awareness of the disease.
Footnotes
Authors’ Note
All authors of this article have no commercial or proprietary interest in any drug, device, or equipment mentioned in the submitted article. All authors have no any financial interest (as a consultant, stock owner, employee, evaluator, etc) in any item mentioned in the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All authors of this manuscript disclose the funding received for this work from the following organizations: National Institutes of Health (NIH), Wellcome Trust, Howard Hughes Medical Institute (HHMI), and other(s).