
Abstract
Aim:
Myocardial bridge is associated with atherosclerosis altered in shear stress and endothelial dysfunction. Mean platelet volume (MPV), a determinant of platelet activation, is shown to be related with atherosclerosis and endothelial dysfunction. In this study, we aimed to evaluate platelet function assessed by MPV in patients with myocardial bridge.
Methods:
Forty-two patients with myocardial bridge in the left anterior descending artery (LAD) and 43 age- and gender-matched healthy participants were included in the study. Myocardial bridging was defined as an intramyocardial systolic compression or milking of a segment of an epicardial coronary artery on angiography. For the entire study population, MPV was measured using an automatic blood counter.
Results:
The study population consisted of 42 patients with myocardial bridge (52.7 ± 10.2, 76.2% male) and 43 age- and sex-matched healthy control participants (52.1 ± 10.4, 74.4% male). Compared to the control group, MPV value was significantly higher in patients with myocardial bridge (8.9 ± 1.24 vs 8.3 ± 0.78; P = .01). Further, there were no significant differences between groups regarding hemoglobin level, platelet count, fasting blood glucose, and creatinine levels.
Conclusions:
Our study findings indicated that myocardial bridge is associated with elevated MPV values. Our results might partly explain the increased cardiovascular events in patients with myocardial bridge.
Keywords
Introduction
Myocardial bridge (MB) is a congenital coronary anomaly, where a segment of the epicardial coronary artery courses intramurally. 1,2 Angiographic prevalence of MB is reported 3 to range from 0.5% to 29.4%. Although it is considered to be a benign, MB may cause ischemia, acute coronary syndrome, coronary spasm, life-threatening arrhythmias, exercise-induced atrioventricular conduction block, sudden cardiac death. 4 –7
It has been indicated that platelet size reflects platelet activity and is measured using mean platelet volume (MPV). 8 Large platelets are more reactive and produce more prothrombotic factors. 9 Myocardial bridge may result in significant alteration in coronary flow hemodynamics. Blood flow-related shear stress has been established as an important influence on endothelial function. 10 To our knowledge, no study has assessed platelet activation using MPV measurement in patients with MB. We hypothesized that impaired coronary flow in MB segment and endothelial dysfunction may induce platelet activation in patients with MB. Therefore, the aim of this study was to measure MPV values in patients with MB to evaluate platelet activation.
Materials and Methods
Study Population
Forty-two patients with MB in the left anterior descending artery (LAD) and 43 age- and gender-matched participants with normal angiographically coronary arteries were included in the study. All patients with MB underwent coronary angiography for stable coronary disease with objective ischemia signs (exercise or myocardial perfusion scintigraphy tests). Patients with acute coronary syndrome, previous cardiac surgery, known coronary artery disease, concomitant dysfunction (>mild degree) of heart valves, cardiomyopathy, left ventricular systolic dysfunction (left ventricular ejection fraction [EF] <50%), atrial fibrillation, congenital heart defects, use of any cardiovascular drugs, history of renal or liver disease, malignancy, hematological disorders, and acute or chronic inflammatory disease were excluded from this study.
Angiographic Analysis
Diagnostic coronary angiography was performed using the standard Judkins technique in multiple projections. Myocardial bridging was defined as an intramyocardial systolic compression or milking of a segment of an epicardial coronary artery on angiography. 11
Laboratory Measurements
Venous blood samples were obtained from all participants in the morning between 08.30 and 10.00 hours, following a fasting period of 12 hours. Glucose, creatinine, and lipid profile were determined by standard methods (Cobas 8000-Hitachi, Roche, Mervue, Galway, Ireland). Blood samples were collected into tubes with K3 EDTA, and the MPV were measured by automatic blood counter (Hematology Analyzer; Coulter Bechman LH 780, Beckman Coulter Ireland Inc.). All analyses were performed in less than 1 hour after sampling to avoid swelling of platelets. The study was approved by the local ethics committee. Informed consents were obtained from the patients.
Statistical Analysis
Continuous variables are expressed as mean ± standard deviation (SD). The level of significance was .05. The Kolmogorov-Smirnov test was used to test the normality of all variables. To compare continuous variables, independent Student t test or the Mann-Whitney U test was used and to compare categorical variables chi-square test was used. Statistical analyses were performed using SPSS, version 15.0 for Windows.
Results
The study population consisted of 42 MB (52.7 ± 10.2, 76.2% male) and 43 healthy age- and sex-matched control participants (52.1 ± 10.4, 74.4% male). There were no significant differences between the groups with respect to age, gender, diabetes mellitus, hypertension, and smoking habits. The basal characteristics of the study population are listed in Table 1 .
Baseline Characteristics Between Myocardial Bridge and Control Participants.
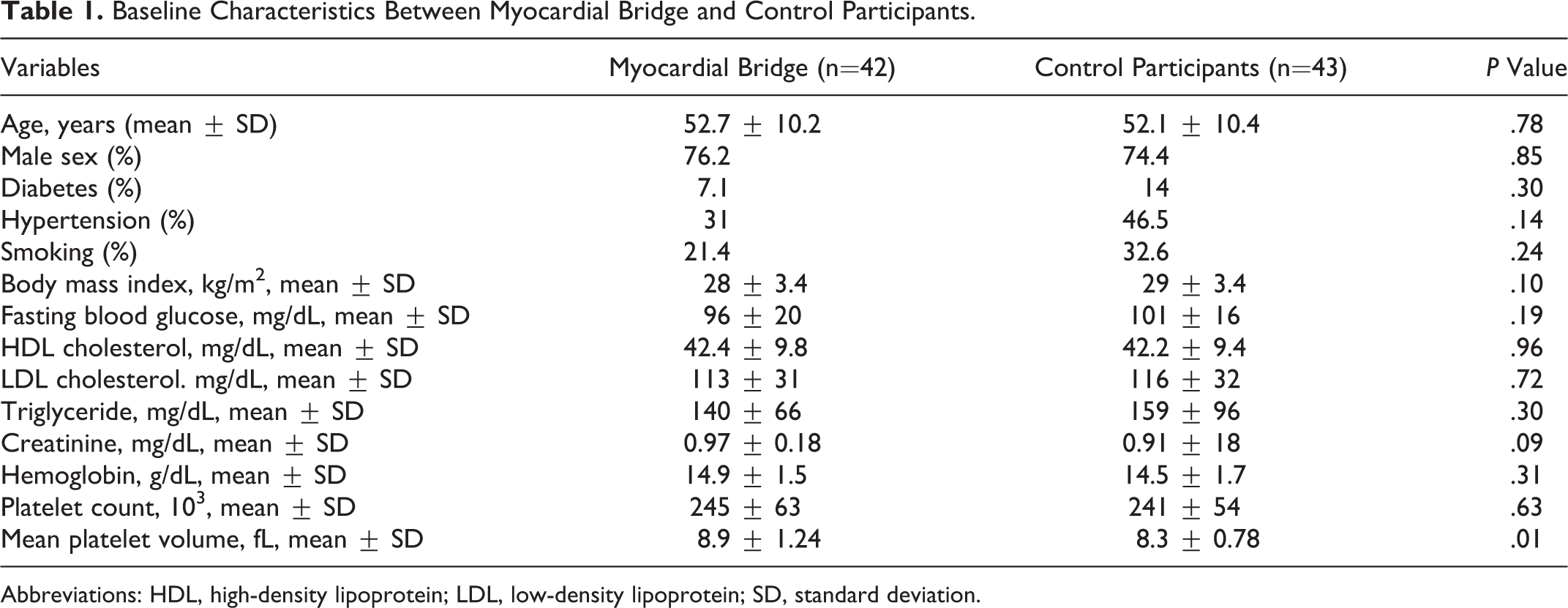
Abbreviations: HDL, high-density lipoprotein; LDL, low-density lipoprotein; SD, standard deviation.
Compared to the healthy control group, MPV value was significantly higher in patients with MB (8.9 ± 1.24 vs 8.3 ± 0.78; P = .01; Figure 1 ). Further, there were no significant differences between groups regarding the hemoglobin levels, platelet counts, blood lipid levels, fasting blood glucose, and creatinine levels.
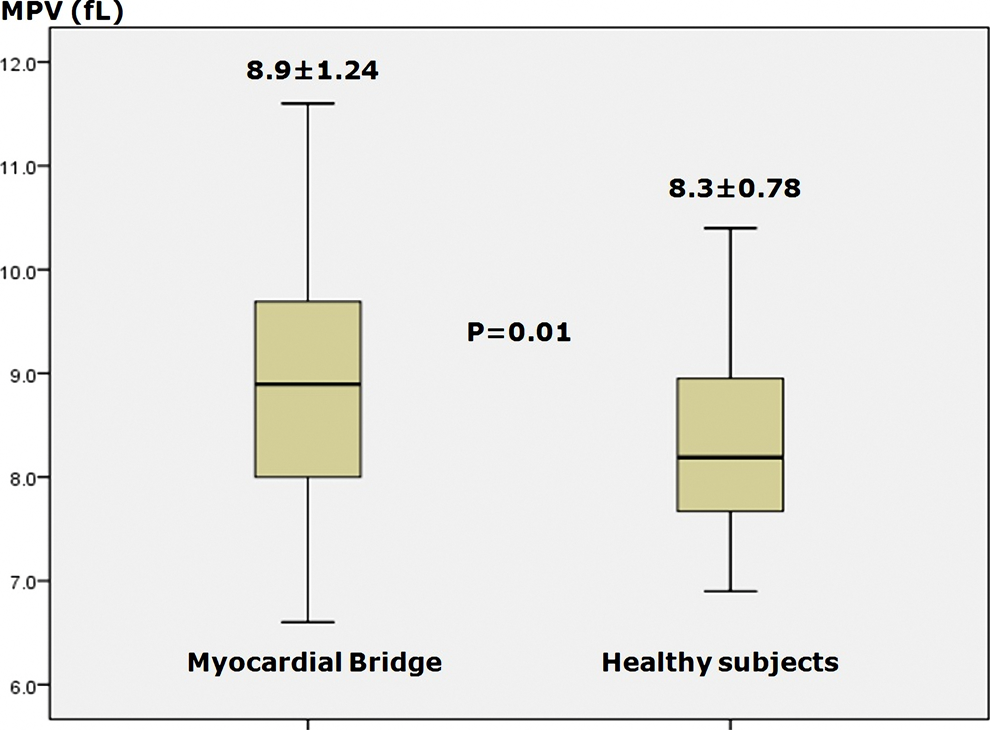
Box plot graphs of MPV values between MB and control groups.
Discussion
To the best of our knowledge, the present study is the first to investigate the MPV values in patients with coronary MB. We have found that patients with MB have significantly higher MPV values compared to control participants. Our results indicate that patients with MB tend to have increased platelet activation.
Myocardial bridging defined as a segment of a major epicardial coronary artery that courses intramurally through the myocardium beneath the muscle bridge. Myocardial bridging is generally confined to the mid-LAD, the main angiographic finding is systolic compression of the involved epicardial coronary artery. 12,13 Myocardial bridging is the most common congenital coronary anomaly, with an incidence of between 1.5% and 16% as assessed on coronary angiography and up to 80% as assessed in autopsy reports. 14 Although it is rare, MB may cause ischemia, acute coronary syndrome, coronary spasm, life-threatening arrhythmias, exercise-induced atrioventricular conduction block, sudden cardiac death. 4 –7 Angiographic studies and intravascular ultrasonographic studies have demonstrated that vessel compression during systole is followed by early diastolic diameter reduction and early diastolic flow acceleration especially during episodes of tachycardia. 15 It has been found that the pressure proximal to the MB was higher than the aortic pressure, and disturbance of blood flow and high wall stress proximal to the MB was the main contributor to the development of atherosclerosis in the proximal segment. 16 Systolic kinking of the blood vessel may cause trauma to the intima and damage to the endothelium. Additionally, endothelial dysfunction has been shown in the segment with MB. 17 These circumstances could produce platelet aggregation, thrombus formation, vasospasm, and result in an acute coronary syndrome. In previous studies, thrombus formation in MB-related arteries has been reported as the cause of a myocardial infarction or sudden cardiac death. 14,16,18 However, no study has investigated the relation between MB and platelet activation assessed by MPV.
Mean platelet volume, one of the platelet function indices that reflect the platelet production rate and stimulation, is assessed easily by a routine hematological analysis. Increase in MPV may occur as a result of the synthesis of prothrombotic and proinflammatory agents in platelets, degranulation of alpha-granules, and release of reactive platelets from stores. Mean platelet volume is a surrogate marker of platelet function associated with a variety of prothrombotic and proinflammatory disease states. 19 Several mechanisms might be responsible for increased MPV in our patients. One of them might be endothelial dysfunction and injury. It is shown that reduced endothelial production of prostacyclin and nitric oxide promotes increased activation of platelets. 20 It has been indicated that long-term compression and relaxation of such overbridged vessels produces impairment of endothelial-dependent vasorelaxation in the bridged segment. 17 Second, several studies have demonstrated that atherosclerotic lesions develop in the segment proximal to MB. 16 Intravascular ultrasonography (IVUS) and necropsy studies have reported that up to 88% of the patients with MB eventually develop atherosclerotic plaque in the segment proximal to MB. 21 Also MPV levels have been found to be increased as a consequence of the atherosclerotic process in our study. 20 Another mechanism contributing to increased platelet activity might be high shear stress in MB segment. Likewise several studies have shown that shear stress results in platelet activation. 22 So these insults might have a role in the increase of MPV in our patient group. Although most patients with MB have a good prognosis, increased platelet activity could contribute to increased atherosclerotic risk and atherosclerotic complications.
This study has some limitations including the small sample size of patients with MB. This was a cross-sectional study and we were not able to do any follow-up; therefore, we do not know whether increased MPV predicts atherothrombosis formation in our patient group. Since in our study we aimed to investigate MPV values in patients with MB, we did not extend our blood sampling to other plasma vascular markers and platelet activation markers. The IVUS was not performed routinely to assess the bridging segment.
As a conclusion, these findings indicated that MB is associated with elevated MPV values. The mechanisms may be due to endothelial dysfunction in the MB region, atherosclerotic lesions in the segment proximal to MB and high shear stress in MB segment. We speculated that patients with high MPV values might benefit from antiplatelet therapy. Further studies are needed to establish the clinical significance of increased MPV in patients with MB.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.