
Abstract
The widespread usage of blood count autoanalyzers has led to a major improvement in cellular hematology because of quick and accurate results found in most instances. However, spurious test results also can be observed like pseudothrombocytopenia (PTCP). In our study, we aimed to evaluate the clinical and laboratory factors associated with PTCP. Forty-six patients with PTCP and 69 healthy volunteers were enrolled in the study. Sex distribution was similar between the groups. Hospitalization, infection, the use of low-molecular-weight heparin and pregnancy increased the incidence of PTCP. Atherosclerosis and some drugs such as warfarin and calcium channel blockers were associated with PTCP, but the coincidence was not statistically significant. Antinuclear antibody positivity was higher in PTCP group (18.8% vs 7.2%; P=0.033) but anticardiolipin positivity rates were similar when compared to controls. Pseudothrombocytopenia was frequently misdiagnosed, which led to inappropiate treatments. Therefore, this situation should be kept in mind.
Introduction
EDTA-dependent pseudothrombocytopenia (PTCP) is the phenomenon of a false low platelet count due to EDTA-induced aggregation of platelets. This condition may be caused by many factors such as clotting of blood because of insufficient anticoagulation and platelet satellitism, but most of the cases are related to thrombocyte autoagglutination usually along with EDTA anticoagulation. Incidence of EDTA-dependent PTCP is approximately between 0.07% and 0.20% in general hospital practice, 1 which is increased in hospitalized patients, 2 about 0.1% to 2%. Despite this, the laboratory result is devoid of any clinical importance, misdiagnosis of PTCP as true thrombocytopenia leads to inessential diagnostic tests and unwarranted exposure to transfusion and related complications.
Antinuclear antibody (ANA) test is especially used to detect some autoantibodies against nucleus antigens. These antibodies are usually seen with systemic or organ-specific autoimmune diseases like systemic lupus erythematosus (SLE), Sjögren's syndrome, Raynaud phenomenon, scleroderma, Calcinosis cutis, Raynaud's phenomenon, Esophageal dysfunction, Sclerodactyly and Telangiectasia (CREST’s) syndrome, and dermatopolymyositis. False positivity with increasing age and cross-reactions in some autoimmune conditions is seen.
Antiphospolipid syndrome (APS) is characterized by arteriovenous thromboses, repetitive pregnancy losses, and positivity of some antibodies. Laboratory tests of this disease consist of lupus anticoagulant and antiphospolipid (aPL) antibodies. But this antibody is also not specific and can be determined with other diseases. Anticardiolipin (ACA) positivity is about 5% in healthy control groups and 35% in patients with SLE. 3
It has been observed that ACA level is associated with a degree of thrombocytopenia in patients with SLE and autoimmune thrombocytopenia.4,5 These data propose that these antibodies make cross-reactions with phospholipids and cause destruction of thrombocytes.
In the light of all these information, we can consider that antibodies may show false positivity even in healthy people. Also some studies have implied clinical situations and incidence of PTCP in these cases. We aimed to determine the relationship between PTCP and some clinical conditions like hospitalization and infection; some autoantibodies and routine laboratory tests performed in our polyclinics of internal medicine.
Materials and Methods
The study was conducted between January 2010 and August 2010 at Fatih University, Faculty of Medicine, Ankara, Turkey. Forty-six patients with the diagnosis of PTCP (50.4 ± 21 years) and sex-matched 69 healthy controls (47.4 ± 18 years) were enrolled in the study.
Participants whose platelet count was below 100 × 10 9 /L, measured by automatical complete blood count analyzers, had no primary hemostatic disease, at least 15 platelet clusters were observed in freshly prepared peripheral blood smears that were accepted as PTCP.
The EDTA and also citrate-coagulated blood samples were collected from patients diagnosed as PTCP. Patients and controls were evaluated by pregnancy, positivity of ANA and ACA antibodies, existence of cold agglutinins, malignancy, concomitant diseases, huge thrombocytes, satellitism of platelets, hyperlipidemia, and medications.
Informed consent was obtained from each patient, and our study protocol was according to the ethical guidelines of the Declaration of Helsinki as reflected in a prior approval of university’s human research committee. The local ethics committee approved the study.
Blood samples were collected from patients and control groups after overnight fasting. Routine tests were performed with blood sample coagulated with 5% EDTA. Patients who have platelet count lower than 100 × 10 9 /L and no bleeding tendency evaluated as EDTA dependent pseudothrombocytopenia.
Concurrently, citrate-coagulated venous blood samples were also studied. Peripheral smears of blood both taken from fingertip and EDTA-coagulated tubes were also evaluated for each participant.
Prothrombin time, activated platelet thromboplastin time, fibrinogen, and
Cold agglutination test was performed for each participant using the suitable method. 1/32 and more titers at 39.20F and significant titers not corrected at 98.60F were assessed as positive test. Antinuclear antibody test is studied with immune flourescence antibody (IFA) method using human epithelial cells (HEp-2) as a substrate. The test was evaluated as positive if nucleus showed different fluorescent staining that may be with several patterns. If nucleus did not show any specific staining, the ANA test was evaluated as negative. Anticardiolipin immunoglobulin M (IgM) and IgG (ACA-IgM and ACA-IgG) antibodies were studied with enzyme-linked immunosorbent assay method using Aeskulisa Cardiolipin GM kit (Aeskulisa Diagnostics GmbH, Wendelsheim, Germany). Normal plasma levels were accepted as 0 to 15 MPL/mL for ACA-IgM and 0 to 15 GPL/mL for ACA-IgG.
All analyses were performed using the statistical package of social programs (SPSS) for Windows, version 13.0 (SPSS Inc, Chicago). The demographic features of 2 groups were statistically compared with Pearson chi-square, Fisher exact chi-square tests, and Kruskal-Wallis variance analyses. If significant difference is detected with Kruskal-Wallis test, the groups causing this significance are assessed with Mann-Whitney U test. The correlation of variables was analyzed using Spearman correlation test. Data were expressed as mean value ± standard deviation. P <.05 was considered as statistically significant.
Results
A total of 49 consecutive patients diagnosed with PTCP were included in this study. Results were compared with 69 healthy volunteers. Fifty-threepercent of patients were women (n = 51) and 36.2% were men (n = 29). Sex distribution was similar between 2 groups. Mean age of patient group was 50.4 ± 21 and of control group was 47.4 ± 18 years. There was also no significant difference (P > .05). Ten patients (20%) with PTCP were pregnant and 3 of them were EDTA-PTCP. None of the pregnant women in the study had any disease and medication; all of them showed normal platelet counts after delivery.
Overall, 23.8% of patients had diabetes mellitus (DM), 32.5% were hypertensive, 26.3% had atherosclerotic heart disease, 5% history of cerebrovascular accident, and 10% had hypothyroidism. Thirty-eight of them was hospitalized (76.25%) and 58% of patients had coexisting disease. There was no statistically significant difference between control and patient groups about coexisting diseases. Table 1 shows comparison of 2 groups about medications, coexisting diseases, and demographic features.
Comparison of Demographic Features, Concurrent Diseases, and Medications of Control and PTCP Groups
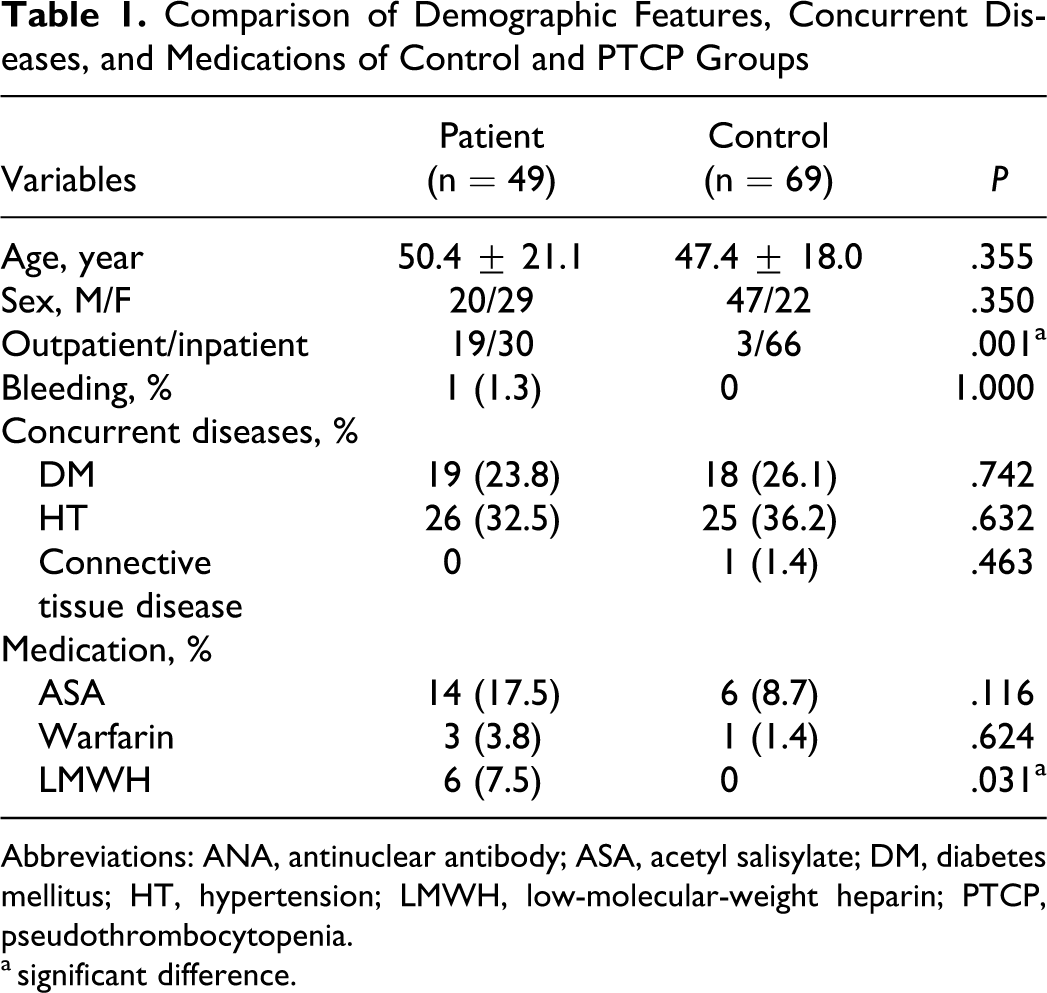
Abbreviations: ANA, antinuclear antibody; ASA, acetyl salisylate; DM, diabetes mellitus; HT, hypertension; LMWH, low-molecular-weight heparin; PTCP, pseudothrombocytopenia. a significant difference.
Twenty patients (51.3%) were using medications, consisting of mostly aminosalicylic acids (17.5%), β-blockers (16.3%), calcium channel blockers (8.8%), angiotensin-converting enzyme inhibitors (8.8%), angiotensin receptor blockers (7.5%), and low-molecular-weight heparin (LMWH, 7.5%). The LMWH usage was significantly higher at PTCP group. Incidence of active infection and ratio of hospital stay were higher in LMWH-taking group (P = .011, P = .010).
Also, complete blood count and laboratory parameters were compared between groups and high white blood cell and mean platelet volume (MPV) values at PTCP group (P = .003 and P = .006). Laboratory parameters are compared in Table 2 .
Comparison of Some Laboratory Parameters Between Patient and Control Groups
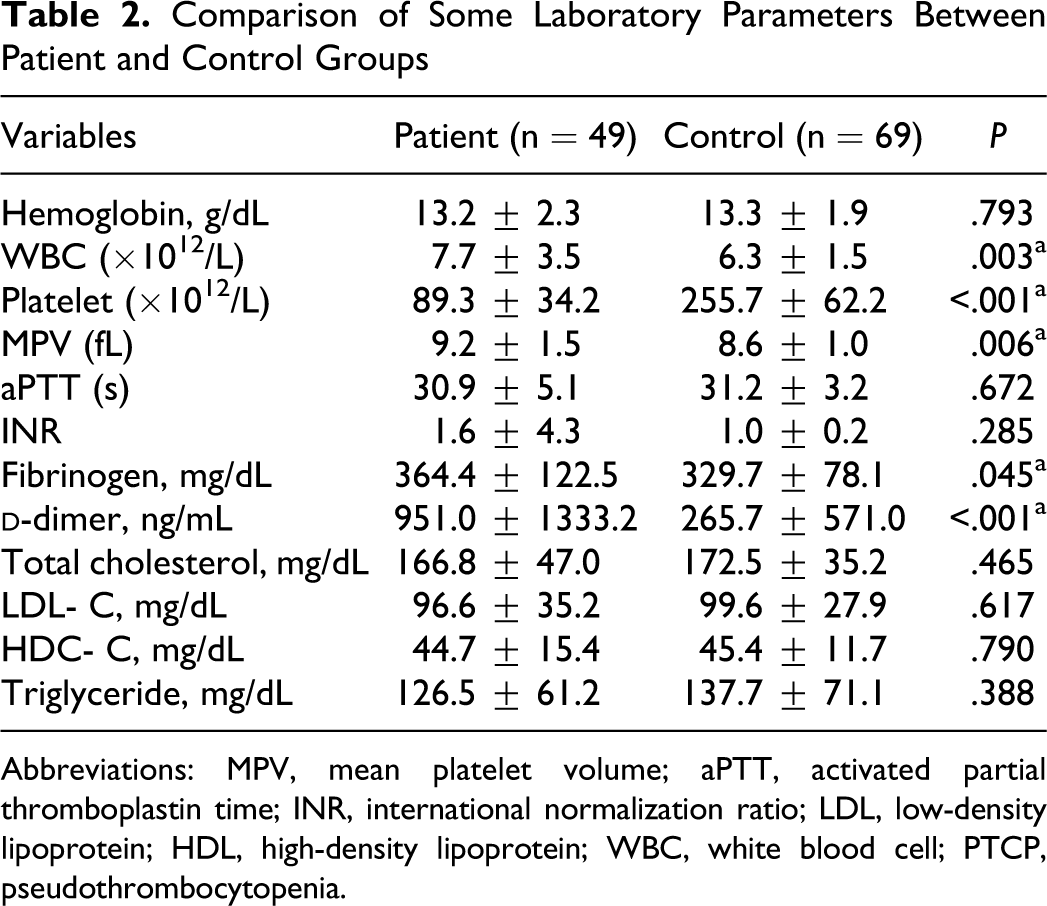
Abbreviations: MPV, mean platelet volume; aPTT, activated partial thromboplastin time; INR, international normalization ratio; LDL, low-density lipoprotein; HDL, high-density lipoprotein; WBC, white blood cell; PTCP, pseudothrombocytopenia.
Fifteen patients and 5 controls had ANA positivity (P = .033). Thirty patients were ACA positive, whereas none of the control group had it. This difference was not statistically significant. Figure 1 compares autoantibody positivity between the 2 groups.
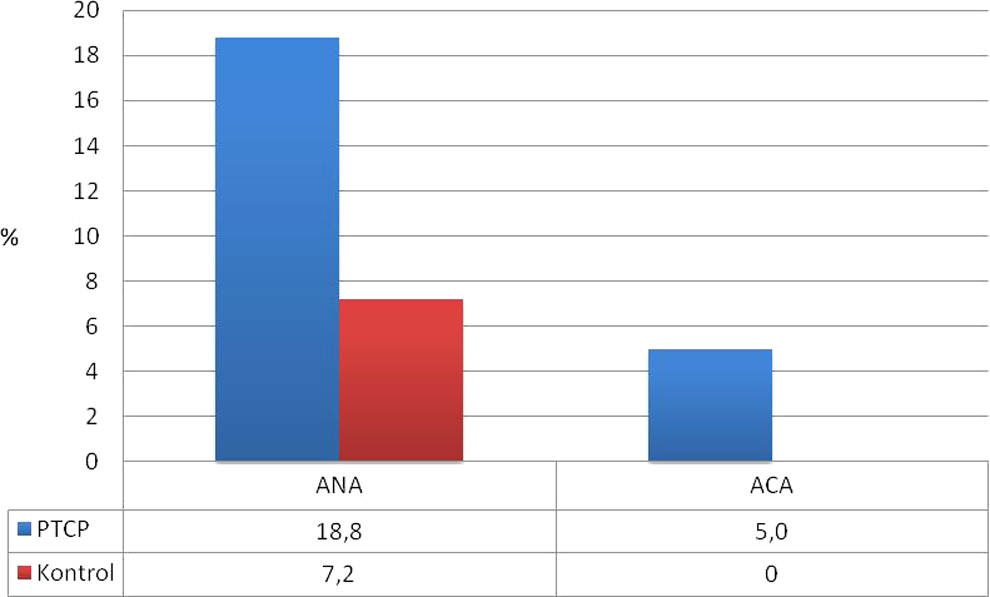
Comparison of antinuclear antibody and anticardiolipin antibody levels between PTCP and control groups.
When EDTA- and citrate-coagulated samples were compared for blood counts, platelet count is observed as significantly corrected, but citrated tubes showed apparently lower hemoglobin and hematocrit values (Table 3 ). Thirty-seven patients showed more than 50% increase after using citrate as an anticoagulant. Platelet count increases to 130000 after using citrate for anticoagulation, as observed in 24 participants (30%). Overall, 31.2% of patients showed unaltered or decreased platelet counts.
Comparison of Complete Blood Count Parameters Between EDTA-Coagulated and Citrate-Coagulated PTCP Groups
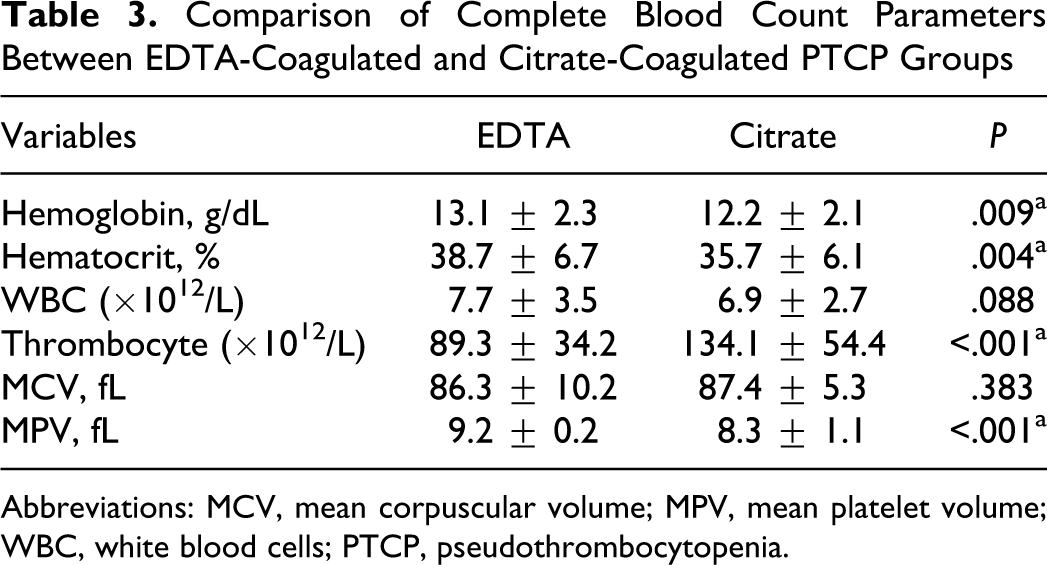
Abbreviations: MCV, mean corpuscular volume; MPV, mean platelet volume; WBC, white blood cells; PTCP, pseudothrombocytopenia.
Hospitalization is observed as significant risk factor for PTCP (odds ratio = 7.085). Consequently, existence of infection, ANA positivity, pregnancy, LMWH usage, and hospitalization were observed as significant risk factors with varying degree for PTCP. Odds ratios of parameters were also calculated (Table 4 ).
Odds Ratio of Some Risk Factors for Pseudothrom bocytopenia
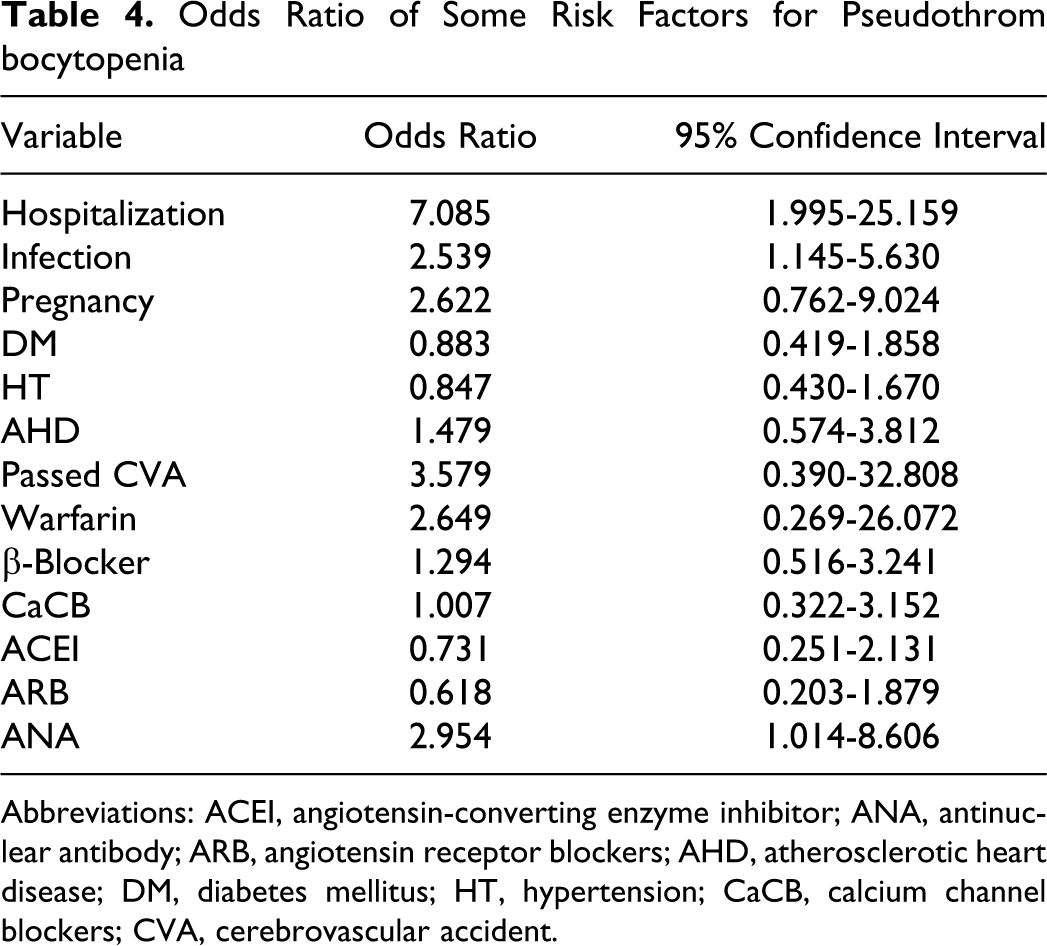
Abbreviations: ACEI, angiotensin-converting enzyme inhibitor; ANA, antinuclear antibody; ARB, angiotensin receptor blockers; AHD, atherosclerotic heart disease; DM, diabetes mellitus; HT, hypertension; CaCB, calcium channel blockers; CVA, cerebrovascular accident.
Discussion
Pseudothrombocytopenia is a term used for the condition wherein the autoanalyzers measure the platelet count incorrectly lesser than its true value because of platelet clustering. Usually this clustering is caused by antiplatelet antibodies in blood. 6 Incidence of platelet clustering was estimated at between 0.1% and 2% in hospitalized patients 7 ; in the same patient population, the incidence of EDTA-PTCP has been increased up to 1.9% when compared with all patients (0.09%, 8). In our study, we also observed that most of our patients with PTCP were inpatients.
Diabetic patients are more likely to have coronary atherosclerotic diseases. Also there are some clues indicating that DM leads to increased thrombocyte activity and count of young platelets in circulation. Also large thrombocytes with much more thromboxane-producing capacity and elevated synthesis of Gp1b and Gp2b/3a at megakaryocytes are expressed in diabetic patients in some reports. 8 Along with all these data, it is expected that increased tendency to PTCP is expected in diabetic patients because of these procoagulant factors; but in our study, no significant difference is detected about the frequency of PTCP between diabetic and nondiabetic patients. According to this finding, it may be considered that immunologic factors are much more important at PTCP etiology.
In our study, LMWH usage is observed to be significantly higher in PTCP group when compared with controls. Heparin shows its effect on antithrombin 3 (AT3). Antithrombin 3 is a neutral inhibitor that binds to thrombin with other coagulants and neutralises them. Heparin increases the effectiveness of AT3. Heparin is available in 2 forms according to their molecular weight: unfractionated and low molecular weight. The LMWH is obtained from unfractionated heparin by chemical hydrolysis and shows different features. The LMWH has more factor XA selectivity and lesser tendency to thrombin binding. This molecule also has lesser effect on thrombocyte when compared with unfractionated form, rarely causing heparin-induced thrombocytopenia. Although LMWH has lesser effect on platelets, clustering must be decreased in the groups using LMWH when compared with patients not using any heparins. In our study, higher incidence of PTCP in LMWH-using group may be associated with higher hospitalization and infection ratio in this group. In our study, higher incidence of PTCP in LMWH-using group may be associated with higher hospitalization and infection ratio in this group.
Mean platelet values of EDTA-coagulated samples were significantly higher compared to citrated samples in our study. The MPV usually increases when peripheral destruction of platelets occurs but decreases when any disease disrupts the platelet production. For example, MPV is usually above 11 fL in idiopathic thrombocytopenic purpura (ITP), but this value is below 6.4 in aplastic anemia and leukemia. 9 Also it is known that when EDTA is used as an anticoagulant, thrombocytes at peripheral blood expands, so the values of MPV and the width of platelet distribution are higher in EDTA-coagulated blood when compared with citrate-coagulated one. Our findings were similar to the previous reports.
About 8% thrombocytopenia is seen during pregnancy. 10 The most common cause is gestational thrombocytopenia, comprising approximately 75% of cases, the other common cause is hypertensive diseases (21%) like eclampsia, preeclampsia, and a component of hemolysis, elevatde liver enzymes, low platelets (HELLP) syndrome. The other rare but important cause of thrombocytopenia during pregnancy is immune-associated thrombocytopenia like ITP and neonatal alloimmune thrombocytopenia. 11 Other reasons are rheumatologic diseases like SLE, disseminated intravascular coagulation, antiphospholipid syndrome, and drugs. There are some case reports and case series about PTCP during pregnancy. 12 Even neonatal PTCP related to transplasental passage of antibodies is also reported. 13 In our study, the frequency of PTCP was higher in patient group when compared to controls. Pregnancy can cause different immunologic mechanisms and PTCP pathogenesis may differ in pregnant women. More studies are needed with regard to this subject.
Antiphospolipid antibodies are produced against negatively charged phospholipids in cell membranes in the presence of plasma apolipoprotein H, which is a cofactor binding to the platelets.14,15 Because phospholipids on platelet membranes play a role in thrombotic processes, aPL antibodies may cause platelet aggregations.4,16 Antiphospolipid antibodies are proven to accompany chronic autoimmune ITP 17 and also a relationship is proven between thrombocytopenia in SLE and aPL antibodies.18,19 This sign suggests that aPL antibodies may cause thrombocyte destruction by direct mechanisms. In our study, we did not find any relationship between PTCP and aPL antibodies.
In our study, significant ANA positivity was observed in patients with pseudothrombocytopenia. Anticardiolipin antibodies also showed increased positivity in the patient group, but it was not statistically significant. In a report, they produced some autoantibodies against negatively charged phospholipids and thrombocyte surface proteins like glycoporotein 2b-3a by the way of using tonsillary lymphocytes. 5 These data suggest that patients with autoimmune diseases and even healthy people can produce antiplatelet and antiphospholipid antibodies, and these antibodies may show cross-reactions. So, we considered that we may find antiplatelet antibodies in our ANA and ACA measurements. In a study, they confirmed that EDTA-dependent antibody coincided 81.8% patients together with 63.6% ACA postivity in the same patient group. This concordance was related to antibody similarity between the tests. 20 So, there may be a cross-reaction between ACA antibody and thrombocytes.19,21 In our study, there was no significant relationship between PTCP and ACA antibodies.
Some errant thrombocytic measurements are possible at the time of infection.22,23 Abnormal platelet histograms can be observed because of bacteriemia in peripheral blood smear and contamination. 24 Fungi and some fungal particles may evaluated as platelet in automatized blood counters. 25 It is also proven that platelet count wrongly measured higher in patients with thrombocytopenia having candida infection. 26 In our study, 36.3% of patients with PTCP had infection.
Conclusion
There is no enough data to evaluate EDTA-PTCP as a clinical condition for possible autoimmune and neoplastic diseases. But we consider that when thrombocytopenia is observed, it is beneficial to evaluate the risky patients for autoimmune diseases.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.