
Abstract
Platelet dysfunction contributes to the increased risk of thromboischemic complications after percutaneous coronary intervention (PCI), particularly in type 2 diabetes. Little is known about the effects of glycemic control on platelet reactivity. We assessed adenosine diphosphate-induced platelet aggregation and flow cytometric expression of P-selectin in 90 patients (56 diabetic and 34 nondiabetic patients) undergoing coronary stent implantation after administration of clopidogrel as a potential predictor of poststent complications and its relation to glycemic control. Posttreatment platelet reactivity was significantly elevated in diabetic compared with nondiabetic participants and was associated with smoking, hypercholesterolemia, overweight, and cardiovascular ischemic events. A linear relationship was found between hemoglobin A1c in diabetic patients and platelet reactivity. Both methods (standard aggregometry and P-selectin expression) used for assessment of platelet function were positively correlated. Low responsiveness to clopidogrel detected by posttreatment platelet reactivity is a risk factor for ischemic events after PCI in diabetic patients.
Introduction
Platelet aggregation and activation mediated by various agonists play fundamental roles in the development of ischemia in patients with coronary artery diseases (CAD) 1 and in thromboischemic complications after percutaneous coronary intervention (PCI). 2 Activated platelets mediate vessel wall inflammation, and generation of thrombin and platelet–platelet aggregates mechanically obstruct the vessel lumen. 3
Diabetes is commonly associated with accelerated atherosclerosis.4,5 Patients with type 2 diabetes have a 2- to 4-fold increase in the risk of CAD, and diabetic patients without prior myocardial infarction have the same risk for a subsequent acute coronary event as nondiabetic patients with a previous myocardial infarction. 6 Platelet dysfunction, among other mechanisms, contributes to the increased risk of atherothrombotic complications in the diabetic population.7,8
Exogenous added adenosine diphosphate (ADP) and ADP released from platelet dense bodies following activation bind 2 types of platelet G-protein coupled purinergic receptors (P2Y1 and P2Y12).9,10 Signaling events downstream of the P2Y12 receptor mediate thromboxane A2 production, α-granule release, and subsequent expression of P-selectin on activated platelets. 11 The P2Y12 receptor stimulation by ADP is inhibited by clopidogrel (Plavix or Iscover), a thienopyridine prodrug, which has to be metabolized in the liver to acquire its antiplatelet aggregation properties. 12 Clopidogrel with aspirin is the regimen of choice to prevent stent thrombosis in patients undergoing PCI and to reduce major adverse cardiovascular events in patients with non-ST segment elevation acute coronary syndrome (NSTEACS).13–15
Nevertheless, numerous studies have reported interindividual variability in platelet response to clopidogrel and aspirin, and identified patients who did not achieve platelet inhibition as “low responders” or “resistants.”16–20 Stent thrombosis has been shown to occur in patients taking clopidogrel and aspirin.21,22 However, the definite demonstration of the association between low in vitro responsiveness to clopidogrel and thrombotic events is still lacking.23–26
Because the failure of antiplatelet therapy can have severe consequences, there is a need for a reliable assay to quantify the effectiveness of clopidogrel treatment. 27 Most clinical studies on clopidogrel rely on standard platelet aggregometry to measure the inhibition of ADP-induced aggregation.17,28 In addition to aggregometry, flow cytometric determination of surface expression of platelet proteins, in particular P-selectin (CD62P), is commonly used to monitor platelet activation. 27
There have been few reports on platelet reactivity testing in diabetic patients and little is known about the effects of glycemic control on platelet reactivity.29–31 Therefore, to find a consensual method that on one hand is practicable in clinical routine and on the other hand helps to identify diabetic patients at increased risk of thromboischemic complications, this study aimed to assess platelet function profile in patients with type 2 diabetes mellitus on clopidogrel therapy undergoing elective coronary stent implantation as a potential predictor of poststent complications and its relation to glycemic control, using both standard platelet aggregation testing and flow cytometric detection of P-selectin (CD62P).
Materials and Methods
Materials
This prospective study was carried out on 90 cardiac patients attending the cardiology clinic, National Heart institute, Cairo, Egypt (56 type 2 diabetic patients and 34 nondiabetic participants). The study protocol was approved by the local ethical committee of Ain Shams University, and an informed consent was obtained from each participant before enrollment.
The mean age of the whole patient population was 56.2 ± 6.9 years (range, 45-71 years). They were 52 males and 38 females, with a male-to-female ratio of 1.4:1. Patients enrolled in this study were scheduled for elective PCI. Patients were excluded if they had history of bleeding diathesis or gastrointestinal bleeding, a clinically significant illness, within 4 weeks prior to the study, acute myocardial infarction within 48 hours, elevated cardiac markers, cerebrovascular event within 3 months, chronic vessel occlusion or angiographically visible thrombus, a medical or surgical condition that may impair drug absorption or metabolism, taken anticoagulants or antiplatelet treatment (other than aspirin) within 2 weeks prior to PCI, a known allergy or intolerance to clopidogrel, a platelet count <100 × 109/L, abnormal kidney or liver function tests, and a history of major surgery or trauma within the preceding 3 months.
A loading dose of 600 mg clopidogrel (Biocure Pharm, Egypt) was given to all patients prior to PCI followed by a daily dose of 75 mg for at least 3 months. All patients had undergone successful coronary angioplasty with implantation of bare-metal stents (BMS). Patients who had complications during the procedure that may induce a bias in the trial were excluded. Routine medical treatment were administrated including nitrates, β-blockers, aspirin 162 mg/d, lipid-lowering drugs, and various types of antihypertensive drugs mainly angiotensin-converting enzyme (ACE) inhibitors for hypertensive patients. All diabetic patients were on oral hypoglycemic drugs and did not receive insulin therapy.
All the study participants were subjected to (i) full medical history and thorough clinical examination including measurement of blood pressure and body mass index; (ii) laboratory investigations including complete blood count (CBC) using Coulter LH 750 analyzer (Beckman Coulter, Inc., Fullerton, CA), liver and kidney function tests as well as assessment of serum glucose and serum cholesterol levels using Synchron CX-7 (Beckman, Switzerland), and estimation of hemoglobin A1c (HbA1c) for diabetic patients using D-10 (BioRad, France) in human whole blood through ion-exchange high-performance liquid chromatography. Platelet reactivity to ADP was measured using platelet-rich plasma (PRP) aggregation quantified by optical aggregometry and flow cytometric detection of P-selectin (CD62P) according to previous reports.17,21,29
Definitions and follow-up strategy
Patients with type 2 diabetes mellitus were defined according to the criteria of American Diabetes Association. 32 All the studied patients had scheduled clinical follow-up at 1, 3, and 6 months to determine the occurrence of adverse events and detect any poststent complications. The clinical end point included all the following cardiovascular events: the occurrence of death secondary to cardiovascular causes, recurrent acute coronary syndrome (ACS), and acute, subacute, and late stent thromboses. Acute coronary syndrome was defined by the presence of symptoms compatible with recurrent ischemia requiring rehospitalization and coronary angiography.21,33 Acute stent thrombosis was defined as stent thrombosis that occurred during the 24 hours after stent implantation. Subacute stent thrombosis occurred after discharge to 30 days follow-up, whereas late-stent thrombosis occurred between 30 days and 6 months of follow-up. 34 Response to clopidogrel was assessed by posttreatment platelet reactivity defined as the percentage of platelet aggregation induced by 5 μmol/L ADP or percentage of platelet activation prior to PCI in patients already on clopidogrel for at least 6 hours when maximum inhibition was expected.21,24,30,35
Methods
Sampling
Peripheral blood samples were collected from patients before undergoing PCI at least 6 hours after first administration of 600 mg of clopidogrel in vacutainer tubes containing potassium ethylene diamine tetraacetic acid in a final concentration of 1.5 mg/mL for CBC and in vacutainer tubes containing 0.2 mL 3.8% trisodium citrate in a ratio of 9 volumes of blood to 1 volume of citrate properly mixed for assessment of platelet reactivity. For chemical analysis, clotted samples were obtained and serum was separated.
ADP-induced platelet aggregation using light transmittance aggregometry
Platelet-rich plasma was obtained as a supernatant by centrifugation of citrated whole blood for 10 minutes at 120g. A second centrifugation was done at 850g for 10 minutes to obtain platelet-poor plasma (PPP). Platelet count was performed on PRP using Coulter LH 750 analyzer (Beckman Coulter, Inc., Fullerton, CA) and counts were adjusted between 200 × 109/L and 400 × 109/L by dilution with autologous PPP. Platelet aggregation was assayed by the turbidimetric method in a 2-channel aggregometer (Chrono-Log 450 Model; Chrono-Log, Havertown, Pennsylvania), according to other reports.18,36 Light transmission was adjusted to 0% with PRP and to 100% for PPP for each measurement. Platelet aggregation was assessed within 2 hours from blood sampling. Aggregation was assessed in siliconized tubes at 37°C in constant stirring conditions and was induced by 5 μmol/L ADP (Diamed, Switzerland), as described elsewhere.17,37,38 Aggregation was expressed as the maximal percentage change in light transmittance from baseline with PPP from the same patient as a reference. Hematocrit and platelet count were assessed to ensure that the degree of platelet reactivity was not influenced by cell counts. Control samples from healthy volunteers who had not taken medications or antiplatelet drugs for the preceding 2 weeks were included in each run with patients’ samples to determine the median normal reference aggregation value.
Flow cytometric detection of surface platelet receptors
Evaluation of surface expression of platelet receptors by standard 3-color flow cytometry was performed in citrated whole blood based on Gawaz et al 39 with the use of the following monoclonal antibodies: anti-CD61 PE (anti-GP IIb/IIIa labeled with phycoerythrine) which is specific for resting and activated platelets, anti-P-selectin labeled with fluorescein isothiocyanate (anti-CD62P FITC) which is a marker of platelet activation, and FITC and PE isotypic controls supplied by Beckman Coulter. Briefly, 10 μL of citrated blood were diluted with 490 μL phosphate-buffered saline (PBS); Sigma Chemicals, St Louis, Missouri. A volume of 35 μL of the mixture was added to 5 μL of anti-CD61 PE, 5 μL of anti-CD62P FITC, and 5 μL of ADP (5 μmol/L) or PBS (for resting samples). A resting sample was performed to ensure the absence of in vitro platelet activation and determine the spontaneous level of CD62P expression. For each activation point, a mouse isotype control was carried out in parallel. Samples were protected from light and incubated at room temperature for 20 minutes then fixed with 300 μL of 1% buffered paraformaldehyde for a maximum of 1 hour, until data acquisition in EPICS-XL PROFILE II Coulter flow cytometer (Beckman Coulter). Platelets were gated via their forward and side scatter properties and were identified based on their expression of CD61. Data were expressed as the percentage of positive events (ie, the percentage of platelets positive for coexpression of CD61 and CD62P) as described elsewhere.27,29,40,41
Statistical analysis
Analysis of data was done by IBM computer using Statistical Program for Social Science version 15 (SPSS Inc, Chicago, Illinois). Quantitative variables were described in the form of mean, standard deviation (SD), median, and range; and qualitative variables were described as number and percentage. Student t, Mann-Whitney, Kruskal-Wallis, χ2, and Fisher exact tests were used for intergroup comparisons. Spearman correlation coefficients were used to study the correlation between posttreatment platelet reactivity and HbA1c. The predictive capability of ADP-induced platelet aggregation and P-selectin expression was assessed using the receiver–operating characteristic (ROC) curve. The area under the curve is a measure of the overall discriminatory power of the platelets. P values <.05 and <.01 were considered significant and highly significant, respectively, in all analyses.
Results
Upon comparison between demographic data of diabetic and nondiabetic patients (Table 1 ), hypertension and hypercholesterolemia were more evident among patients with type 2 diabetes than nondiabetic participants (P = .021 and P = .032, respectively). Notably, the percentage of posttreatment ADP-induced platelet aggregation and flow cytometric expression of CD62P was significantly elevated in cardiac patients with type 2 diabetes compared with nondiabetic patients (P < .001). The overall incidence of 6 months of poststent complications was 15.6% (14 of 90 patients). The ischemic events were higher among diabetic population (21.4%) compared with nondiabetic participants (5.9%). In fact, the majority of patients with poststent complications (85.7%) had type 2 diabetes compared with 14.3% of nondiabetic patients (P = .49).
Clinical and Laboratory Characteristics of Cardiac Patients With and Without Diabetes Mellitus

Abbreviations: ADP, adenosine diphosphate.
As shown in Table 2 , the percentage of posttreatment platelet aggregation with respect to 5 μmol/L ADP was higher in females, obese patients, patients with hypercholesterolemia, and those with poststent complications (P < .05). Similar associations were observed as regard to P-selectin expression except for overweight (P < .05). In addition, the percentage of P-selectin expression was elevated among smokers (P = .02). Patients with previous myocardial infarction and a left ventricular ejection fraction <40 displayed increased posttreatment platelet reactivity than their counterparts (median platelet activation 27% vs 17% and 26% vs 17%, respectively), yet, the difference did not reach statistical significance.
Association Between Posttreatment Platelet Reactivity and Patients Characteristics
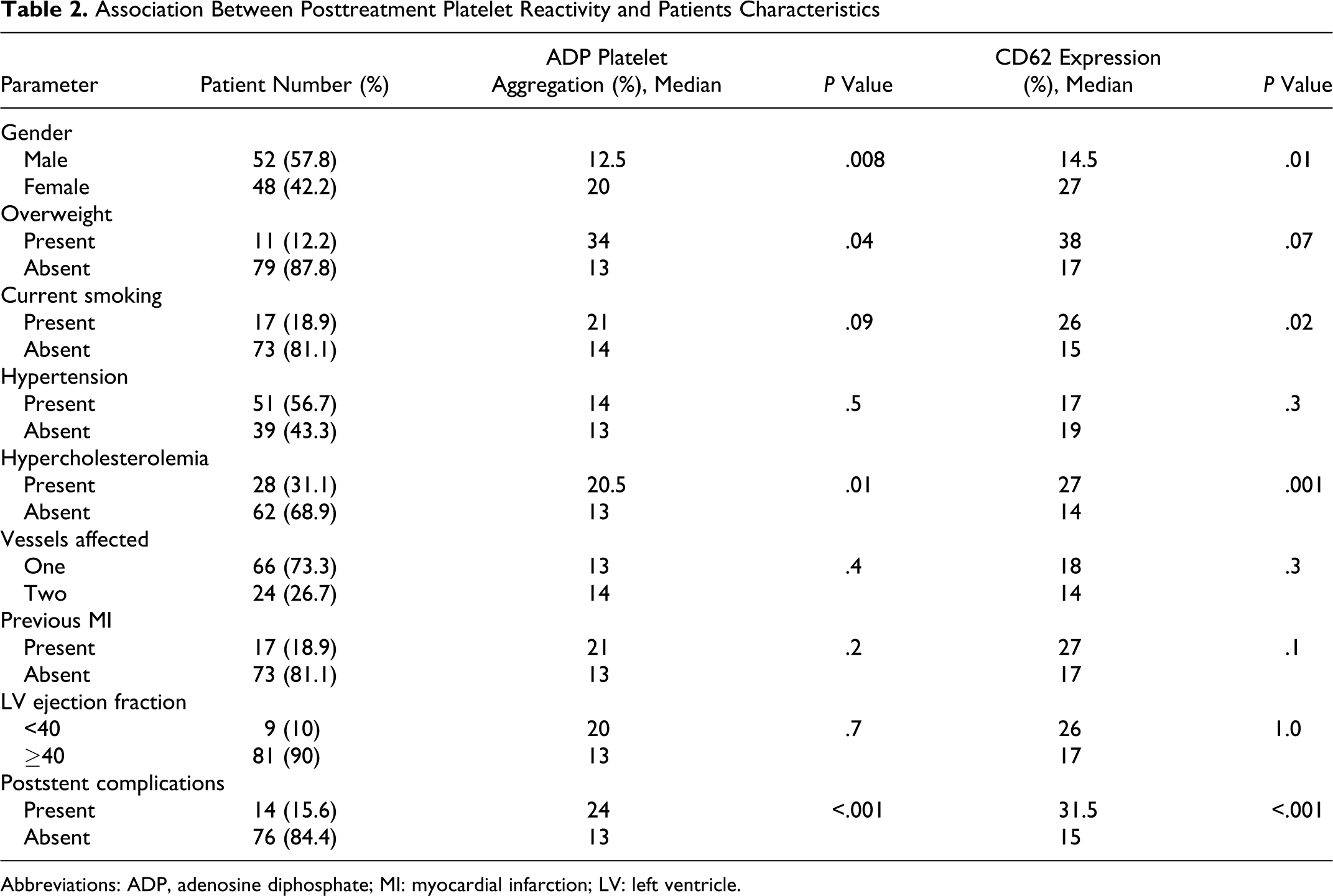
Abbreviations: ADP, adenosine diphosphate; MI: myocardial infarction; LV: left ventricle.
Analysis of predictors of posttreatment platelet reactivity in the studied diabetic patients (Table 3) showed that the percentage of ADP-induced platelet aggregation was increased in obese diabetic participants compared with those with average weight (P = .007), whereas CD62P expression percentage was markedly elevated in obese diabetic patients, smokers, and those with hypercholesterolemia (P < .05). A significant association was found between both of ADP-induced platelet aggregation and P-selectin expression levels and poststent complications (P = .007 and P = .003, respectively).
Predictors of Posttreatment Platelet Reactivity in Diabetic Patients

Abbreviation: ADP, adenosine diphosphate.
Correlation studies revealed a linear relationship between HbA1c as an index for glycemic control in diabetic patients and the percentage of both ADP-induced platelet aggregation and CD62P expression (r = .289 and r = .292, respectively; P = .03). Both methods used for evaluation of platelet function profiles; standard platelet aggregometry in response to 5 μmol/L ADP and CD62P expression by flow cytometry were positively correlated among all participants as well as in diabetic and nondiabetic patients, separately (r = .927, r = .917, and r = .833, respectively; P < .001; data not shown). Representative example of flow cytometric detection of CD62P expression is shown in Figure 1.

Flow cytometric detection of P-selectin in a diabetic patient (A) and nondiabetic patient (B).
To determine the best cutoff value of posttreatment platelet reactivity to predict the clinical end point, ROC curve analysis (Figure 2) revealed that both conventional ADP-induced platelet aggregation and P-selectin expression were able to distinguish between patients with and without poststent complications. The cutoff for standard aggregometry is 12.5%; area under the curve 0.793, 95% confidence interval 0.674 to 0.913, while the cutoff for P-selectin is 18.5%; area under the curve 0.831, 95% confidence interval 0.736 to 0.926 (P < .001). All complicated cases were above these values (P < .001).

Receiver–operating characteristic (ROC) curve analysis of post-clopidogrel platelet reactivity in relation to ischemic events.
Discussion
Several clinical studies revealed low or nonresponsiveness to clopidogrel that may be the result of inadequate generation of the active drug metabolite required to inhibit the P2Y12 receptors.17,28,42 In some studies, response to clopidogrel was defined as the difference between baseline and posttreatment maximal intensity of platelet aggregation.43,44 This definition is not consensual and the cutoff value16,17,27 to identify low responders varied from <10% to <40%. This approach is also not suitable for daily clinical practice as the majority of patients with ACS are urgently treated and many others are already on chronic clopidogrel or aspirin therapy at the admission to the hospital. 33 High posttreatment platelet reactivity was proposed as a better estimate of thrombotic risk rather than clopidogrel responsiveness.33,45,46 Therefore, we choose to identify clopidogrel effect with ADP-induced platelet aggregation and activation on 1 single-blood sample at the PCI time.
In the present analysis, patients with type 2 diabetes had higher incidence of hypertension, hypercholesterolemia, and poststent complications. The elevated posttreatment platelet reactivity observed in diabetic patients denoted decreased response to clopidogrel. This could provide a pathophysiologic mechanism explaining increased cardiovascular risk in patients with diabetes. In agreement with these findings, it was reported that diabetes is a “prothrombotic state” characterized by atherosclerosis, inflammation, and high platelet reactivity.47,48 Platelet function profiles were first studied in diabetic patients on combined aspirin and clopidogrel treatment by Angiolillo et al 29 who found increased platelet aggregation and activation after a 300-mg clopidogrel loading dose and a high proportion of nonresponders to the standard clopidogrel loading dose in the diabetic population. Recently, more evidence has shown that diabetic patients may be predisposed to inadequate platelet responses to clopidogrel.30,31,49
In the present study, the incidence of 6 months of bare-metal poststent complications in all patients was 15.6% (14 of 90 patients), being 21.4% among diabetic patients. These results were in line with Zurakowski et al 50 who reported the occurrence of restenosis at 6-month follow-up in 10 (13.7%) of 73 patients, and Cuisset et al 33 who found cerebrovascular ischemic events in 12 (11%) of 106 patients within only 1-month follow-up after PCI. Moreover, Gurbel et al 21 found that 44 (20%) of 191 patients had cardiovascular ischemic events within 6-month follow-up. Type 2 diabetes has been considered an equivalent to CAD. Several mechanisms account for such increased atherothrombotic risk in diabetic populations including hyperglycemia, insulin resistance, and proinflammatory and prothrombotic status. 51 The prothrombotic status is related to endothelial dysfunction, impaired fibrinolysis, increased coagulation factors, and altered platelet function, which decrease response to antiplatelet agents.8,29
At present, the mechanisms underlying clopidogrel resistance remain broadly unexplored and are likely multifactorial.31,52,53 Possible explanations that may be involved in the reduced sensitivity of diabetic platelets to dual antiplatelet therapy observed in our study include increased platelet turnover, cytosolic levels of calcium, oxidative stress resulting in aspirin-insensitive thromboxane biosynthesis, altered structure of platelet membrane due to impaired lipid metabolism, genetic polymorphisms of the ADP receptor, dysfunctional cytochrome P450 metabolism, differences in the rate of intestinal absorption of clopidogrel, and enhanced protein glycation reducing interaction with drug target.29,41,53,54 The latter mechanism may explain why poor metabolic control may play a role in reduced platelet sensitivity to antiplatelet drugs. 55 This is in line with the linear relationship demonstrated in the present study between HbA1c and posttreatment platelet reactivity.
In some studies, no correlation was found between HbA1c levels and platelet aggregation, suggesting that glycemic control does not play an important role in clopidogrel resistance.29,52 This was attributed to the limited variability of HbA1c levels in those patients and because all the studied patients in these reports had CAD; therefore, metabolic control was reinforced. Recently, Singla et al 30 showed that diabetic patients with HbA1c ≥7.0 g/dL had significantly higher ADP-induced platelet aggregation than those with HbA1c <7.0 g/dL and found an important correlation between glycemic control and platelet reactivity. This suggests that poorly controlled diabetic patients may require alternative antiplatelet strategies. With the aforementioned observation taken into account, our study further elucidates the link between glycemic control and platelet reactivity.
In the current work, higher posttreatment platelet reactivity was associated with obesity, smoking, hypercholesterolemia, and cardiovascular ischemic events in all patients and diabetic individuals, as well. Our results were in agreement with other reports.17,21,24,56 In diabetic patients, no relationship was reported between ADP aggregation and gender, duration of the disease, body mass index, hypertension, and lipid profile. 52 Therefore, larger scale clinical trials are warranted to evaluate these prognostic measures and their implementation for therapeutic decisions. Despite variables in a single patient that may affect the responsiveness to clopidogrel over time, Buonamici et al 23 showed that a single assessment of the in vitro responsiveness to clopidogrel is a strong marker of thrombotic risk, and patients with high posttreatment platelet aggregation had nearly 4-fold increase in definite or probable stent thrombosis as compared with clopidogrel responders.
The strong predictive value for poststent complications provided by a single assessment of platelet function, as presented in the current work, has important clinical implications. It strongly suggests that antiplatelet therapy directed against P2Y12 and cyclooxygenase 1 in the current dosages is not sufficient to overcome thrombosis in selected patients as reported by Gurbel et al. 21 A strategy of higher maintenance dose or switch to different thienopyridines (eg, ticlopidine or prasugrel) or use of glycoprotein IIb/IIIa inhibitors during PCI may be helpful to overcome poor responsiveness and improve the long-term clinical outcome.57–59
The presented data in this study showed a significant relation between ADP-induced platelet aggregation by conventional light transmittance aggregometry and platelet activation by flow cytometry. Flow cytometric measurement of P-selectin is frequently used for monitoring the effects of clopidogrel. 27 We stimulated platelets with moderate ADP concentrations (5 μmol/L), thus excluding secondary effects not directly associated with purinergic stimulation. In agreement with our results, platelet aggregation studies showed a strong correlation with platelet receptor expression.17,21,35 Recently, Sbrana et al 35 showed that cytometric quantification of platelet markers, in particular CD62P, allows predicting aggregation response to ADP from flow data in patients treated with aspirin alone or with aspirin plus clopidogrel. An international standardization of this technique is still ongoing and different concentrations of ADP have been used to evaluate the inhibitory effect of clopidogrel treatment. 60
In this work, aggregation was expressed as the maximal percentage change in light transmittance from baseline. Peace et al 61 reported that this approach identifies gross platelet dysfunction and provides relatively high reproducibility and low variability in platelet aggregation responses. The time chosen to measure platelet aggregation is of importance to define hyporesponsiveness to clopidogrel. A 300-mg loading dose of clopidogrel can only elicit its full antiplatelet effect at 24 hours, in contrast to a 600-mg loading dose, which can achieve its maximum effect after only 4 hours.17,24,62 Thus, we assessed platelet reactivity more than 6 hours after administration of 600 mg loading dose of clopidogrel to reassure that platelet testing was performed when maximum inhibitory response had been achieved.
Using a single-blood sample testing posttreatment ADP-induced maximal intensity of platelet aggregation and activation, we identified a threshold determining a subgroup of low responders to dual antiplatelet therapy at higher risk of recurrent ischemic events after stenting. Posttreatment platelet aggregation of 12.5% and P-selectin expression levels of 18.5% were the optimal cutoff value to predict 6 months of post-discharge stent complications. This cutoff value is close to that obtained by Hochholzer et al (14%). 63 An arbitrary cutoff for the definition of low responsiveness (clopidogrel-dependent platelet inhibition <30%) was used by Geisler et al. 24 In fact, it might be for the patients’ sake to lower the cutoff value to segregate low responders from responders. Identification of poor responders among diabetic patients may be useful to select those who may potentially benefit from a more aggressive antithrombotic therapy; higher clopidogrel dose, alternative molecules, and adjuvant antiplatelet agents.24,59
Study Limitations
One limitation of the present investigation that deserves consideration is the assessment of platelet function at a single time point prior to the intervention. Although this time point is probably most useful in the clinical setting of PCI, baseline measurements before loading might have provided additional information.
In conclusion, low response to clopidogrel could be considered as a reliable predictor for the occurrence of ischemic events after PCI, particularly in diabetic patients. Poor metabolic control is linked to reduced platelet sensitivity. Posttreatment platelet reactivity may help to identify patients at increased risk who would benefit from intensified antiplatelet strategy. However, before platelet function testing can be widely applied to stratify patients following PCI, large randomized clinical trials must evaluate whether the benefits of an aggressive antiplatelet therapy in nonresponders outweigh any potential risk of increased bleeding.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.