
Abstract
Users of CT pulmonary angiography recognized that ancillary findings on CT pulmonary angiograms of patients in whom PE was excluded often provided useful information.1–5 Some ancillary findings on the CT angiogram, such as peripheral wedge-shaped densities, may suggest the need for further studies of PE because they suggest peripheral PE in the absence of direct visualization of an intraluminal thrombus.4,6 The extent to which such ancillary findings shown on CT angiograms are also shown on the plain chest radiograph, and whether the chest radiograph would contribute additional information or should be entirely supplanted by CT angiography is not known. Medicare claims of 220 961 patients with suspected acute PE in 2005 showed that 71.5% had a chest radiograph obtained on the same day as PE was diagnosed or evaluated. 7 It is not known whether plain chest radiographs of patients in whom PE is excluded show parenchymal or pleural abnormalities not shown as ancillary findings on the CT pulmonary angiogram. The purpose of this investigation is to test the hypothesis that plain chest radiographs may identify some abnormalities not shown as ancillary findings on CT pulmonary angiograms of patients in whom PE was excluded.
Materials and Methods
This is a retrospective study of patients who had negative CT pulmonary angiograms for suspected acute PE. Images were obtained with 64-detector Toshiba units (Toshiba America Medical System, Inc. Tustin, California). Reports of the contrast-enhanced CT pulmonary angiograms and plain chest radiographs were reviewed by 2 investigators working together. Teleoroentgenograms were obtained within 24 hours of the CT angiogram in 332 patients. Among these, 248 (75%) were obtained prior to the CT angiogram and 84 (25%) were obtained afterward. Portable chest radiographs were obtained within 24 hours of the CT angiogram in 193 patients. Among these, 139 (72%) were obtained prior to the CT angiogram and 54 (28%) were obtained afterward.
Statistical Analysis
Data were analyzed using SPSS Version 11.5 for Windows (SPSS Inc., Chicago, Illinois). Significant tests of equality of 2 proportions were carried out using the 2-tail Fisher exact test (http://www.graphpad.com/quickcalcs/contingency2.cfm). Although multiple comparisons were made, we did not use Bonferroni correction and considered P values of .05 or lower as significant.
Results
Reports of plain chest radiographs, either standard or portable, were reviewed in 525 patients with suspected acute PE who had negative CT pulmonary angiograms. The age of patients was 61 ± 18 years and 42% were males. Patients who had standard chest radiographs were younger than those who had portable chest radiographs, 58 ± 19 years compared with 65 ± 16 years (P < .0001). Gender distribution was similar, 132 (40%) of 332 males among those who had standard chest radiographs compared with 86 (45%) of 193 among those who had portable chest radiographs (nonsignificant [NS]). The proportion that had standard chest radiographs before the CT angiogram was 75% and the proportion that had portable chest radiographs before the CT angiogram was 72% (NS).
Ancillary Findings on CT Pulmonary Angiograms Compared With Standard Plain Chest Radiographs
Pulmonary parenchymal disease was shown in 301 (91%) of 332 patients in whom PE was excluded by CT angiography, who had standard chest radiographs (Table 1 ). Pulmonary parenchymal disease was shown in 60 (18%) only on the chest radiograph, 159 (48%) only on the CT angiogram, and in 82 (25%) on both. Among the 301 patients with pulmonary parenchymal disease, 60 (20%) showed it only on the plain chest radiograph, 159 (53%) showed it only on the CT angiogram, and 82 (27%) showed it on both. Atelectasis, airspace disease, and emphysema were the most frequently reported abnormalities on CT angiograms of patients who did not have PE (Table 1). Such findings were observed only on the plain chest radiograph in 7% to 14% of patients.
Findings on CT Pulmonary Angiograms and Standard Chest Radiographs in 332 Patients With No Pulmonary Embolism
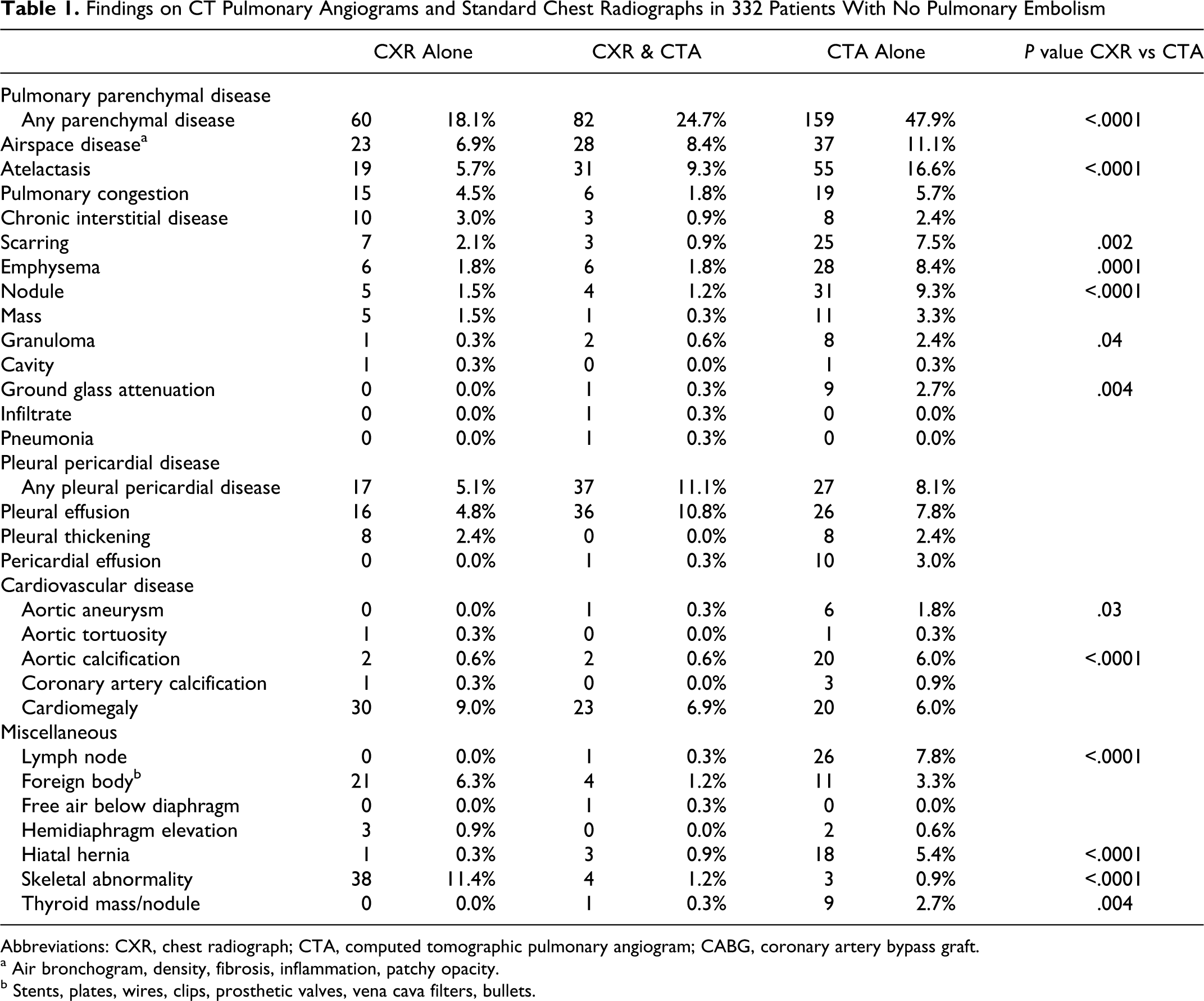
Abbreviations: CXR, chest radiograph; CTA, computed tomographic pulmonary angiogram; CABG, coronary artery bypass graft.
a Air bronchogram, density, fibrosis, inflammation, patchy opacity.
b Stents, plates, wires, clips, prosthetic valves, vena cava filters, bullets.
Pleural or pericardial disease was shown in 81 (24%) of 332 patients in whom PE was excluded who had standard chest radiographs (Table 1). Among these 17 (5%) showed it only on the plain chest radiograph, 27 (8%) showed it only on the CT angiogram, and 37 (11%) showed it on both. Among the 81 patients who showed pleural or pericardial disease, 17 (21%) showed only on the chest radiograph, 27 (33%) showed only on the CT angiogram, and 37 (46%) showed on both. Pleural effusion was the most frequently reported pleural or pericardial abnormality.
Cardiovascular disease
Aortic calcification and aortic aneurysms were reported more frequently on CT angiograms than on standard chest radiographs (Table 1).
Miscellaneous findings
Lymph nodes, hiatal hernias, and thyroid masses or nodules were reported more frequently on CT angiograms than on standard chest radiographs (Table 1). Skeletal abnormalities, however, were reported more frequently on standard chest radiographs.
Ancillary Findings on CT Pulmonary Angiograms Compared With Portable Chest Radiographs
Pulmonary parenchymal disease. This disease was shown in 177 (92%) of the 193 patients in whom PE was excluded by CT angiography, who had portable chest radiographs (Table 2 ). Pulmonary parenchymal disease was shown in 42 (22%) only on the portable chest radiograph, 94 (49%) only on the CT angiogram, and in 41 (21%) on both. The proportion of patients who showed parenchymal findings only on the portable chest radiograph was similar to the proportion shown only on the standard chest radiograph (22% vs 18%; NS). Among the 177 patients with no PE who showed pulmonary parenchymal disease, 42 (24%) showed it only on the plain chest radiograph, 94 (53%) showed it only on the CT angiogram, and 41 (23%) showed it on both. Atelectasis and pulmonary congestion were the most frequent pulmonary parenchymal abnormalities shown only on the portable chest radiograph of patients with no PE (Table 2).
Findings on CT Pulmonary Angiograms and Portable Chest Radiographs in 193 Patients With No Pulmonary Embolism
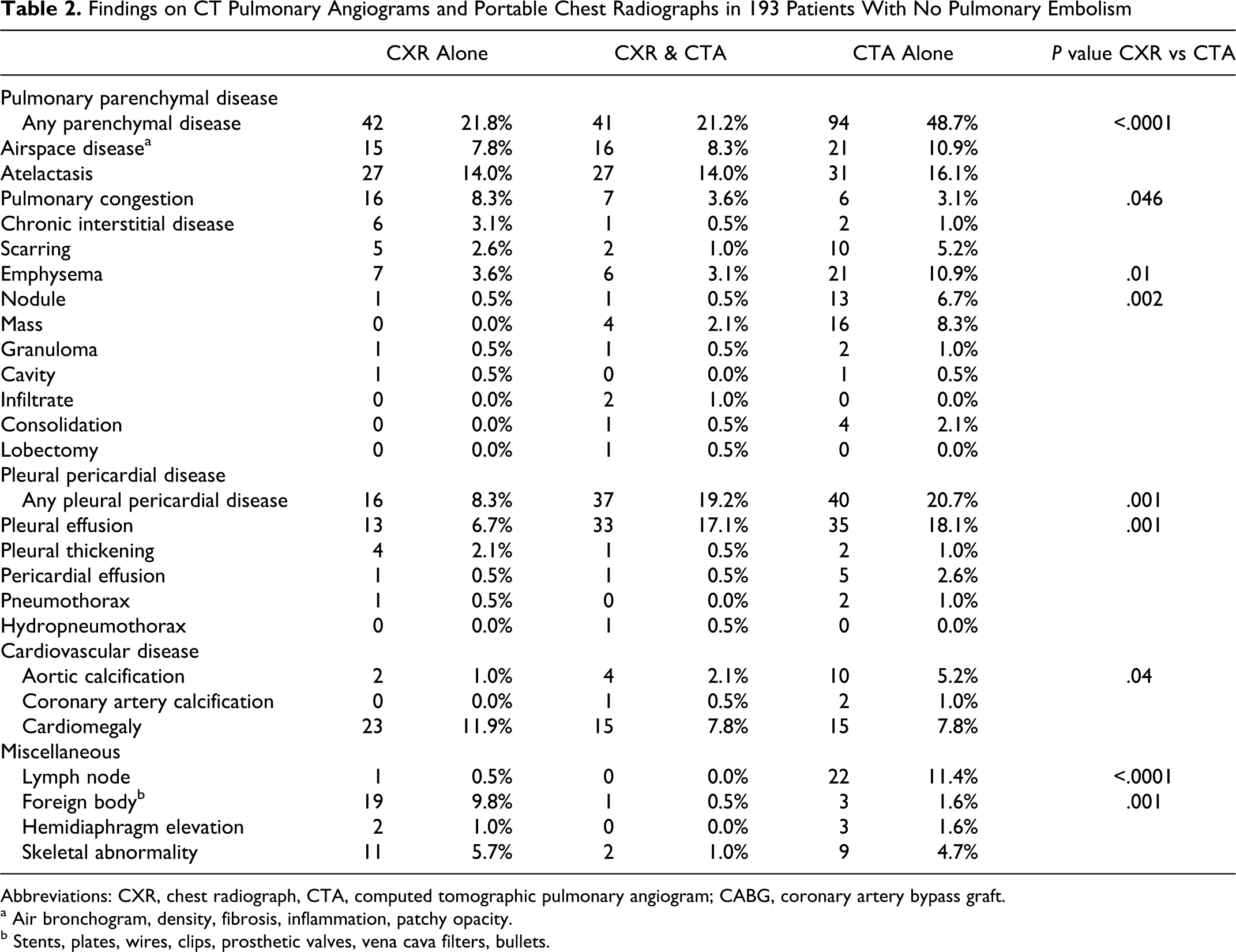
Abbreviations: CXR, chest radiograph, CTA, computed tomographic pulmonary angiogram; CABG, coronary artery bypass graft.
a Air bronchogram, density, fibrosis, inflammation, patchy opacity.
b Stents, plates, wires, clips, prosthetic valves, vena cava filters, bullets.
Pleural or pericardial disease. This disease was shown in 93 (48%) of the 193 patients in whom PE was excluded, and who had portable chest radiographs (Table 2). Among these 16 (8%) showed it only on the portable chest radiograph, 40 (21%) showed it only on the CT angiogram, and 37 (19%) showed it on both. Among the 93 patients who showed pleural or pericardial disease, 16 (17%) showed in only on the portable chest radiograph, 40 (43%) showed it only on the CT angiogram, and 37 (40%) showed it on both. Pleural effusion was the most frequent pleural or pericardial abnormality shown on the CT pulmonary angiogram and on the portable chest radiograph of patients with no PE.
Cardiovascular disease
Aortic calcifications were reported more frequently on CT angiograms than on portable chest radiographs (Table 2).
Miscellaneous findings
Lymph nodes were reported more frequently on CT angiograms than on portable chest radiographs (Table 2). Foreign bodies, however, were reported more frequently on portable chest radiographs.
Discussion
One of the advantages of CT pulmonary angiography is that it often shows pathology in patients in whom PE is excluded.1–5 We confirmed this and showed in addition that the plain chest radiograph also shows pulmonary parenchymal findings, in 18% and 22% (standard chest radiograph and portable chest radiograph, respectively) not reported on the CT angiogram. The ancillary findings rarely indicated an alternative diagnosis, although the findings may have been of clinical value. We did not reread the chest radiographs or the CT angiograms. Our purpose was to determine findings found in routine clinical practice at a community/teaching hospital.
The observation that pulmonary parenchymal abnormalities and pleural or pericardial abnormalities are often reported only on the plain chest radiograph, and not the CT pulmonary angiogram probably reflects the focus of interest of the interpreting radiologist, and not the ability of CT images to show such findings. Radiologists looking for PE on contrast-enhanced CT pulmonary angiograms often may be inattentive to other findings as a result of observer bias. Indeed, interpreters of CT pulmonary angiogram are often biased to exclude PE and may overlook ancillary findings not responsible for chest pain or shortness of breath. Such biases are generally less frequent with interpretation of the chest radiograph. On the other hand, there are instances where diagnostic accuracy of the chest radiograph can be superior to CT of the chest in conditions other than PE. Examples of this would be conditions associated with prior placement of metallic prostheses or clips. Computed tomography techniques suffer from insuppressible streak artifact, which often makes identification of a particular device difficult. Skeletal abnormalities are another example, because with CT angiography, user-defined levels of contrast are optimized for evaluation of images of the mediastinum and lung, and such levels of contrast are less effective for visualization of skeletal abnormalities.
The plain chest radiograph in patients with acute PE shows several radiographic signs that are neither sensitive nor specific.8,9 The radiographic signs of acute PE include oligemia, pleonemia of the obstructed lung, dilated hilar arteries, elevated hemidiaphragm, dilated pulmonary artery trunk, pleural effusion, atelectasis, and infiltrate or pulmonary parenchymal abnormality.8,10,11 Occasionally, cavity formation may occur with pulmonary infarction. 11 Dilatation of the azygos vein and superior vena cava also have been described. 10 Pulmonary edema has also been described. 10 It was thought by some to reflect underlying heart disease, 11 although pulmonary edema has been observed in patients with no prior cardiopulmonary disease. 8 Among patients with submassive or massive acute PE and no prior cardiopulmonary disease, a normal chest radiograph was observed in 16% 8 and 24%. 12 Greenspan et al suggested that the most useful aspect of the plain chest radiograph is to assist in the exclusion of disease processes such as pneumothorax or rib fracture, which may simulate PE. 13 Worsley et al indicated that a recent chest radiograph is particularly useful if an abnormal pattern is identified on the radionuclide perfusion lung scan. 14 Based on the investigations by Greenspan et al and Worsley et al, the American College of Radiology recommended a posterior and lateral chest radiograph as an important initial study because it may eliminate the need for an additional radiographic procedure by revealing an obvious reason for the acute symptoms. 15
Kim et al, among 57 patients with no PE, observed findings on the single detector CT angiogram in 67% that suggested or confirmed an alternate diagnosis. 1 Alternate diagnoses included pneumonia, cardiovascular disease, pulmonary fibrosis, trauma, malignancy, pleural disease, and postoperative changes. 1 Others showed additional pathology of importance,2,3 but the findings usually were not diagnostic of any particular disease. Enden and Klow, among 269 patients with no PE on a multidetector CT angiogram, observed ancillary findings in 82%. 3 The most frequent were pleural effusion (43%) and atelectasis (28%). 3 Shah et al, among 64 patients with no PE on single-detector CT angiograms, showed a pulmonary parenchymal abnormality in 88%. 2 The most frequent were atelectasis (64%) and linear opacities (39%). 2 They suggested that ancillary CT angiographic findings might suggest an alternative explanation for an acute clinical presentation when the CT angiogram is negative. 2 Karabulut and Kiroglu, among 79 patients in whom PE was excluded on dual or multidetector CT angiograms, showed parenchymal findings on the CT angiogram in 84%. 5 Atelactasis and ground glass attenuation were the most frequent findings. 5 Coche et al, among 62 patients with no PE, showed wedge-shaped consolidation in 27%, nonwedge-shaped consolidation in 24%, and isolated atelectasis in 27% on single-detector CT angiograms. 4 They indicated that parenchymal findings on CT angiograms might suggest further investigations when CT angiograms are inconclusive in showing PE. 4 Reissig et al, among 23 patients without PE, observed peripheral consolidations on the single-detector CT angiograms in 26%. 6 They suggested that if parenchymal changes are shown on the CT angiogram, peripheral PE should be considered even in the absence of directly visible emboli. 6
Strengths of this investigation are the large number of patients evaluated, 525. This is the only investigation, to our knowledge, that assesses ancillary findings on the CT pulmonary angiogram and compares them with findings on the plain chest radiograph. We evaluated the reports of the CT angiograms and the reports of the chest radiographs. This was strength, from the point of view that the results reflect the observations of radiologists in a clinical setting. It was a weakness to the extent that rereading of the images may have shown different results. A weakness is that we did not have definitions of the ancillary findings. We reported the findings as described by the radiologists. Another possible weakness is that there was no reference standard to validate which of the ancillary findings were correct.
Our investigation suggests that abnormalities are often described on plain chest radiographs of patients in whom PE is excluded, and such findings may not be described as ancillary findings on CT pulmonary angiograms. This suggests a need for ancillary findings on CT pulmonary angiograms to be described systematically. At present, however, plain chest radiographs in some patients show ancillary findings not reported on CT angiograms.
Footnotes
All authors had access to the data and played a role in writing this manuscript.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.