
Abstract
Mean platelet volume (MPV) was studied in subclinical hypothyroidism (SH) and the results are conflicting. The aim of this study is to assess how MPV is affected in overt hypothyroidism (OH) and mild SH, the 2 end points of hypothyroidism, in patients having low cardiac risk. Premenopausal women without any cardiac risk, 18 with OH, 30 with mild SH, and 37 euthyroid controls were enrolled. Overt hypothyroidism group had higher low-density lipoprotein cholesterol (LDL-C) and total cholesterol levels than the control group (P < .001 and P < .05, respectively). Increase in MPV was insignificant in OH group when compared with SH and control groups. No correlation was observed between MPV and metabolic and hormonal parameters. Both OH and SH did not influence MPV and high-sensitivity C-reactive protein (hs-CRP) in patients with low cardiovascular risk, but these findings need to be further evaluated in this patient group.
Keywords
Introduction
Coronary artery disease is still the most important leading cause of death in industrialized countries. 1 Although it is controversial and the cutoff values for increased mean platelet volume (MPV) in prediction of cardiovascular risk is not clear, large platelets may have a role in the pathogenesis of cardiovascular disease. 2–4 A clear causal relationship between thyroid disorders and cardiovascular disease has not been shown yet. 5 Elevation of thyroid-stimulating hormone (TSH) with normal free thyroid hormone levels is defined as subclinical hypothyroidism (SH) and levothroxine replacement therapy for SH is suggested for patients younger than 65 years if TSH levels >10 mIU/mL and/or thyroid peroxidase (TPO) antibodies are present. In participants with TSH <10 mIU/mL and negative for TPO antibody, replacement is suggested for patients having symptoms of hypothyroidism, high cardiovascular risk, infertility, presence of pregnancy, or planning pregnancy. 6 The clinical significance and medical management of mild SH are not clear. There is conflicting data about how SH affects MPV and to our knowledge there is no data about MPV in overt hypothyroidism (OH). 7–9 The aim of this study is to evaluate MPV in 2 end points of hypothyroidism, OH and mild SH (TSH levels between 4 and 10 mIU/mL), in a patient group who have low cardiovascular risk.
Materials and Methods
Patients
The study was conducted in endocrinology outpatient unit. Nonobese women of reproductive age, having menstruation, aged between 16 and 40 years without a known cardiovascular risk factor were included. Patients with existing cardiovascular disease were excluded. Patients with active infection, having a history for antiplatelet and antilipid therapy, smoking, hypertension, diabetes, anemia, or any of chronic diseases were excluded. Patients with SH having sonographic features of chronic thyroiditis with or without positive antithyroid antibodies were included. A total of 30 patients having TSH levels between 4 and 10 mIU/mL without an indication for levothyroxine replacement were enrolled in the SH group. Patients in the OH group (n = 18) had chronic thyroiditis and or were noncompliant to ongoing levothyroxine replacement therapy. Patients who did not use levothyroxine replacement for at least 3 months before admission were included in the OH group. A total of 37 women who had no clinical, laboratory, or radiological signs of thyroid disease formed the control group. Blood pressures, anthropometric measurements including height, body weight, and body mass index ([BMI] weight kg/height m 2 ) were recorded. Patients signed their informed consent and the study was approved by the local ethical committee (13.01.2011/01/15).
Laboratory Analysis
Free triiodothyronine (fT3), free thyroxine (fT4), TSH, and anti-TPO antibody levels were measured with the Roche/Hitachi modular analytics E170 module (Roche Diagnostics Ltd, Rotkreuz, Switzerland). In blood samples, platelet parameters were determined after assessment of thyroid functions. Samples were collected in a citrate-containing tube and studied within 30 minutes. Platelet parameters were studied by an automated blood counter (Beckman Coulter Gen.S, Minesota, Minnesota). Lipid analysis was performed with Abbott Aeroset autoanalyzer (Chicago, IL, USA) using Abbott kits. Serum low-density lipoprotein cholesterol (LDL-C) level was determined according to Friedewald formula. High-sensitive C-reactive protein (hs-CRP) is analyzed by nephelometric method.
Statistical Analysis
SPSS for windows 11.0 software was used for statistical analysis. Data were defined as mean ± standard deviation (SD). Groups were compared with 1-way analysis of variance (ANOVA) for variables that show a normal distribution and with Mann-Whitney U test for variables that did not show a normal distribution. Pearson correlation coefficient was used for correlation analysis. Statistical significance was defined when P < .05.
Results
Clinical and laboratory characteristics of the study groups were shown in Table 1 . Ages of 3 groups were similar. Although BMI of OH group was higher than both SH and control groups (P < .05 and P < .001, respectively), SH and control groups had similar BMI. Thyroid-stimulating hormone level of OH group was higher than control and SH groups (P < .001). Both SH and OH groups had lower fT4 levels when compared with control group (P < .05 and P < .001, respectively). Overt hypothyroidism group had lower fT3 level than control group (P < .001). Among the metabolic variables, only LDL-C and total cholesterol levels differed between the study groups (Figure 1 ). Overt hypothyroidism group showed higher LDL-C and total cholesterol levels when compared with control group (P < .001 and P < .05, respectively). Both SH and OH groups had higher total cholesterol levels than control group (P < .05). All of the study groups had similar hs-CRP levels. Although MPV of OH was higher than SH and control groups, it was statistically insignificant (Figure 1). Subclinical hypothyroidism and control groups had similar MPV. Low-density lipoprotein cholesterol showed negative correlation with fT4 and positive correlation with TSH (r = −.565, P < .001 and r = .598, P < .001, respectively). No correlation was detected between MPV and any of metabolic and hormonal parameters.
Demographic, Metabolic, and Hormonal Characteristics of Patients Groups
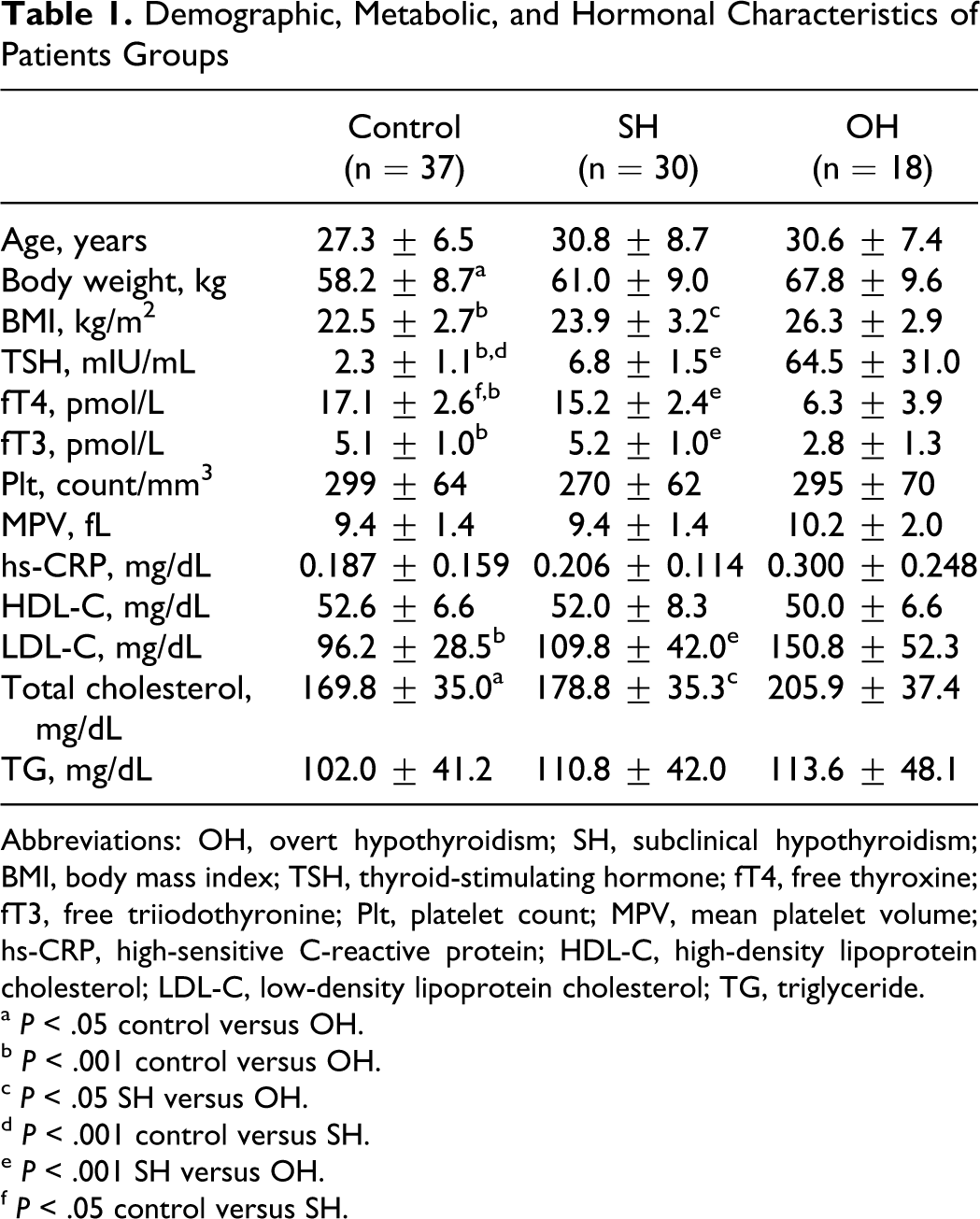
Abbreviations: OH, overt hypothyroidism; SH, subclinical hypothyroidism; BMI, body mass index; TSH, thyroid-stimulating hormone; fT4, free thyroxine; fT3, free triiodothyronine; Plt, platelet count; MPV, mean platelet volume; hs-CRP, high-sensitive C-reactive protein; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TG, triglyceride.
a P < .05 control versus OH.
b P < .001 control versus OH.
c P < .05 SH versus OH.
d P < .001 control versus SH.
e P < .001 SH versus OH.
f P < .05 control versus SH.
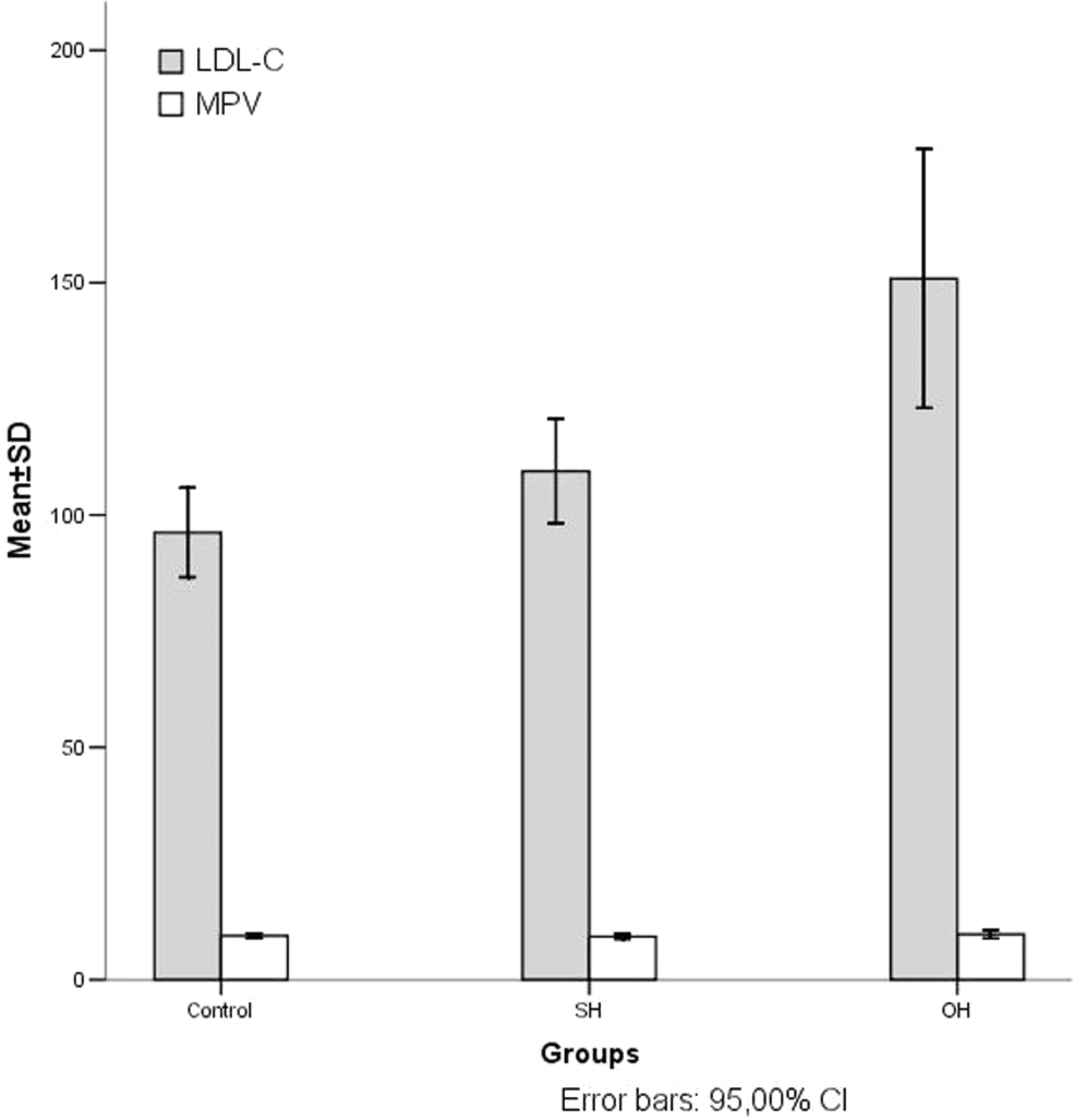
Mean platelet volume and low-density lipoprotein cholesterol levels of study groups. MPV indicates mean platelet volume; LDL-C, low-density lipoprotein cholesterol.
Discussion
Cardiovascular disease is still the most frequent cause of mortality in the developed countries. 10 Increased MPV, reflecting increased activity of platelets, has been reported to associate with ischemic cardiac events and predict future myocardial infarction. 11 The association between thyroid dysfunction and cardiovascular risk and how do different thyroid pathologies affect MPV is scarce. 7–9,12 We evaluated MPV, hs-CRP, and metabolic parameters in a group of women with mild SH (TSH levels between 4 and 10 mIU/mL) and OH, both with low cardiovascular risk.
To our knowledge MPV has not been studied in OH as a cardiovascular event predictor but have shown to be increased in SH in 3 different studies. 7–9 These studies compared MPV in patients with different degrees of SH with normal controls, including both men and women. We evaluated MPV in both end points of hypothyroidism, OH and mild SH, in patients who have low cardiovascular risk (nonobese, nonsmoker premenopausal women, age <50 years, without family history of coronary artery disease) and found the MPV unaffected in both mild SH and OH patient groups when compared with the control group. In one study, it was shown that obesity increases MPV, and obesity is related to increased low-grade inflammation. 13 Studies showing MPV increase in SH included obese and older patients when compared to our study sample. The difference in patient selection may be a causal factor for unaffected MPV in our study. In a meta-analysis no clear-cut association was found between hypothyroidism and cardiovascular risk, which suggests our findings. 5
It is presumed that MPV is increased by the effects of several inflammatory cytokines such as interleukins and nitric oxide, but no chronic inflammation has been reported in the group with SH. 14–17 On the basis of cumulative evidence, the effects of merely SH or OH on MPV seem unlikely without an additional risk factor affecting low-grade inflammation. We have no other evidence of inflammation except for hs-CRP in our study. Studies showing increased MPV in SH lack in determination of several cytokines in the same patient population which limits to have a definite conclusion about MPV in SH. Further studies are needed to identify the inflammation in OH and SH group of patients and to determine the effect of SH and OH in patient groups without cardiac risk factors.
There is no clear conclusion about the cutoff for MPV in predicting future cardiovascular events. 18 Some reports suggest 8.4 fL, while others suggest higher values such as 11.75 fL as a cutoff value. Lack of standardization of the methods of MPV measurement is another handicap of the studies, which objected to show the significance of MPV in cardiovascular risk prediction. 18 Studies indicating an increase in MPV in patients with SH reported a wide range of MPV (6–12.4 fL), and these values are lower than the reported cutoff values for cardiovascular risk prediction. 7 Thus, the presence of SH alone does not seem to be the only causal factor in the elevation of MPV.
Unlike previous reports, we also evaluated MPV in patients with OH and found an insignificant increase in MPV when compared with mild SH and healthy participants which did not reach to the values of MPV in the highest quintile defined for predicting cardiovascular events. 11 This limited elevation of MPV in OH group may be due to our young study sample having low cardiovascular risk. Addition of several risk factors hypothetically may burden this mild elevation of MPV in OH, even in young patient groups.
In conclusion, this study showed that OH and SH did not influence MPV and hs-CRP in patients having low cardiovascular risk. Further prospective studies evaluating the effect of levothyroxine replacement in symptomatic patients having mild SH are needed to identify the effect of thyroid hormonal status on platelet size and function.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.