
Abstract
Background: Pulmonary arterial hypertension (PAH) is a chronic progressive disease characterized by persistent elevation of pulmonary artery pressure. Vasoconstriction, remodeling, and thrombosis cause increased pulmonary vascular resistance and pressure. Previous studies have demonstrated that platelet activation occurs in patients with PAH. Our aim was to assess the mean platelet volume (MPV), an indicator of platelet activation in patients with PAH. Patients and Method: The study group consisted of 22 patients with PAH. An age-, gender-, and body mass index–matched control group was composed of 25 healthy volunteers. All patients underwent physical examination, echocardiography, and diagnostic cardiac catheterization. We measured serum MPV values and platelet counts in patients with PAH and control participant. Results: MPV was significantly higher among the patients with PAH when compared with control group (8.68 ± 0.87 vs 8.02 ± 0.68 fl, respectively; P = .006). Conclusion: We have shown that MPV was elevated in patients with PAH.
Introduction
Pulmonary hypertension (PAH) is a chronic and progressive disease characterized by a persistent elevation of pulmonary artery pressure and pulmonary vascular resistance, which ultimately leads to right heart failure and death. Vasoconstriction, remodeling, and thrombosis contribute to some extent to increased pulmonary vascular resistance and pressure. 1 Regardless of the etiology, thrombotic pulmonary vascular lesions are an integral part of pulmonary vascular pathology that includes, in addition, vasoconstriction and remodeling.
There are few observations that have shown increased platelet aggregation and activation in patients with PAH.2–6
Mean platelet volume (MPV) is a simple and easy method of assessing platelet function.7,8 In comparison to smaller ones, larger platelets have more granules, aggregate more rapidly with collagen, have higher thromboxane A2 level, and express more glycoprotein Ib and IIb/IIIa receptors.9–11
Platelets have central role in pathophysiology of atherothrombotic cardiovascular diseases. Increased MPV has been shown in patients with cardiovascular diseases and in patient groups with known coronary artery disease risk factors. 8 Moreover, increased MPV has also prognostic role in cardiovascular diseases, for example, it is associated with higher mortality following myocardial infarction. 8 These findings raise the hypothesis of the potential importance of MPV in the underlying pathophysiology of atherothrombotic cardiovascular disease. As we mentioned above, thrombosis has an important role in PAH. As a result, we aimed to investigate the platelet indices including MPV and platelet counts in patients with PAH in this study.
Patients and Methods
Study Population
The study group consisted of 22 patients with PAH (17 females, 5 males, mean age 57.8 ± 14.9 years). An age-, gender-, and body mass index (BMI)–matched control group was composed of 25 healthy volunteers (17 females, 8 males with a mean age 56.6 ± 8.7 years). In addition to the clinical presentation, all patients underwent physical examination, echocardiography, and diagnostic cardiac catheterization. The control participants underwent physical examination and echocardiography and they showed normal cardiac findings. The diagnosis of pulmonary hypertension was defined as a mean pulmonary artery pressure at rest of ≥25 mm Hg. 12 The etiologies were idiopathic in 17 patients and PAH associated with congenital heart disease in 5 patients.
Exclusion criteria were left ventricular dysfunction, valvular heart disease, lung disease, diabetes mellitus, chronic renal disease, or hepatic disease. None of the participants were on anticoagulant and antiplatelet drug therapy including aspirin on admission. The study was approved by the institutional ethics committee and all patients gave their informed consent.
Biochemical Measurements
Blood samples were drawn from the antecubital vein by careful vein puncture in a 21-G sterile syringe without stasis at 08.00 to 10.00
Statistical Analysis
Data were analyzed with the SPSS software version 10.0 for Windows. Continuous variables from the study groups were reported as mean ± standard deviation, categorical variables as percentages. To compare continuous variables, the Student t-test or Mann-Whitney U test were used where appropriate. Categorical variables were compared with the chi-square test. Statistical significance was defined as P < .05.
Results
Clinical features of the study and control groups and hemodynamic findings of patients with PAH were summarized in Table 1. There were no statistically significant differences between the 2 groups with respect to age, gender, BMI, systolic and diastolic blood pressures, and levels of glucose, creatinine, total cholesterol, triglyceride, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, hemoglobin, white blood cell (WBC), and platelet count. Mean platelet volume was significantly higher among patients with PAH when compared with control group (8.68 ± 0.87 vs 8.02 ± 0.68 fl, respectively; P = .006) (Table 2). Platelet counts tended to decrease from control group to the patients with PAH. However, the difference did not reach a statistically significant level.
Comparison of the Clinical, Laboratory and Hemodynamic Characteristics of the Patients With PAH and Control Participants
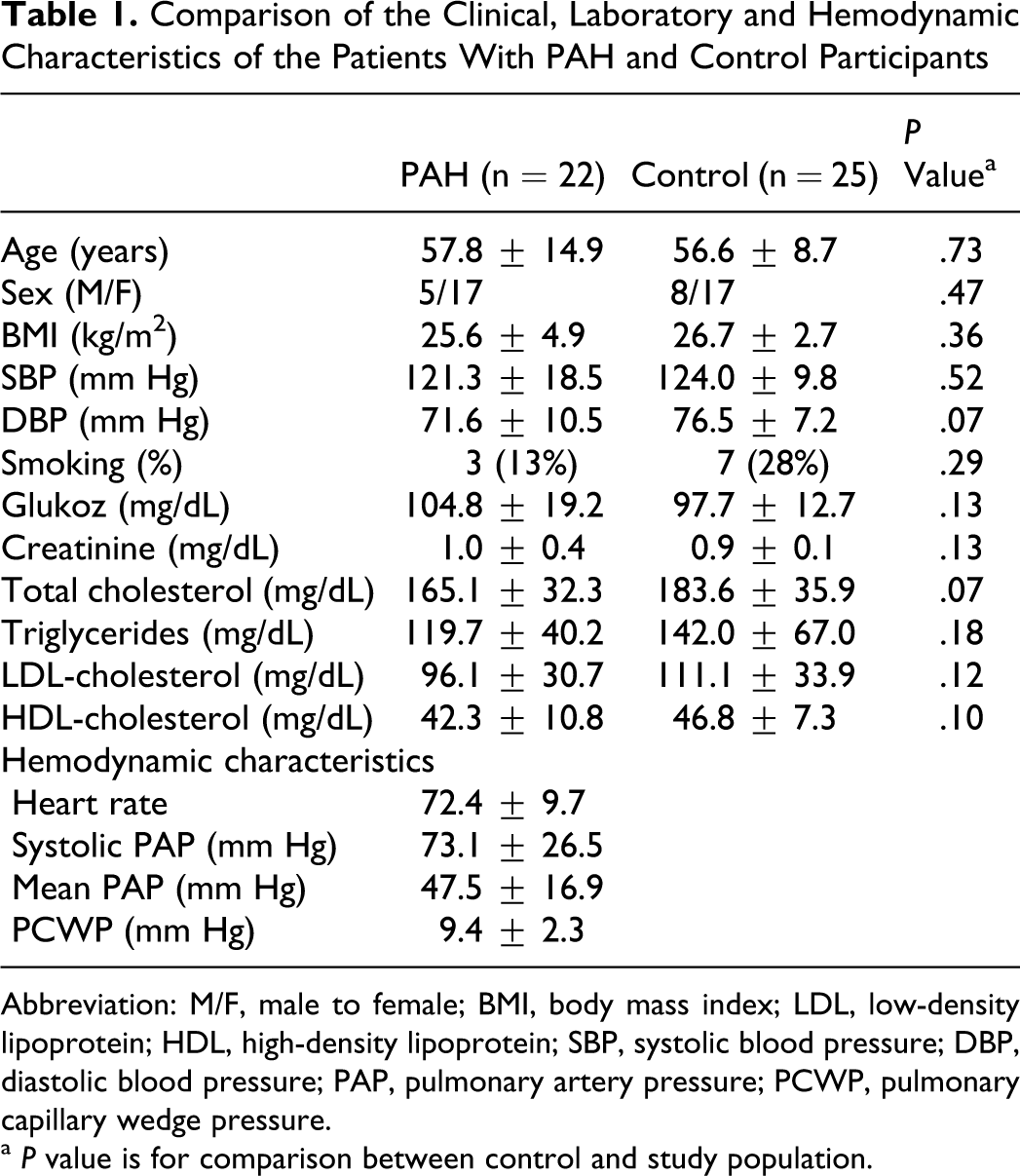
Abbreviation: M/F, male to female; BMI, body mass index; LDL, low-density lipoprotein; HDL, high-density lipoprotein; SBP, systolic blood pressure; DBP, diastolic blood pressure; PAP, pulmonary artery pressure; PCWP, pulmonary capillary wedge pressure.
a P value is for comparison between control and study population.
Comparison of the Platelet Indices of the Patients With PAH and Control Participants
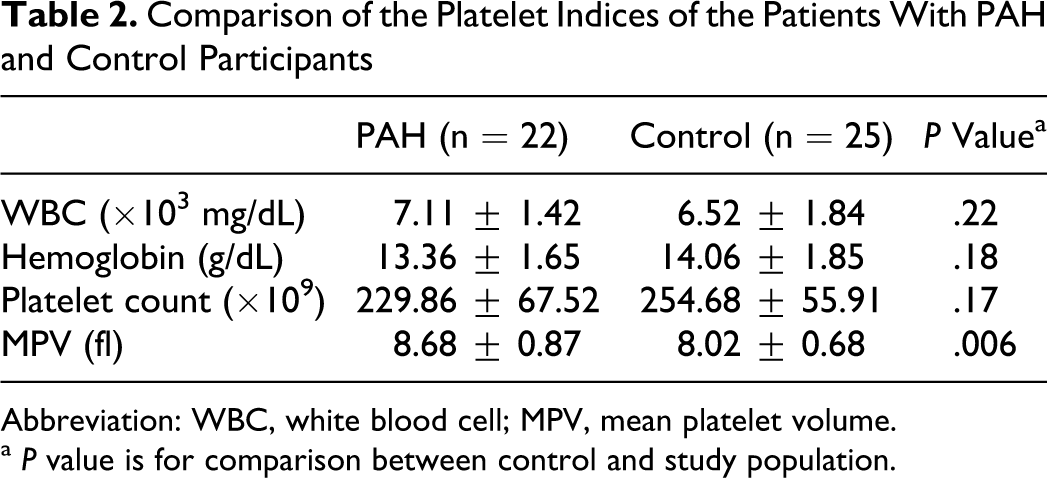
Abbreviation: WBC, white blood cell; MPV, mean platelet volume.
a P value is for comparison between control and study population.
Discussion
In the present study, we examined MPV, an indicator of platelet activation in patients with PAH. We found that MPV was significantly higher in patients with PAH.
Vasoconstriction, vascular wall remodeling, and thrombosis are considered as possible etiologies of primary pulmonary hypertension. 1 In situ thrombosis is a prominent finding in pulmonary vessels from patients with primary pulmonary hypertension. 13 It may result from injury to the endothelium, abnormal fibrinolysis, enhanced procoagulant activity, and platelet abnormalities.13,14
The previous reports have shown increased platelet aggregation and activation in patients with PAH.2–6 The degree of platelet activity was also associated with functional class and survival.4,5
Mean platelet volume is a simple and easy method of assessing platelet function and reflects the platelet production rate and stimulation.7,8 Platelets are enucleate cells measuring approximately 1 to 2 μm in length with an average life span of 8 to 10 days, which are formed via cytoplasmic fragmentation of bone-marrow derived megakaryocytes. Platelets are heterogeneous in size, density, and reactivity. Larger platelets are both metabolically and enzymatically more active than smaller platelets and they have a greater prothrombotic potential. 15
Elevated MPV is associated with other markers of platelet activity, including increased platelet aggregation, increased thromboxane synthesis and b-thromboglobulin release, and increased expression of adhesion molecules. 16 Furthermore, higher MPV is observed in patients with smoking, 17 diabetes mellitus, 18 obesity, 19 hypertension, 20 and hypercholesterolemia, 21 suggesting a common mechanism by which these factors may increase the risk of cardiovascular disease.
There are some proposed mechanisms for increased platelet activation in PAH. Firstly, pulmonary vascular endothelial dysfunction might lead to platelet activation and local thrombosis. 22 Secondly, systemic inflammation in patients with PAH might cause platelet activation. 23 Inflammation is an important feature of PAH, and increased circulating levels of cytokines including interleukin-6 (IL-6) was reported in patients with PAH and increased levels of cytokines were adversely associated with survival. 23 Platelet size is regulated at the level of the megakaryocyte. Researches reported that cytokines such as IL-3 or IL-6 influence megakaryocyte ploidy and can lead to the production of more reactive and larger platelets.24,25 So IL-6, which is increased in patients with PAH, can also cause an increase in MPV values by stimulating the megakaryocyte ploidy.
To the best of our knowledge, there is only one data about MPV in patients with PAH. Can et al found that MPV values in patients with PAH were significantly higher than controls. 2 Our results confirm this study. Actually, optimal cut-off for distinguishing increased risk for MPV is not known. Muscari et al found a direct association between an MPV ≥ 8.4 fl (the high tertile of its distribution) and ischemic ECG changes. 26 Our MPV values in patients with PAH were above this value.
Platelet volume is mainly determined in the bone marrow. It is supposed that the large platelets are caused by a reduced fragmentation of megakaryocytes. Mean platelet volume has been shown to inversely correlate with the total platelet count, which could even suggest the consumption of small platelets and a compensatory production of larger reticulated platelets. 27 In our study, platelet counts tended to decrease from control group to the patients with PAH. However, the difference did not reach a statistically significant level.
Our study has some limitations. First, the number of patients was small mostly due to numerous exclusion criteria. Second, our analysis was based on a simple baseline determination at single time point that may not reflect the patient status over long periods. Third, correlation of platelet indices with hemodynamic variables would be important, however, our sample size was too small.
In conclusion, we have shown that MPV was significantly elevated in patients with PAH compared to control participant. These data indicate that increased MPV, an indicator of platelet activity, are present in PAH. There is no study about effect of higher MPV on prognosis of patients with PAH. Elevated MPV values might also indicate that PAH patients with higher MPV may have a higher risk of systemic thromboembolism due to increased platelet activation. Further randomized studies with larger sample size are required to assess whether MPV identify patients with PAH at increased clinical risk and whether therapeutic modification of this marker may lead to improvement in clinical course of disease.
Footnotes
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.