
Abstract
Keywords
Introduction
In previous studies on patients with hip fracture (HF), symptomatic venous thromboembolism (VTE), including fatal events, occurred at a rate between 1.3% and 8.2% within 3 months after hospital admission, despite the use of thromboprophylaxis. 1 Events with arterial origin are also common in these patients. A pooled analysis of cohort studies reported that vascular events contributed to 50% of all deaths after HF with similar proportions due to ischemic heart disease, cardiac failure, and pulmonary embolism. 2
The main reason for the high rate of vascular complications after HF is presumed to be activation of coagulation with thrombin generation via the extrinsic pathway triggered by tissue factor originating from the fracture site. 2 Thus, thrombin generation is already ongoing when the patient arrives at the hospital and is further enhanced by the operative procedure carried out to fix the fracture. When thrombin is generated, prothrombin fragment 1 + 2 (F1 + 2) is released from prothrombin and excreted in the urine (uF1 + 2) where it can be measured by an enzyme-linked immunosorbent assay (ELISA). Previous studies have shown increased levels of uF1 + 2 in patients experiencing vascular thrombotic complications, both venous and arterial, after total hip and total knee arthroplasty (THA and TKA).3 –5
The current study was undertaken to document the natural history of uF1 + 2 excretion in elderly patients during and after a HF.
Methods
The study was a prospective pilot study. Patients with HF older than 65 years of age, permanently living in Denmark, and admitted to Aarhus University Hospital, Aarhus, Denmark, with a radiologically verified fracture of the hip needing operative treatment were asked to participate. Exclusion criteria were denied written informed consent, dementia, known renal insufficiency, lack of walking ability, and contraindications to antithrombotic treatment.
The study was conducted in accordance with The Declaration of Helsinki and approved by the local Ethics Committee; the study upheld the standards of Good Clinical Practise Guidelines (ICH GCP) and was notified to the Danish data protection agency.
Study Procedures
After inclusion in the study, patient characteristics (gender and age) and fracture type were noted. Operative treatment of the fracture was carried out within 24 hours after hospital admission in most cases. After the operation, the type of procedure and complications were registered. Standard operative procedures and after-treatment were used. Patients were allowed full weight bearing after surgery. Training was undertaken by physiotherapists at the hospital or in rehabilitation centers.
Thromboprophylaxis with fondaparinux, 2.5 mg subcutaneously, was started 6 to 8 hours after operation and continued for 7 days. Extended prophylaxis was not used. At follow-up on day 90 ± 10, patients were contacted by phone, mail, or seen in the outpatient clinic and asked questions about their health status in the postoperative period. Simultaneously, the Danish Central Health Care Registry was used to determine whether any patients had registered any kind of hospital contact. All vascular complications (venous and/or arterial) and deaths that occurred during the study were recorded and verified by hospital records.
Blood and Urine Sampling and Analyses
During the study, blood sampling and repeated spot urine sampling were performed according to the study overview shown in Figure 1. Blood samples were taken at admission. Serum creatinine was analyzed using standard laboratory technique. To evaluate renal function, creatinine clearance was calculated using the following equation by Cockroft and Gault 6 : creatinine clearance (mL/min) for men: (1.23 × (140 − age) × weight)/se-creatinine and for women: (1.04 × (140 − age) × weight)/se-creatinine (age in years and weight in kg and se-creatinine in µmol/L).
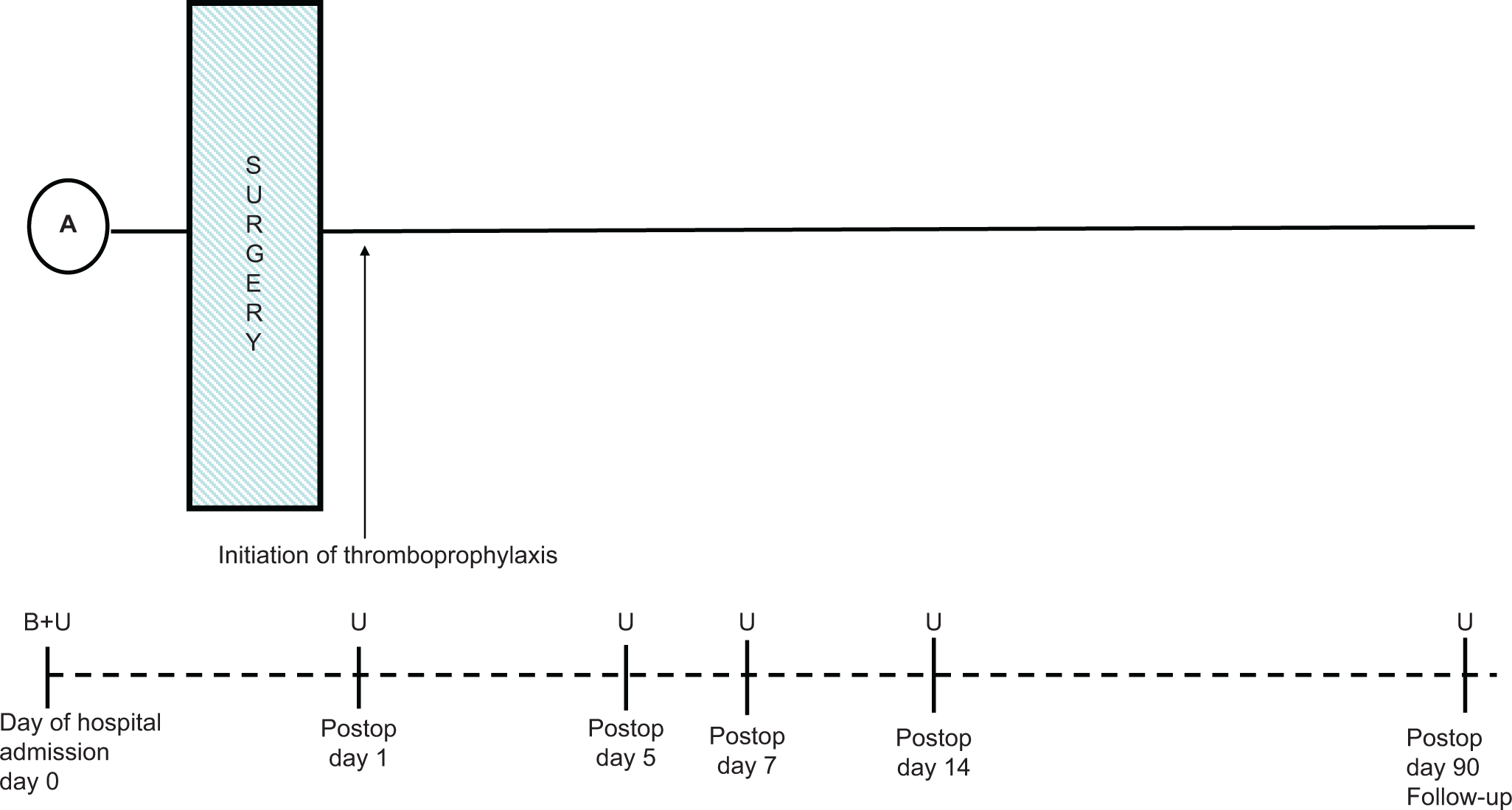
Study overview. A indicates day of hospital admission; B, blood samples; U, urine samples.
The first urine sample was collected at hospital admission (day 0). In the postoperative period, urine samples were collected in the morning on days 1, 5, 7, 14, and at follow-up on day 90 (Figure 1). After collection, the urine samples were snap frozen and stored at −80°C until batch analysis after the last patient had completed the study. Levels of uF1 + 2 were measured using a commercially available ELISA kit (Enzygnost F1 + 2, Monoclonal; Dade Behring, Marburg, Germany) that can be used both in citrated plasma and in urine. The kit is the same we have used in a previously published study. 4 The measuring interval is between 20 and 1200 pmol/L. The precision and reproducibility is described in the package insert. According to this, the coefficient of variance (CV) was between 3.6% and 5.5% within a reference interval between 40 and 700 pmol/L, and CV for the day-to-day variation was between 4.4% and 11.2%. A BEP 2000 analyzer (Dade Behring) was used for the analyses as described previously.4,5 All analyses were done by double measurements.
Statistics
Descriptive statistical methods were used. Basic characteristics and uF1 + 2 levels during the observational period were illustrated by median and ranges. In case of double measurements, the average was used in calculations. Values < 20 pmol/L and >1200 pmol/L were used as 20 pmol/L and 1,200 pmol/L, respectively, in the calculations. The nonparametric Wilcoxon rank sum test was used to compare medians of uF1 + 2 levels on the various days of measurement. The results were considered statistically significant if the 2-sided P value was <.05.
Results
The inclusion period was between September 11 and November 5, 2008. A total of 32 patients, 25 women and 7 men, were included. One female patient with a psychiatric diagnosis was excluded before the first urine sampling because she withdrew her consent to participate (patient no 19); thus, 31 patients completed the study. The median age was 84 years (range: 70-98), median weight was 61.5 kg (range: 44-75), and median height was 165 cm (range: 151-180). The median creatinine clearance was 53.5 mL/min (range: 22-93). The fracture types included 14 femoral neck fractures, 14 intertrochanteric fractures, and 3 subtrochanteric fractures. Patients underwent the following operative procedures: 3 had cannulated screws, 14 had a dynamic hip screw, 4 had an intramedullary nail, and 10 had a cemented hemiarthroplasty.
The median uF1 + 2 levels on the various days of measurement are shown in Table 1 and Figure 2. The median uF1 + 2 level at admission to hospital was 158.6 (range 27.2 -> 1200) pmol/L, and it was statistically, significantly increased compared with the level at follow-up (day 90) 30.3 (range < 20−168) pmol/L (P = 4.9 × 10−7). Maximum uF1 + 2 levels were seen on day 1 (the day after surgery) that is, 217.6 pmol/L (range: 62.6-404.5), which was even more increased compared with the level at day 90 (P = 9 × 10−7). Decreasing uF1 + 2 levels were seen on the following days of measurement until normalization at follow-up. In general, highly pronounced inter-individual variations were noted of the uF1 + 2 levels, especially during the first week after the fracture (Figure 3).
Median uF1 + 2 and Range (pmol/L) in All Patients, in Patients Operated With Either Hemiarthroplasty or Osteosynthesis, and in Patients With or Without Vascular Thrombotic Events/Death
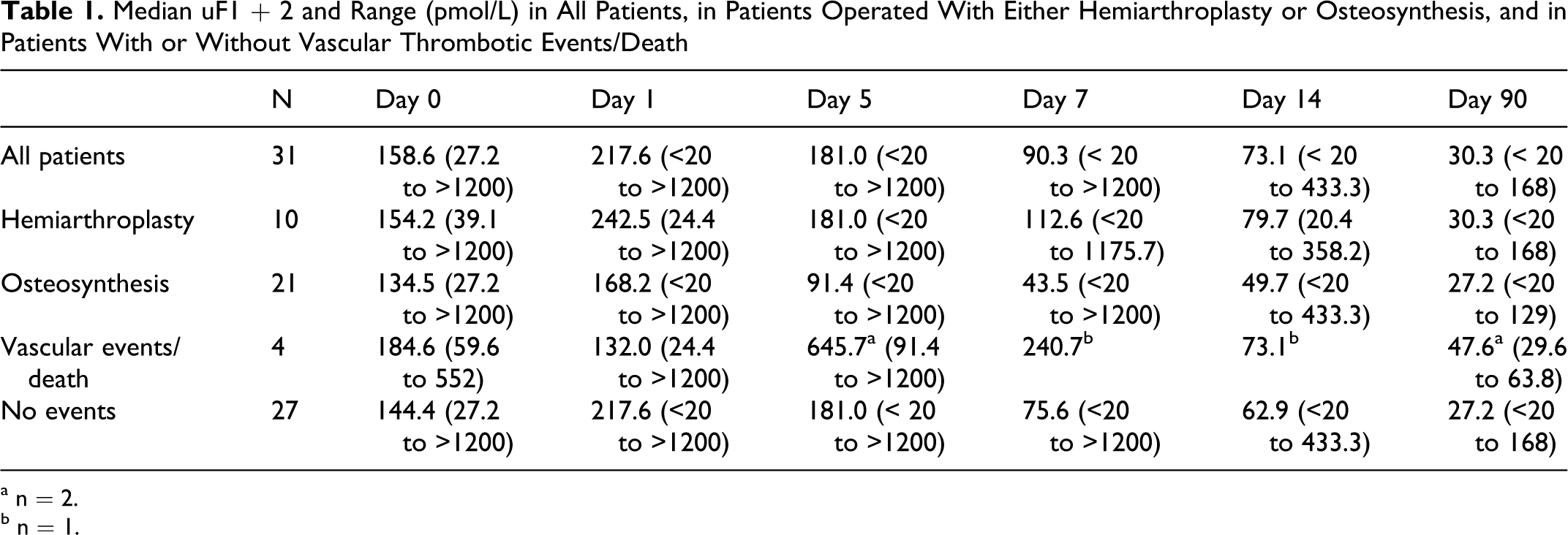
a n = 2.
b n = 1.
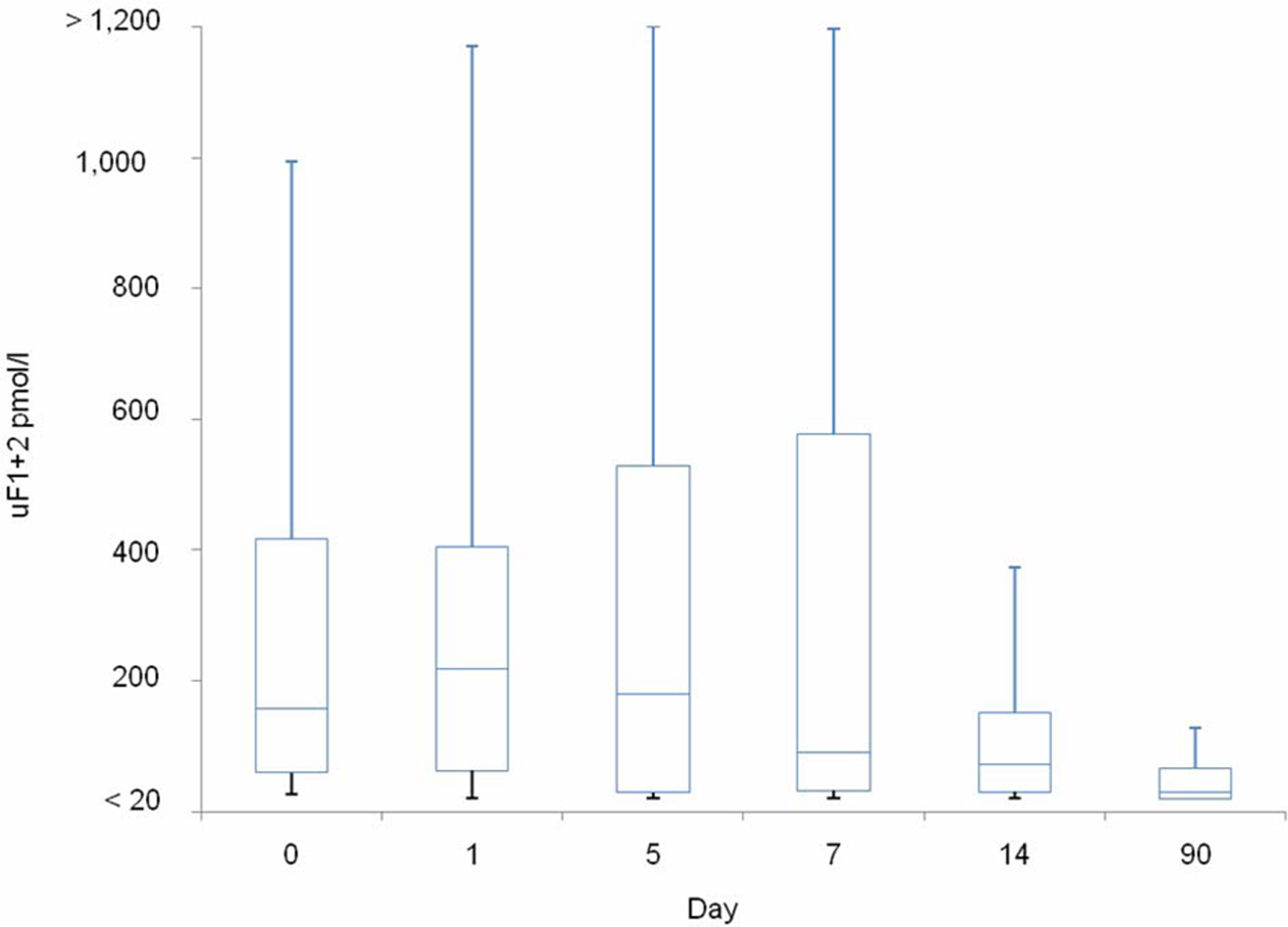
Box plot showing the F1 + 2 levels in a spot urine (uF1 + 2) pmol/L on the various days of measurement (N = 31). Median (line in box), quartiles (box), 95% of observations (wiskers).
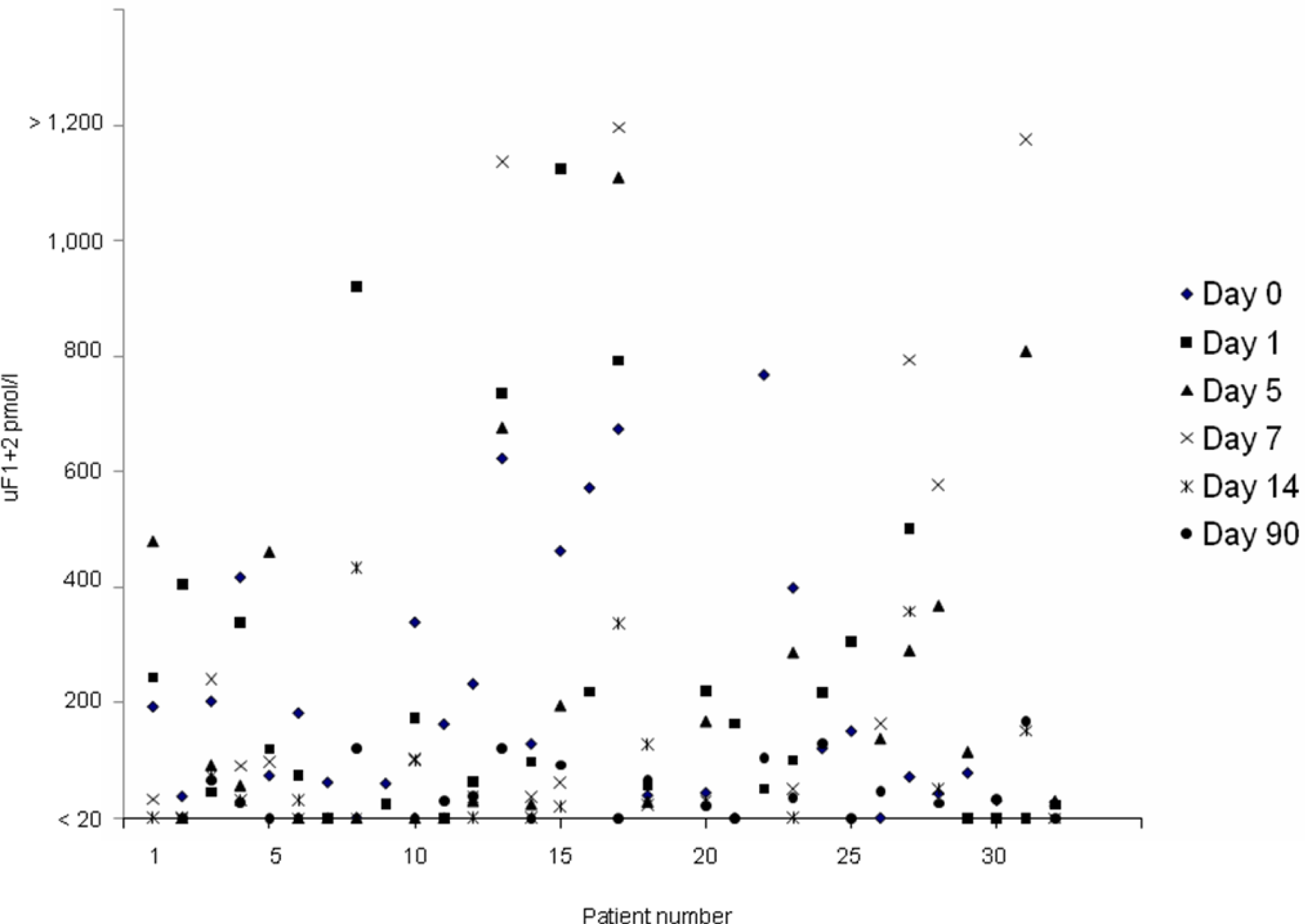
Scatter plot of all data points in the study (N = 31). Patient no 19 was excluded before urine collection (see text).
There was a tendency toward higher median uF1 + 2 levels on all days in patients treated with hemiarthroplasty versus patients treated with osteosynthesis. However, the differences seen were not statistically significant on any day (Table 1).When a comparison was made between these 2 groups on the day of admission and the day after operation (day 1), the relative increase in uF1 + 2 excretion was 57% after hemiarthroplasty (from 154.2 to 242.5 pmol/L) versus 25 % after osteosynthesis (from 134.5 to 168.2 pmol/L). Furthermore, the relative decrease in uF1 + 2 was more pronounced on days 5 and 7 in patients treated with osteosynthesis compared with patients treated with a hemiarthroplasty.
Two patients died during the study on days 51 (patient no 16) and 33 (patient no 9), respectively, after admission. Autopsy was not performed. The causes of death were presumed to be atrial fibrillation and lung infection in one and metastases to the liver from an occult malignant tumour in the other. Two patients experienced vascular thrombotic complications. One was a woman of 88 years who had an acute myocardial infarction 2 days after admission and was treated with a pacemaker (patient no 3). The other was a woman of 80 years, readmitted to the hospital 61 days after surgery, with collapse and angina pectoris treated with nitroglycerin (patient no 11). The median uF1 + 2 levels in patients with and without a vascular thrombotic event or death are shown in Table 1. There was a trend toward higher levels on the day of hospital admission in patients with events compared with patients without events, 184.6 pmol/L versus 144.4 pmol/L (P = .65).
Discussion
In this exploratory pilot study, we found a substantial elevation of uF1 + 2 levels in elderly patients with HF at hospital admission and even higher levels on the days following operation. Although it was a small study, there was a trend toward higher uF1 + 2 levels in patients with vascular thrombotic events and death compared with patients without such events.
For obvious reasons, we cannot show the pre-fracture level of uF1 + 2 in the actual patient population, however, we assume that it was close to the median level at follow-up 30.3 pmol/L or lower. We base this on the assumption that a 3-month period should be sufficient to reestablish the normal hemostatic activity after a fracture. In addition, when we compare with previous studies in which we have followed the uF1 + 2 excretion in patients with THA and TKA, the median uF1 + 2 level before the operative procedure was <20 pmol/L using the same ELISA method for measurement of uF1 + 2 as in the current study.4,5 Based on these arguments, the significantly elevated uF1 + 2 level seen at hospital admission in patients with HF, compared with the level at follow-up, can be explained by the increased hemostatic activity induced by the fracture and the further increase seen on the day after operation (day 1) is a result of the additive activating effect of the operative trauma. When these results were stratified according to the type of operative procedure, the higher relative increase in the median uF1 + 2 level from the level at admission to the level on day 1 in patients treated with a hemiarthroplasty compared with the relative increase seen in patients treated with osteosynthesis indicates a more intense coagulation activity after a hemiarthroplasty. The increased intensity may be explained by the longer duration of the operative procedure and the use of cement. This interpretation is further substantiated by our finding of a more pronounced relative decrease in uF1 + 2 on days 5 and 7 in the osteosynthesis group.
When we continue to compare with previous findings, patients with HF had a higher median uF1 + 2 level at hospital admission than patients having THA with objectively verified VTE events 3 days after the operation. 4 Furthermore, the median level of uF1 + 2 on the day after surgery in patients with HF exceeded the level on the day after surgery in patients having TKA with VTE events. 5 This indicates that the coagulation activity in elderly patients with HF is substantial from the first day they present at the hospital and may explain the high rate of VTE events in these patients. 1 The uF1 + 2 levels seen in patients with vascular events/death in the current study exceeded our previously defined cutoff of 50 pmol/L for detection of significant coagulation activity, indicating that this might also be used in patients with HF.3,4 Despite the relatively small patient population in this study, we saw marked individual variations in the uF1 + 2 excretion on all days. This underlines that individual differences may play an important role and could indicate the need for individualized antithrombotic treatment. Based on the findings in this study, it may be possible to monitor coagulation activity in the individual patient by measuring uF1 + 2 to help the clinician making more qualified treatment decisions.
Hypercoagulability after HF has been reported in studies using thrombelastography (TEG). A study by Wilson et al 7 showed significant hypercoagulability after surgery in patients with HF persisting for at least 6 weeks, and it correlated with development of DVT. In another study, a rapid TEG (r-TEG) technology was used to predict symptomatic thrombotic events (venous and arterial) in a group of critically ill patients who had undergone surgery for head-, spinal cord-, and pelvic injuries. 8 Our study is the first that has been able to differentiate between the coagulation response caused by the fracture itself and the additive effect of the operative trauma.
We cannot draw any firm conclusions based on this small study, but it demonstrated that elderly patients with HF have a substantial coagulation activity (high median levels of uF1 + 2) at hospital admission and during the first week after operation. To confirm these findings, we have started a large-scale cohort study in patients with HF at our department using the same methodology.
Footnotes
This work was presented orally at the annual meeting of the Danish Orthopaedic Society in Copenhagen on October 23, 2009
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.