
Abstract
Reports of intracerebral hemorrhage (ICH) in patients with hemophilia B are relatively rare. We describe the first clinical results of the use of a monoclonal antibody purified factor IX (FIX) concentrate (Mononine) after an ICH and the long-term outcome of prophylaxis with this product to prevent recurrences. A 44-year-old male with severe hemophilia B was referred to our department because of nausea, vomiting, left lower limb hemiplegia, and left arm paresis. Computed tomography (CT) revealed a right frontal intraparenchymal bleed. The patient was treated with replacement therapy with FIX for 40 days. Computed tomography scans performed on day 40 after the event showed complete disappearance of the cerebral hematoma from the parenchymal tissue. Subsequently, the patient received 25.6 IU/kg-1 of FIX twice a week. At the 48-month follow-up visit, no more major or minor bleeding events had occurred. Long-term prophylaxis after ICH is recommended.
Introduction
Intracerebral hemorrhage (ICH) is one of the most severe bleeding events that can occur in patients with hemophilia. It is associated with a high mortality rate and with a relevant number of disabling sequelae. Although this complication may occur at any age, it is particularly common in the newborn (3.5%-4% of neonates with hemophilia). Recurrences in the same patients are frequent. 1 –4 No differences have been found between hemophilia A and B. Because of the low frequency of the disease, reports of ICH in patients with hemophilia B are rare. 5 There are insufficient data in the literature regarding patients older than 50 and only limited information on the acute phase treatment of ICH in patients with hemophilia. Furthermore, no data on long-term therapy to prevent recurrences following a first ICH have yet been published.
The role of prophylaxis in preventing or avoiding the progression of hemophilic arthropathy has been well established. 6,7 A distinction can be made between primary and secondary prophylaxis depending on when the prophylaxis is started. 7 The benefits of the latter strategy, in terms of reducing the annual rate of bleeding events and improving quality of life, were recently confirmed by a large survey in Italy, which included 84 adolescents and adults with severe hemophilia who were switched from on-demand treatment to prophylaxis. 8
Treatment recommendations or guidelines for the management of patients with hemophilia who have had an ICH are not available, nor is there evidence or consensus about the role of long-term prophylaxis with coagulation factor concentrates in preventing recurrences. Mononine (CSL Behring, Marburg, Germany) is a monoclonal antibody-purified factor IX (FIX) concentrate; several published studies have determined the pharmacokinetic properties of this concentrate and its efficacy, administered by bolus injection or continuous infusion, in the treatment of acute bleeding episodes and in the prevention of bleeding in surgical settings. 9 –11 To our knowledge, no reports have been published yet on the efficacy of Mononine in the acute phase treatment of ICH and in the long-term follow-up.
Case Report
We report the case of a patient with intraparenchymal hemorrhage managed with a monoclonal antibody-purified FIX concentrate (Mononine). The drug was used in the acute phase and subsequently as long-term prophylaxis to prevent ICH recurrence.
The patient was a 44-year-old male with severe hemophilia B (FIX < 1%), which was diagnosed within the first year of life following investigations to determine the cause of a hematoma that developed at a puncture site. His bleeds were initially managed with plasma, subsequently with low-purity plasma-derived FIX concentrates and then, starting from July 2003, with the monoclonal antibody-purified FIX. The patient received a mean of 48 000 IU/year of Mononine on demand to treat an average number of 20 bleeding events, including 12 joint bleeds. Before arriving at our institution, the patient had undergone several surgical procedures at different sites during his infancy and adolescence: synovectomy of both knees, both ankles, and the right elbow, left ankle tendon surgery, correction of phimosis, and posttraumatic right femur fixation. The patient had been infected, via transfusions, with hepatitis B virus, human immunodeficiency virus (HIV), and hepatitis C virus (HCV), with serological positivity being recorded at the age of 17, 24, and 29 years, respectively. The HIV infection had been managed by several antiretroviral regimens and, at the time of the ICH, the patient was being treated with a highly active antiretroviral therapy (HAART) protocol, including efavirenz/didanosine/lopinavir plus ritonavir, which maintained a CD4 count >500/mm3 and an HIV viral load <50 copies/mL. The HCV infection has not been treated yet. In 1995, the patient developed hypertension, which is being treated with a combination of a diuretic and a β-blocker.
On the day the ICH occurred, the patient woke up in the morning complaining of left arm paresthesia and an unstable gait. The previous night he had been nauseous and had vomited. He arrived at the Emergency Department in the afternoon, with left lower limb hemiplegia and paresis of the left arm. He was immediately given an infusion of 2000 IU of Mononine. Computed tomography (CT) revealed a right frontal intraparenchymal bleed, surrounded by a faint halo of edema. On neurological examination, the patient’s level of consciousness was normal, but he had left lower limb paraplegia and left arm paresis. His blood pressure was 170/105 mm Hg and his platelet count was in the normal range. In the following hours, the patient developed a series of seizures, controlled by diazepam and diphenylhydantoin in addition to the anti-edema cerebral therapy. Blood pressure was first lowered by labetalol and clonidine and later by adding a diuretic and a calcium-channel blocker. Subsequent CT scans, performed 12 and 24 hours later, did not show any changes.
The replacement therapy with FIX consisted of bolus injections of 4000 IU (55.5 IU/kg-1 over 24 hours) in the first 4 days, reduced to 3000 IU (41.6 UI/kg-1) until day 11, and then 2000 IU (27.7 UI/kg-1) until day 40. In the first 4 days, FIX levels, evaluated daily, ranged between 50% and 60% (n.v. 60%-160%) and the partial thromboplastin time (PTT) was normal. FIX levels were maintained in the range of 40% to 50% with the PTT value higher than normal during the following 7 days and in the 30% to 40% interval with a slight increase of PTT from day 12 to day 30. No further seizures occurred from day 6.
Blood pressure was controlled only by a combination of a diuretic and a β-blocker from day 30. The patient underwent active and passive physical therapy, with progressive improvement of movements, starting with left arm function. From day 20, we observed recovery of left limb function, so that the patient was able to remain in the upright position and walk with aids after day 25.
We further studied the cerebral status by angiographic magnetic resonance imaging (MRI), which excluded vascular malformations. A series of CT scans, performed every 48 hours during the first week and once a week thereafter, showed 50% reabsorption of the hemorrhagic mass by day 20 and complete disappearance of the cerebral hematoma from the parenchymal tissue by day 40 (Figure 1 ). Computerized tomography scans, performed 3 and 6 months after the ICH, and MRI, performed after 12 months, were normal.
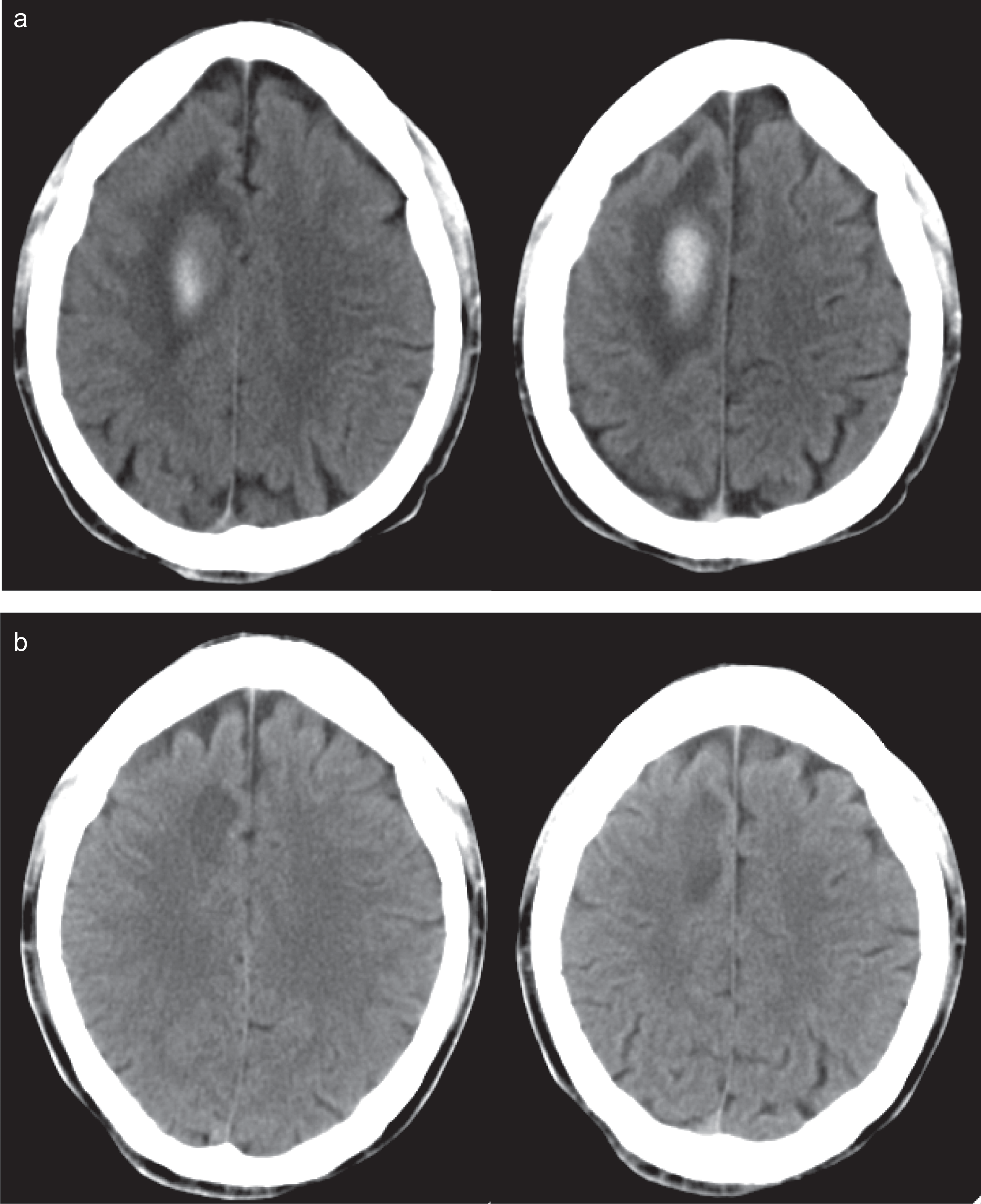
Computerized tomography (CT) scans of an acute frontal parasagittal intraparenchymal hematoma (a) in a human immunodeficiency virus (HIV)-positive patient with severe hemophilia B. Computerized tomography scans performed after 40 days: the hematoma has been reabsorbed, leaving only a faint residual hypodense area at the site of the bleed (b).
From day 40, the patient received 2000 IU of Mononine (25.6 IU/kg-1) twice a week. At the 48-month follow-up visit, the patient completely adhered to this long-term prophylaxis regimen, and no more major or minor bleeding events had occurred and no extra infusions of FIX had been required. The number of working days lost due to hemophilia had decreased from 35/year to 0/year.
The neurological examination did not show any sequelae of the bleeding event, with full upper and lower limb function. Blood pressure was well controlled by a β-blocker. Figure 2 shows FIX plasma levels measured after the administration of Mononine 25 IU/kg. Notably, the concentration of FIX reached a maximum (ie, 26.1 IU/dL) after 15 minutes and was still 4 IU/dL after 72 hours.
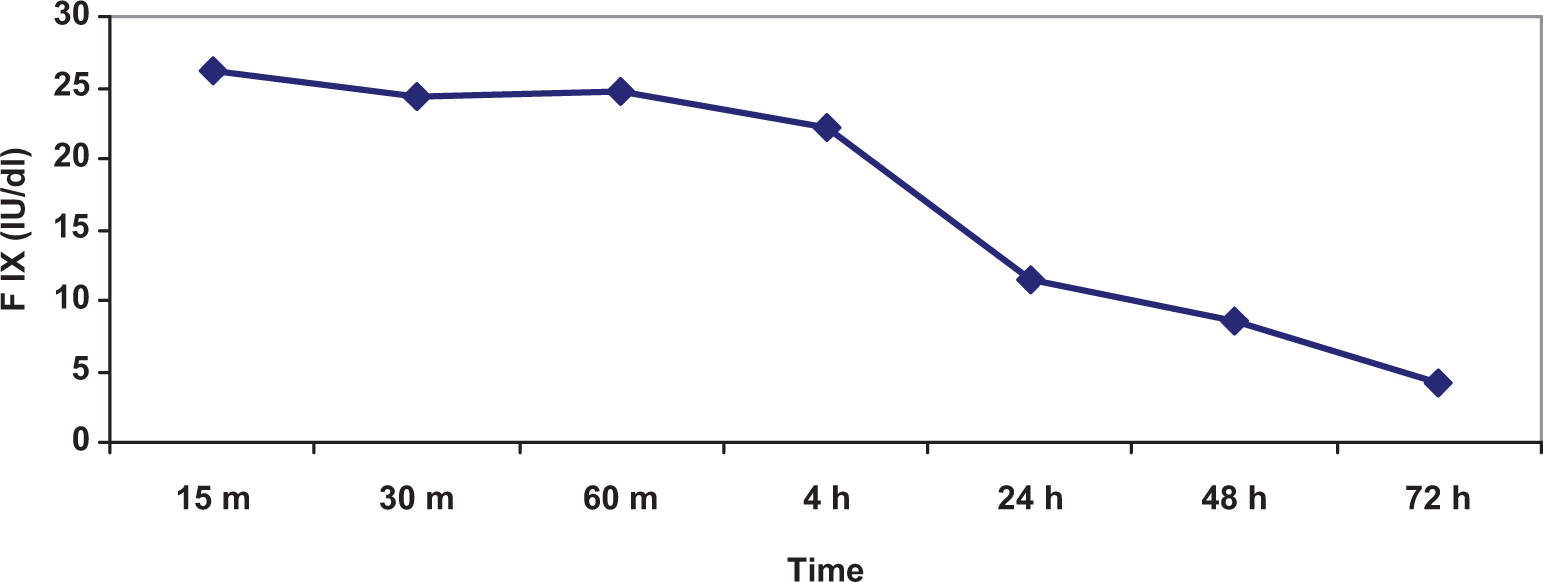
Plasma concentration-time curve of factor IX following the first administration of Mononine (25.6 UI/kg-1). X axis: Factor IX level (IU/dL); y axis: Time (m = minutes, h = hours).
Discussion
We describe the first clinical results on the short-term use of a monoclonal antibody purified FIX concentrate (Mononine) for the immediate management of an ICH and the long-term outcome of prophylaxis with the same concentrate for the prevention of recurrences. Our protocol for the treatment of the acute ICH episode was highly effective, resulting in total reabsorption of the subdural hematoma and, over time, complete physical recovery without any neurological deficit.
Following the acute phase, the patient received long-term prophylaxis with Mononine at slightly lower dosages than usually recommended (25 IU/kg vs 30-40 IU/kg). The FIX plasma concentration-time curve (Figure 2) revealed that after a 1-day wash-out, a bolus injection of the daily dose of Mononine (2,000 IU) was able to maintain FIX plasma levels around 5% after 72 hours. This result may explain the efficacy of the adopted prophylaxis regimen in ensuring a long period free of bleeding episodes. Indeed, during the prophylaxis, the patient did not suffer any bleeding episodes and had a marked improvement in his quality of life, reflected by the fact that he did not miss any days from work due to hemophilia (35 days/year before prophylaxis) and had no limitations to daily activities.
Currently, there are no definitive guidelines on treatment following a first ICH in patients with severe hemophilia. After the acute phase, patients usually return to the regimen they were receiving prior to the ICH (which is, in most cases, on-demand treatment), and only in around one third of cases are they switched to long-term prophylaxis. 12 Our case report shows that careful management of a patient with hemophilia who has had an ICH, with institution of long-term secondary prophylaxis, can lead to a favorable outcome, with resolution of acute symptoms and sequelae as well as prevention of recurrent ICH.
Footnotes
Acknowledgment
Dr. Rachel Stenner for the revision of the manuscript.
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.