
Abstract
Hematologic abnormalities of mild anemia and leucopenia have been frequently associated with acute brucellosis, but thrombocytopenia are less frequently seen. In the present study, we documented 5 (2.6%) isolated thrombocytopenic patients with the manifestations of brucellosis observed during the course of active infection. Five (2.6%) patients, 4 boys and 1 girl, with ages ranging from 2 to 14 years, had isolated thrombocytopenic at diagnosis. In 5 (2.6%) patients, platelet counts ranged from 39 000 to 120 000/mm3. Tube agglutination tests for brucellosis were positive for all patients (1/160-1/1280). All patients recovered completely, and their thrombocytopenia returned to normal by 2 to 4 weeks after antibiotic treatment of brucellosis. In our study, we present 5 patients with Brucella-induced thrombocytopenia mimicking idiopathic thrombocytopenic purpura to emphasize the isolated thrombocytopenia and the resolution of thrombocyte counts following treatment of brucellosis.
Keywords
Introduction
Brucellosis remains an important public health problem in Turkey and it can affect people at any age, including children, representing 20% to 25% of cases. 1
Brucellosis is a multisystem disease with a broad spectrum of clinical manifestations. Hematologic abnormalities of mild anemia and leucopenia have been frequently associated with acute brucellosis, but thrombocytopenia are less frequently seen.2 –5 As mentioned above, thrombocytopenia during the clinical course of brucellosis is not common, with an incidence varying from 1% to 8% in adults.2,6 Thrombocytopenia is usually moderate and attributed to bone marrow suppression or hypersplenism.6,7 In our study, we present 5 patients with Brucella-induced thrombocytopenia mimicking idiopathic thrombocytopenic purpura (ITP) to emphasize the isolated thrombocytopenia and the resolution of thrombocyte counts following treatment of brucellosis.
Cases and Results
Records of children younger than or equal to 16 years and admitted to the Yuzuncu Yil University Hospital between 2004 and 2010 were analyzed retrospectively. Patients who were known to have any acute or chronic systemic disease other than brucellosis were excluded. In addition to history and physical examination, all children had a complete blood count and Brucella serology. Over this time period, 187 patients who had been referred to our hospital were diagnosed as brucellosis. In the current study, we documented 5 (2.6%) patients with isolated thrombocytopenia having the manifestations of brucellosis observed during the course of active infection. The diagnosis of brucellosis was made because of a clinical picture compatible with the disease, together with Brucella agglutination titers of at least 1:160. Leukocyte and differential counts and hemoglobin levels were considered abnormal according to the established reference values in infancy and childhood. 8 Thrombocytopenia was defined as a platelet count of less than 150.000 /mm3. Bone marrow aspirations were carried out in 3 patients for the differential diagnosis of thrombocytopenia. For treatment of brucellosis, the preferred antibiotic regimen consisted of a combination of doxycycline and rifampicin or cotrimoxazole and rifampicin for 6 to 8 weeks. Doxycycline was administered only in children older than 8 years. Follow-up was carried out according to individual response.
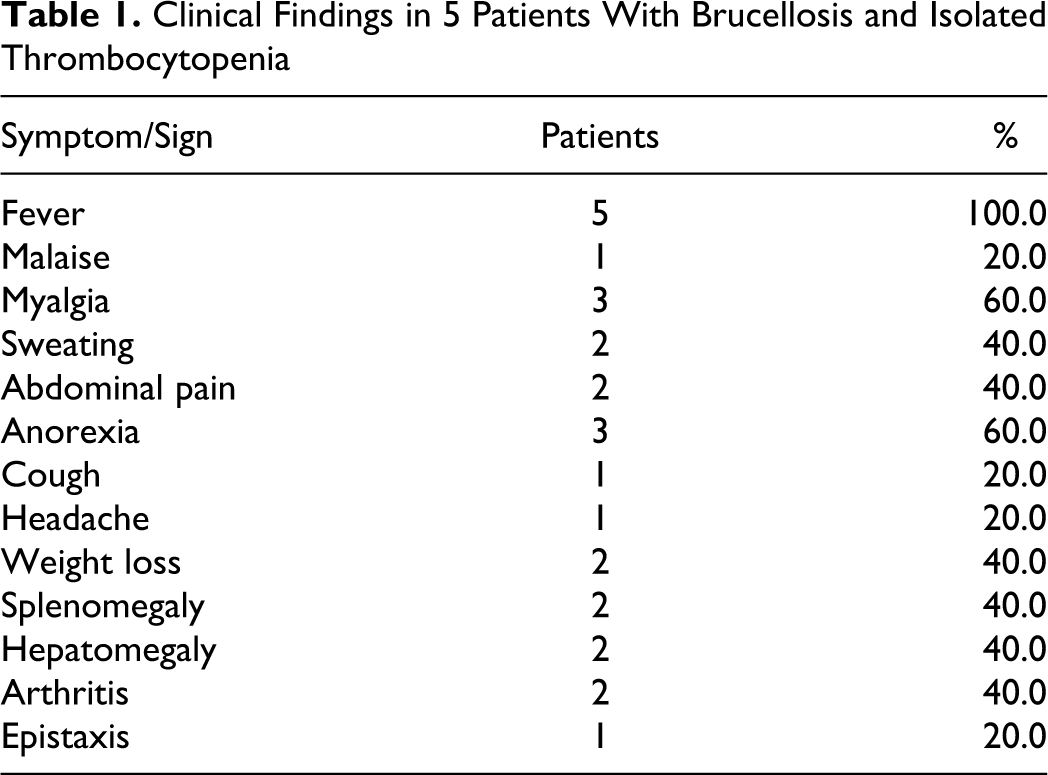
Five (2.6%) patients, 4 boys and 1 girl, with ages ranging from 2 to 14 years, had isolated thrombocytopenia at diagnosis. All patients had recently consumed unpasteurized homemade dairy products or had contact with sheep and cows. Fever was present in all. Clinical findings of the patients are given in Table 1. The patients including splenomegaly in 2, hepatomegaly in 2, arthritis in 2, headache in 1, epistaxis in 1, and abdominal pain in 2. Initial laboratory findings of the patients are given in Table 2. In 5 (2.6%) patients, platelet counts ranged from 39 000 to 120 000/mm3. The routine coagulation tests were normal. Serological tests for hepatitis B surface antigen (HBsAg), anti-hepatitis C virus (anti-HCV), HIV, parvovirus, rubella, cytomegalovirus, and Ebstein-Barr virus all were unremarkable. Tube agglutination tests for brucellosis were positive for all patients (1/160–1/1280). Bone marrow aspiration showed normal cell proliferation and maturation in 3 patients. An increased number of megakaryocytes were seen in 2 of 3 patients; only in remaining patient, megakaryocytes’ count was normal. All patients recovered completely, and their peripheral blood counts returned to normal by 2 to 4 weeks after antibiotic treatment of brucellosis. None of the patients were given corticosteroid or intravenous immune globulin (IVIG) treatment.
Clinical Findings in 5 Patients With Brucellosis and Isolated Thrombocytopenia
Results of Initial Peripheral Blood Cell Count and Some Laboratory Manifestations in 5 Patients With Brucellosis and Isolated Thrombocytopenia
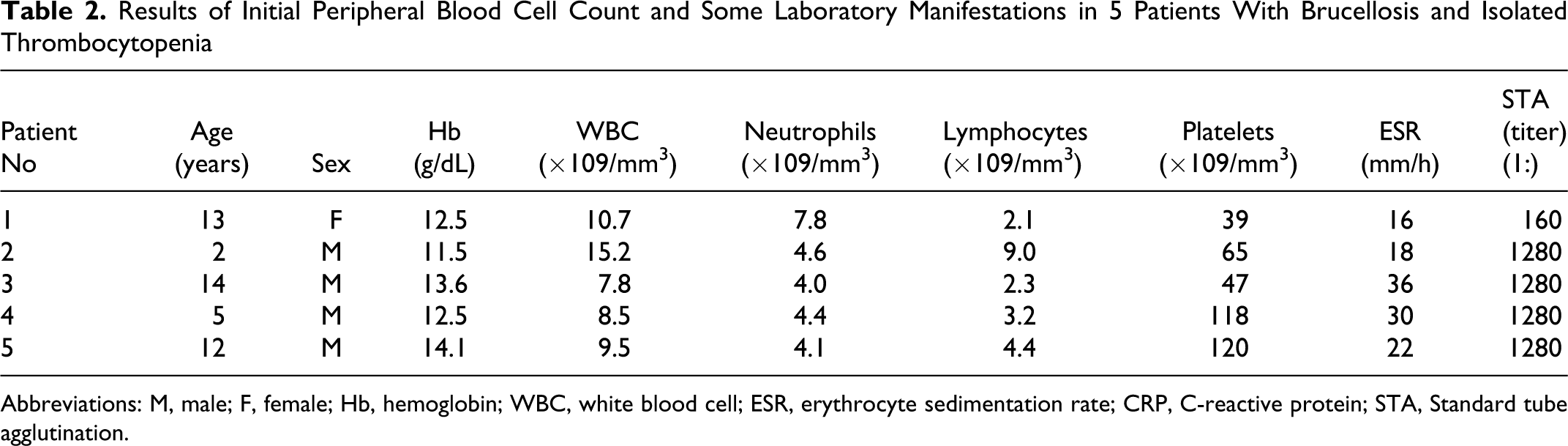
Abbreviations: M, male; F, female; Hb, hemoglobin; WBC, white blood cell; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; STA, Standard tube agglutination.
Discussion
Brucellosis constitutes a major health problem in our region. It is a multisystem disease with a broad spectrum of clinical manifestations. The symptoms are nonspecific; however, the majority complains of fever, sweats, malaise, anorexia, headache, arthralgia, and backache.
Few data on the frequency and diversity of hematologic abnormalities occurring in brucellosis have been reported in children.3–5 Hematological abnormalities ranged from fulminant as of disseminated intravascular coagulation to anemia, leucopoenia, thrombocytopenia, and clotting disorders. 6 The most commonly observed hematologic abnormalities associated with brucella infection are mild anemia and leucopenia. 9 Thrombocytopenia is reported in 1% to 26% of cases and rarely causes bleeding.5,10–12 Isolated thrombocytopenia (platelets < 150 × 109/mm3) was seen in 8% of cases in a study reported from our region. 2 In our study, 5 (2.6%) patients with isolated thrombocytopenia having the manifestations of brucellosis observed during the course of active infection. This result is in accordance with previous reports. Severe thrombocytopenia is extremely rare.13,14 In our study, severe thrombocytopenia was not found. Hemorrhages have been reported in 3% to 19% of patients with brucellosis, which is more frequently associated with B. melitensis than with other Brucella species. In our study, in 1 patient epistaxis was found.
The mechanism responsible for thrombocytopenia in brucellosis is not certainly understood but is probably multifactorial, including hypersplenism, disseminated intravascular coagulation, bone marrow suppression, hemophagocytosis, and immune destruction of platelets. 15 Antiplatelet antibodies may cause peripheral immune destruction of platelets but it is difficult to detect these antibodies with the usual tests in Brucella-induced thrombocytopenia. A negative assay for antiplatelet antibodies does not exclude the diagnosis of immune thrombocytopenia.12,16 The mechanisms of thrombocytopenia in our patients were possibly related to brucellosis-induced thrombocyte destruction by antibodies against Brucella species cross reacting with thrombocytes, mimicking ITP, as an examination of bone marrow aspiration revealed increment of megakaryocytes in 2 patients, a finding which may also be seen in ITP. It is well documented that appropriate antimicrobial therapy improves the clinical and hematologic status of patients with brucellosis. Platelet recovery usually occurs within 2 to 3 weeks of initiation of appropriate antimicrobial therapy. 9 In our study, all patients recovered completely, and their platelet counts returned to normal by 2 to 4 weeks after antibiotic treatment of brucellosis.
In conclusion, brucellosis should be considered a possible diagnosis among patients with fever and isolated thrombocytopenia, especially in geographic regions where brucellosis is endemic. Thrombocytopenia, like other hematologic complications of brucellosis, is generally mild and resolves promptly with treatment of the disease.
Footnotes
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.