
Abstract
In the current study, clinical and laboratory findings and treatment modalities of children with acute and chronic immune thrombocytopenic purpura (ITP) were evaluated retrospectively. Our purpose was to determine clinical outcome of children with ITP and their responses to different treatment regimes. Total of 260 children with ITP were enrolled in the study. The mean age of patients was 76.8 ± 48.1 months. The therapy responses of high-dose methylprednisolone (HDMP; n = 134), standard dose methylprednisolone (n = 32), and intravenous immunoglobulin (IVIG; n = 15) treatments were similar. Two (0.8%) of the 260 ITP patients had intracranial bleeding. None of the patients died due to hemorrhage. Of all the patients with ITP, 191 (73.5%) completely resolved within 6 months after initiation of the disease and therefore they were diagnosed as acute ITP; 69 patients (26.5%) had progressed into chronic ITP. The therapy responses of HDMP, standard dose methylprednisolone, and IVIG treatments are similar.
Introduction
Immune thrombocytopenic purpura (ITP) is a common, acquired bleeding disorder in childhood period. It may follow a viral infection or immunization and is caused by an inappropriate response of the immune system. 1 The disease is characterized by thrombocytopenia, shortened platelet survival, the presence of antiplatelet antibodies in plasma, and normal or increased number of megakaryocytes in bone marrow. 2 Immune thrombocytopenic purpura mostly appears as extensive cutaneous bleeding, such as petechia, purpura, and ecchymosis in an otherwise healthy child, and it has usually short duration and good prognosis.3,4 The course of ITP may be acute, chronic, or recurrent. 5 In acute ITP, platelet count returns to normal values within 6 months after diagnosis (more than 150 000/mm3) and relapse does not occur. 6 In chronic ITP, decreased platelet number remains after 6 months. 6 In the recurrent forms, platelet count decreases after having returned to normal levels. 6 The disease resolves in 60% to 80% of the patients in weeks or months, however about 10% to 30% of cases fail to remit over 6 months and therefore become chronic.7–9
In the current study, clinical and laboratory findings and treatment modalities of children with acute and chronic ITP were evaluated retrospectively. Our purpose was to determine clinical outcome of children with ITP and their responses to different treatment regimes.
Patients and Methods
A total of 260 patients diagnosed as ITP between 1995 and 2009 in the Department of Pediatric Hematology, Faculty of Medicine, Yuzuncu Yil University, were retrospectively evaluated. The age, gender, presenting complaint, platelet count at diagnosis, treatments applied, treatment response, seasonal preponderance, previous infection, and immunization history of the patients were recorded. The diagnosis of acute ITP was made based on the history, physical examination, and laboratory analysis, including a complete blood count revealing isolated thrombocytopenia (platelet count <150 000/mm3), normal hemoglobin, white blood cell count, absence of atypical lymphocyte or blast on peripheral blood smear examination, and absence of underlying conditions or malignancy. 6 Chronic ITP was defined as persistent thrombocytopenia with or without continued therapy for 6 months following initial diagnosis. 6 Bone marrow aspiration was performed in patients with acute ITP who were thought to be treated with corticosteroids. The diagnosis was confirmed in patients with all chronic ITP before the initiation of treatment. If a child had an immunization or viral infection history within a month before the onset of ITP, it was accepted as the causing factor. The patients were categorized as complete remission (CR), when the platelet count was ≥150 000/mm3; partial remission (PR), platelet count ranging from 50 000/mm3 to 150 000/mm3; minimal remission (MR), platelet count ranging from 30 000/mm3 to 50 000/mm3; and no response (NR), platelet count >30 000/mm3. 10 In our center, treatment regimes for ITP included intravenous high-dose methylprednisolone ([HDMP] 30 mg/kg per d for 3 days and 20 mg/kg per d for 4 days), oral steroids with standard dose (2 mg/kg per d for 14 days), intravenous immunoglobulin ([IVIG] 1 g/kg per d for 2 days), intravenous anti-D immunoglobulin (50 μg/kg per d for 6 days), and rituximab (375 mg/m2 per week for 4-6 weeks). Splenectomy was generally performed in patients with chronic ITP who were older than 5 years old, having frequent bleeding episodes, whose platelet counts were <10 000/mm3 and whose symptoms were refractory to pharmacologic management. All patients received pneumococcal and Haemophilus influenzae immunizations prior to surgery. Supportive measurements including restricted physical activity, avoiding head or abdominal trauma, and lining the bed using protective padding in bed were recommended to patients with ITP.
Statistical analyses were performed using the commercial SPSS 14 packet program. Conformity of continuous variables to normal distribution was assessed using the 1-sample Kolmogrov-Simirnov test. For descriptive statistics, the mean was used for the variables with normal distribution, and the median was used for the variables without normal distribution. Parameters with normal distribution were compared using the variance analysis. Following variance analysis, the Duncan test was used to find the difference between the groups. The chi-square tests were used to determine the relationship between categorical variables and Z tests to compare the ratios. Level of significance was set as P < .05.
Results
Of the 260 children, 134 (51.5%) were males and 126 (48.5%) were females. Mean age of the patients was 76.8 ± 48.1 months. The majority (61.9%) of children was aged 2 to 10 years. Presenting platelet count was between 200 and 86 000/mm3 (14 200/mm3 ± 16 220/mm3). Most cases (77.6%) presented with a very low platelet count (<20 000/mm3). The most common presenting symptoms were petechiae and/or purpura, epistaxis, and gingival bleeding.
Clinical and laboratory findings of patients with acute or chronic ITP were shown in Table 1. 69 (26.5 %) of the 260 patients had persistent disease for more than 6 months and are thus defined as having chronic ITP. The other 191 patients (73.5%) completely resolved their disease within 6 months and met the criteria for acute ITP. The male/female ratio of children with acute and chronic ITP was not statistically significant (P > .05). Children with chronic ITP presented at older age than children with acute ITP. The mean age (SD) at presentation for acute patients was 75 (48.6) months and 81.8 (46.9) months for chronic patients, without significant difference between the groups. The highest proportion of children with ITP was aged 2 to 10 years. A history of preceding viral infection, subsequently resolved, was significantly more common in acute than in chronic ITP (P < .05). A history of preceding viral infection was noted in 36.6% and 36.2% of children with acute ITP and chronic ITP, respectively. Majority of cases was diagnosed in summer season. No significant difference (P > .05) was found in patients with regard to seasonal changes. A vaccination history was noted in 4 patients (1.5%) with acute ITP. Three patients with measles and another with diphtheria-pertussis-tetanus (DPT). No recurrence or chronicity was noted in these patients. A history of honeybee and insect bite was noted in 2 patients. Additionally, recurrence or chronicity was not noted in these patients. Presenting platelet count was between 200 and 86 000/mm3 (14 200/mm3 ± 16 220/mm3). Most cases (77.6%) presented with a very low platelet count (<20 000/mm3). The mean presenting platelet count for acute ITP was slightly higher 14 202/mm3 than that for chronic ITP 14 144/mm3. However, there was no significant difference between acute and chronic cases (P > .05). The most common presenting symptoms were petechiae and/or purpura (61.5%), epistaxis (38.4%), and gingival bleeding (19.6%). The ratio of this symptoms in the children with acute or chronic ITP was not statistically significant (P > .05). Bone marrow aspiration was performed as part of the initial diagnostic evaluation in 228 cases (87.6%).
Clinical and Laboratory Findings of The Patients with Acute and Chronic ITP
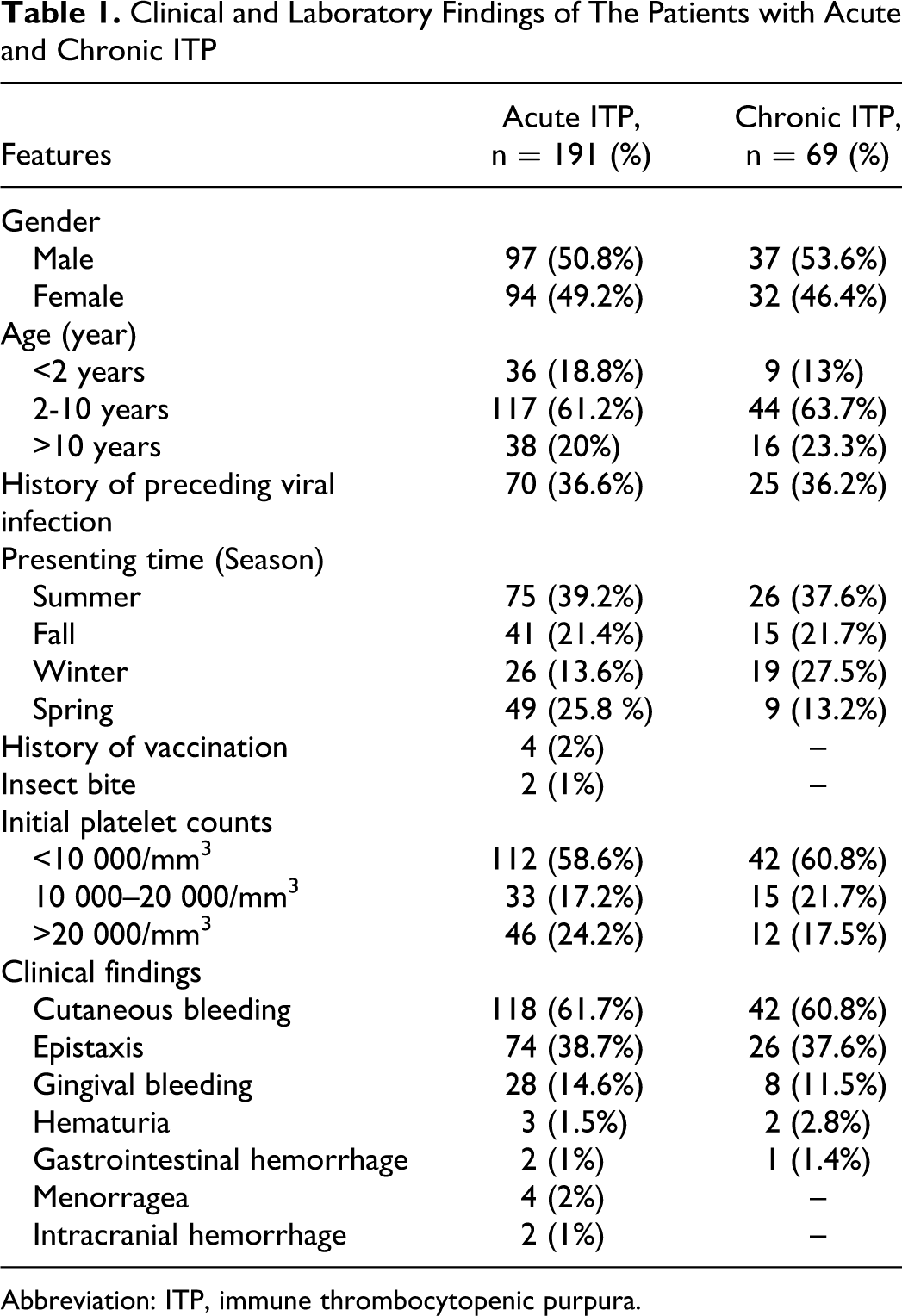
Abbreviation: ITP, immune thrombocytopenic purpura.
Intracranial bleeding, the most severe complication of ITP, was seen in 2 patients (0.8%); in one of them in whom the platelet count was 4000/mm3, HDMP treatment was administered. On the second day of the treatment, she had headache and vomiting and her cranial computerized tomography (CT) revealed subarachnoid hemorrhage. Intravenous immunoglobulin was added to the regimen and thrombocyte suspension was given. The patient was followed up without any neurological sequel. Other patient was admitted to our hospital with headache, vomiting, bleeding from nose, and bruises on the extremities; her platelet count was 4000/mm3. Cranial CT revealed hyperdense areas in the right occipital regions and bilateral basal ganglia, which consisted of hemorrhage. Thrombocyte, HDMP, and IVIG suspension were given. The patient was followed up without any neurological sequel.
Therapy was given to 247 (95%) of 260 patients. In 13 patients (5%), observation alone was the only clinical option. The most frequently used drug was HDMP in both groups. In all, 180 patients with acute ITP were treated with HDMP and 145 showed a response (80%). A total of 32 patients with acute ITP were treated with standard dose methylprednisolone, and 25 showed a response (78.1%). Intravenous immunoglobulin was used as treatment in 20 patients with acute ITP, with 16 (80%) responding to that therapy. The combined results for IVIG plus HDMP were 9 (81.8 %) responses in 11 patients with acute ITP. There was no statistically significant difference between any treatment groups in treatment−response ratio (P > .05). Furthermore, of the patients who had taken HDMP as first treatment, 145 had CR, 11 had PR, 3 had MR, 21 had NR. Chronicity rate was found higher in patients with NR or PR to HDMP therapy than with CR (P < .05).
Of the 69 chronic ITP patients, 34 cases resolved between 7 and 112 months. Seven patients (10.1%) resolved between 6 and 12 months after presentation, 12 patients (17.4%) resolved between 12 and 24 months, and 15 patients (21.7 %) resolved between 25 and 112 months. A total of 325 therapy cure was given to patients with chronic ITP. Totally 143 cure of HDMP, 75 cure of standard dose steroid, 27 cure of IVIG, 44 cure of whin-ro, 20 cure of rituximab and 16 cure of IVIG plus steroid treatment protocols were given. When we compared the total therapy cures that were given to patients with chronic ITP, with regard to the success rate of CR to treatment, we found that patients given HDMP had higher CR rate than other patients who had taken standard dose steroid, IVIG plus steroid, IVIG, whin-ro, rituximab, and the patients who did not followany treatment; and this difference was statistically significant (P < .05). Of all the patients with chronic ITP, splenectomy was performed in 9 patients (3.4%). The mean time between diagnosis and splenectomy was 42.1 months (range: 6-85 months). A CR was noted in 6 (66.6%) of 9 patients after splenectomy.
The ratio of positive response to the initial treatment and chronicity, according to treatment modalities is shown in Table 2. There was no statistically significant (P > .05) difference between used treatment modalities for chronicity rate. We also did not find any statistically significant difference between used treatment modalities for positive response to the initial treatment (P > .05). Due to the low number of patients who had taken whin-ro, statistical evaluation could not be done.
Positive Response and Chronicity Ratios of Patients According to Treatment Modalities

Abbreviations: HDMP, high-dose methylprednisolone; MP, methylprednisolone; IVIG, intravenous immunoglobulin.
The overall response rate was 86.5% (225 of 260 patients with ITP). Of the 69 patients with chronic ITP, 35 (50.7%) did not respond to multiple combined treatment and splenectomy. Of these patients with chronic ITP, PR was achieved in 9 (13%) and MR in 1 (1.4%), but NR in 25 (36.2%).
Discussion
Immune thrombocytopenic purpura is a common pediatric hematologic disorder. It is an immune-mediated illness that results in thrombocytopenia due to platelet destruction from autoantibodies. 6
The most extensive study was reported by the Intercontinental Childhood ITP Study Group (ICIS). 11 In this international study, 2031 patients were registered at 136 facilities in 38 countries between June 1997 and May 2000, of which 1496 patients were followed up for >6 months. The male-to-female ratio was 1.2:1, and the mean age at diagnosis was 68.4 ± 49.2 months, without any difference in the average age between boys and girls. Our study revealed sex ratio was 1.03:1, and the mean age at diagnosis was 76.8 ± 48.1 years. The usual age of presentation is between 1 and 10 years, with peak incidence around 5 years of age. 12 Males and females seem equally affected. 12 However, male predominance has also been reported in children less than 2 years of age.13,14 In our study, majority of children (61.9%) with ITP were in 2 to 10 years age group. The mean age of presentation was 76.8 ± 48.1 months. We did not find gender predominance in children with ITP except for children younger than 2 years old, in which the male/female ratio was 1.8:1.
Acute ITP occurs most frequently in Spring or Winter, but similar seasonal variations in the chronic form have not been reported.6,11,13 However, Kalyoncu et al 14 found that most cases were diagnosed in summer in acute and chronic ITP. In this study, evaluation of the distribution of the patients according to the season of diagnosis showed a higher incidence, 38.8%, of ITP in the summer (n =101 of 260), in comparison with 17.3% (n = 45 of 260) in the winter, 21.6% (n = 56 of 260) in the fall, and 22.3% (n = 58 of 260) in the spring.
Vaccination-associated ITP has been reported in the literature, and it has been most often investigated in relation with measles, mumps, and rubella (MMR) vaccine. It was detected in 1 study that MMR vaccine increased the relative risk for ITP 6-fold and had a risk of 1 ITP case in a mean of 40 000 doses. 15 Moreover, ITP might also develop following DPT, poliovirus, Haemophilus influenzae, and hepatitis B vaccines. The course and treatment response in vaccination-associated cases are generally good. Immune thrombocytopenic purpura did not reoccur when these patients were vaccinated again with the same vaccines. 15 In our study, vaccination-associated acute ITP was noted in 4 patients with ITP.
In typical ITP, a normal child develops bruising and petechia over a short time period with no other serious symptoms of bleeding.4,16 Approximately 75% of patients have mild symptoms at their initial presentation of ITP, including the majority of children with platelet counts less than 10 000/mm3. 17 The mean initial platelet count in this study was 14 200/mm3, slightly lower than previous reports that ranged from 15 400/mm3 to 19 000/mm3.18,19 Although, petechiae and purpura are generally observed in most children with ITP, aproximately 20% of children develop other manifestations of bleeding such as epistaxis, melena, and menorrhagia.4,16 In our study, in 191 children with acute ITP, the most common presenting symptoms were petechiae and/or purpura (61.7%), epistaxis (38.7%), and gingival bleeding (14.6%). The other presenting symptoms were hematuria (n = 5), gross gastrointestinal system bleeding (n = 3), and menorrhagia (n = 4). In 69 children with chronic ITP, the most common presenting symptoms for chronic ITP were petechiae and/or purpura (60.8%), epistaxis (37.6%), and gingival bleeding (11.5%). The other presenting symptoms were hematuria (n = 2) and gross gastrointestinal system bleeding (n = 1).
The aim of therapy for ITP is the assumption that a rapid reversal of thrombocytopenia will minimize the risk of intracranial hemorrhage.20,21 Although children with acute ITP and platelet counts below 20 000/mm3 are at risk of life-threatening hemorrhage.22,23 Corticosteroids, IVIG, and anti-D immunoglobin may raise platelet counts in these patients.6,24–27 In life-threatening, excessive hemorrhage, and if necessary emergent splenectomy are recommended for the urgent therapy.11,27–29 Immunosupressive agents other than corticosteroids, splenectomy, anti-CD20 monoclonal antibody, and currently, thrombopoietin-like agents are among other therapeutic strategies in patients with chronic ITP.29,30 In the absence of data showing improved clinical outcome, treatment decisions are based on the assessment of the pediatrician and may show variations in different geographical groups. 11 In our center, we mostly preferred to use HDMP treatment because it is as efficient as IVIG and its cost is low.11,27,31 Watt 18 found that 256 patients were treated with steroid and 235 had a response (92%). In our study 212 patients were treated with steroids, and 160 (75.4%) had a response to initial therapy. Intravenous immunoglobulin was used as treatment in 20 patients, with 15 (75%) responding initially to that therapy. The combined results for steroid/IVIG were 6 (54.5%) responses in 11 patients treated. In our study group, initial treatment strategy did not show any significant difference in the treatment−response ratio (P > .05).
In our series, splenectomy was performed in 9 (3.4%) patients with chronic ITP. In a study from Argentina, splenectomy was performed in 79 (19.5%) of 404 children with chronic ITP; 55 (69.5%) of them achieved sustained normal platelet counts. 32 In a study from United Kingdom, 32 (48%) underwent splenectomy during a period from 1950 to 1980. However, only 5 (19%) children had a splenectomy from the period 1984 to 1994, in the same study. 33 Splenectomy was performed with decreasing frequency in the more recent case series. 24 After splenectomy, complete response was observed in 18 (75%) and 6 (50%) children reported by Vianelli et al 34 and Khalifa et al, 35 respectively. In our study, 66.6% children achieved CR response following splenectomy.
The outcome of children with ITP at 6 months seems not to be affected by initial treatment strategy. 36 Similarly, in our study group, initial treatment strategy most frequently, corticosteroid or IVIG, did not show any significant difference in progression to chronic ITP. The frequency of chronic ITP in children is between 25% and 31% in literature.11,18,37,38 The rate of chronicity was observed as 26.5% in our patients. Most children with typical ITP recover completely within a few weeks without treatment, and there is no proof that therapy prevents intracranial hemorrhage.16,25,36 Although the incidence of life-threatening hemorrhage is very low, there is a risk of mortality in patients with severe thrombocytopenia and with major bleeding manifestations. Intracranial hemorrhage, which may be seen in about 0.1% to1% of children with ITP and which is the most feared complication, occurred in 2 patients (0.8%) in our study.39,40 Consistent with the previous studies, none of our patients died.3,27,39 Our data reconfirm that ITP is usually a benign and self-limiting disease. Since the condition is often self-limiting and the risk of life-threatening hemorrhage is rare, the initial treatment of children with ITP remains controversial. Our results demonstrate 86.5% response rates with all of the common therapies.
In conclusion, the prognosis of childhood ITP is good. Although major bleeding developed in some of our patients, none resulted in death. The therapy responses of corticosteroid and IVIG treatments were similar and initial treatment strategy, corticosteroid or IVIG, did not show any significant difference in treatment−response ratio. Steroid provides a cheaper alternative to IVIG in countries that are not self-sufficient in blood products.
Footnotes
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.