
Abstract
Essential thrombocythemia (ET) can cause systemic vascular thrombosis but rarely cause obstruction of coronary arteries or acute myocardial infarction (MI). Treatment of acute MI in patients with ET may be a problem due to the important role of platelets in the pathogenesis of infarction. In this report, a 63-year-old man presented with acute chest pain and a greatly increased platelet count. The patient was successfully treated with intravenous tirofiban, a glycoprotein IIb/IIIa receptor blocker. Essential thrombocythemia was diagnosed based on bone marrow findings, clinical presentation, and laboratory analysis. Thrombocythemia had been controlled with hydroxyurea.
Introduction
Essential thrombocythemia (ET) is a myeloproliferative disorder of unknown etiology involving a multipotent hematopoietic progenitor cell and manifested clinically by overproduction of platelets without a definable cause. 1 It is an uncommon disease, with an incidence of approximately 7 per million per year. 2 It affects later life of (50-60 years old) males and females equally. 3 The clinical consequences of the disease implicate disturbed microcirculation and functional complaints such as headache, dizziness, paresthesias, visual problems, and arterial and venous thrombosis. 4 Hydroxyurea, interferon-α, anagrelides, and some agents such as clopidrogel that inhibits thromboc thrombocyte aggregation are used in the treatment. 5
In this report, a case of ET, diagnosed as a non-ST-segment elevation myocardial infarction (NSTEMI) and treated with tirofiban, a glycoprotein (GP) IIb/IIIa inhibitor, is presented.
Case Presentation
A 63-year-old man was admitted to the hospital with complaints of chest pain and dyspnea. He had been complaining of weakness and chest pain relieved with rest for 2 weeks, the intensity of chest pain increased in the day that he was sent to the emergency room. His past medical history was significant for high platelet counts with a nonrevealing workup for myeloproliferative disease. The patient's risk factors for coronary artery disease included history of heavy smoking (40 cigarettes/d) and hyperlipidemia. He had no history of spontaneous bleeding, prior myocardial infarction (MI), hypertension, diabetes mellitus, or a family history of coronary disease.
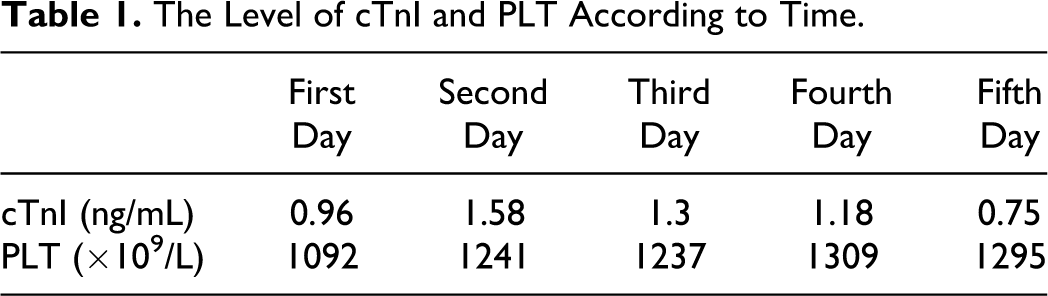
On physical examination, vital signs included blood pressure 130/80 mm Hg, pulse of 75/min, respirations 19/min, and temperature of 36.5°C. Cardiac examination was normal heart sounds with a regular rate and rhythm without murmurs, rubs, or gallops. Lung examination was clear to auscultation bilaterally, and the extremities had no clubbing or edema bilaterally. Laboratory work revealed a leukocyte count of 16.52 × 109/L with a normal differential cell count, hemoglobin of 161 g/L, hematocrit of 47.1%, and platelet (PLT) of 1092 × 109/L. Cardiac enzymes revealed a creatinine kinase (CK) of 79 u/L, The mass assay for CK-MB (MMB) of 1.8 ng/mL, and Cardiac Troponin I (cTnI) of 0.96 ng/mL (Table 1). The patient’s electrocardiogram (ECG) revealed normal sinus rhythm and a ventricular rate of 72 beats/min, with no acute ST-segment changes. Electrocardiogram showed QRS Qr in lead III and qr in lead aVF with no ST segment shift (Figure 1 ). The patient was diagnosed acute non-ST elevation MI according to Universal Definition of Myocardial Infarction. 6
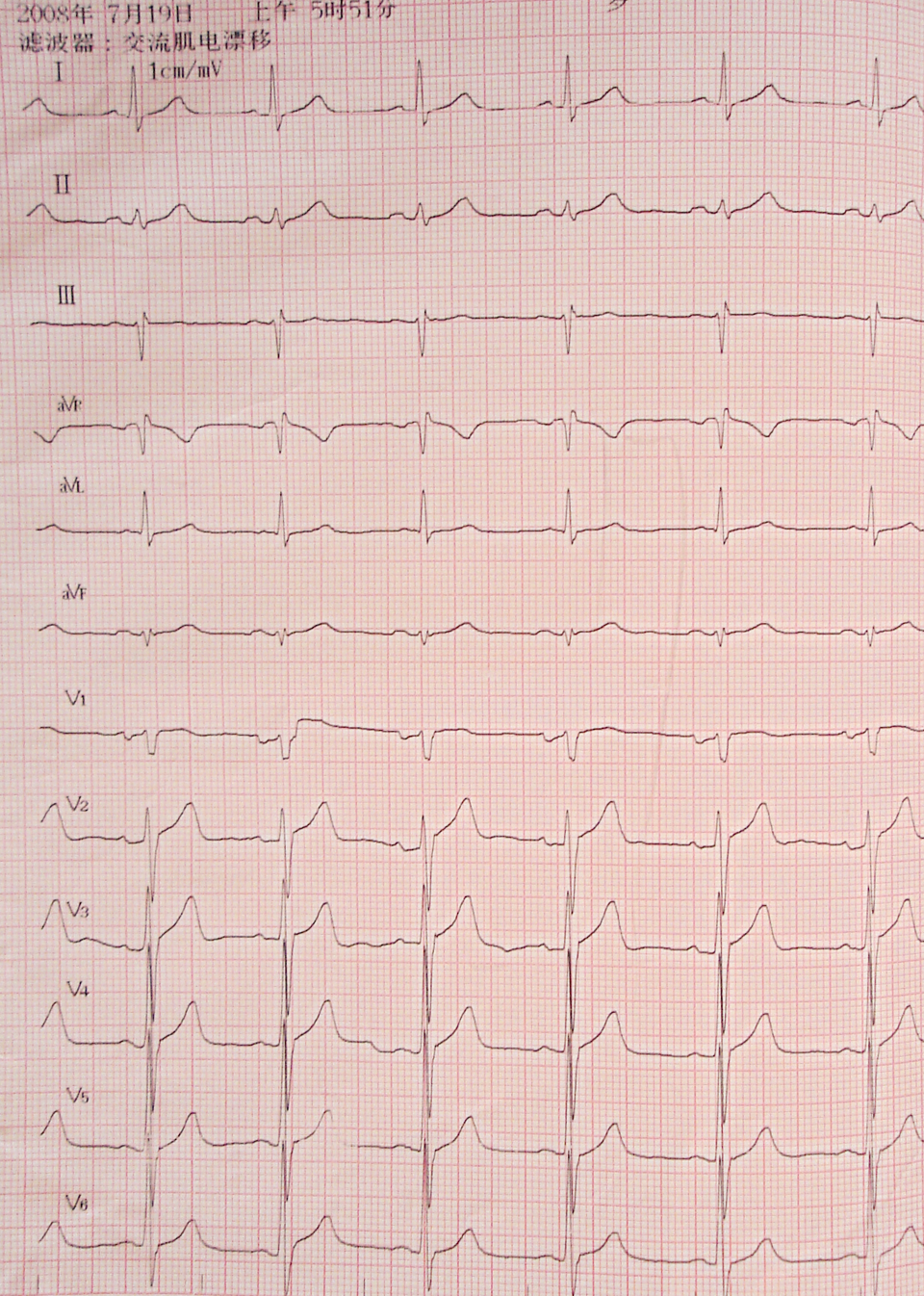
Electrocardiograms showed QRS Qr in lead III and qr in lead aVF with no ST segment shift.
The Level of cTnI and PLT According to Time.
The patient was transferred to the coronary care unit where continuous infusion of tirofiban (0.4 ug/kg permin bolus) followed by 0.1 ug/kg per min for 48 hours, heparin (1000 U/hours), and the oral combination of clopidogrel (75 mg/d before 300 mg bolus), plus aspirin (100 mg/d) was reinstituted. Bone marrow biopsy revealed megakaryocytic hyperplasia with mild degree fibrosis (Figure 2 ). Criteria for the diagnosis of ET were established by the World Health Organization Classification of Tumors Group and designed to exclude other potential causes of thrombocytosis such as underlying systemic illness, iron deficiency, and other myeloproliferative diseases. Hydroxyurea (at a dose of 1500 mg/d) treatment was added to the treatment. An ultrasonic cardiogram performed on the seventh day revealed no segmental wall motion abnormalities and the left ventricular ejection fraction was 71%. The patient refused to coronary angiography for his personal reason and was discharged.
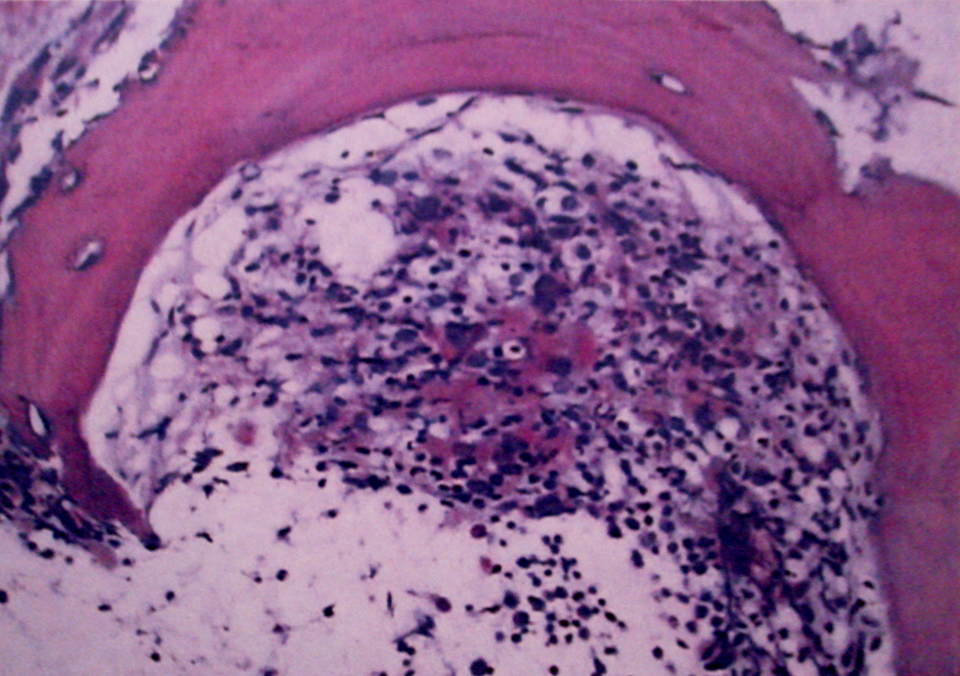
Bone marrow biopsy revealed megakaryocytic hyperplasia with mild degree fibrosis.
Discussion
Essential thrombocytopenia is a myeloproliferative disorder characterized by monoclonal proliferation of hematopoietic stem cells. It is manifested clinically by the overproduction of platelets in the absence of a definable cause. Patients who have ET have a tendency to experience thromboembolic events; the rate of cardiovascular complications varies between 4% and 21%. 7 However, in this hematologic disease where there is a significant increase in thrombocyte count, thrombosis or occlusion of coronary arteries leading to acute MI (AMI) develops rarely. 4,8
Criteria for the diagnosis of ET were established by the World Health Organization in 2007 and were designed to exclude other potential causes of thrombocytosis such as underlying systemic illness, iron deficiency, and other myeloproliferative diseases. 9 Although ET may cause systemic vascular thrombosis and subsequent tissue ischemia, involvement of the coronary arteries and consequent MI is exceedingly rare. Acute MI may be a cause of secondary thrombocytosis; but in secondary thrombocytosis, the platelet count is usually less than 1000 × 109/L. The platelet count in our case was higher than that reported in the literature for secondary thrombocytosis.
Douste-Blazy and associates 10 reported that in cases of ET, pathophysiologic mechanisms of thrombus formation in different coronary arteries were (1) activation of thrombocytes as a result of endothelial damage, (2) extended arterial spasms and as a result formation of thrombus, (3) increased procoagulant activity of thrombocytes, (4) changes in GPs on the surface of thrombocytes, and (5) possible deficiency of selective lipooxygenase. Acute MI, developing in cases of ET, was not a result of atherosclerotic plaque rupture and was characterized by the formation of primary thrombus due to increased numbers of platelets, frequently in intramural arteries and rarely in epicardial arteries. 11 In these patients, coronary angiograms are frequently found to be normal. 10 –12 No specific treatment of AMI, in patients with ET is reported.
In the literature, only rare cases of application of conventional treatment, thrombolytic treatment, or coronary angioplasty are found. 11,13 In this case, tirofiban, a GP IIb/IIIa receptor blocker was preferably used, taking into account the pathophysiology of the disease. There are no reports of the use of tirofiban in cases of ET with NSTEMI.
Essential thrombocythemia treatment is a difficult compromise between balancing the necessity of preventing thrombotic and/or hemorrhagic complications. Hydroxyurea is effective in preventing thrombosis in high-risk patients with ET by keeping the platelet count below 600 000/L. 14 Although hydroxyurea could reduce the platelet count, there is limited evidence that it can decrease thrombotic episodes in patients with ET. 14
Therefore, it may be thought that, in patients with ET, antithrombotic therapy could prevent acute coronary syndrome (ACS) generated by primary platelet rich thrombus, and blocking the GP IIb/IIIa receptors could break the continuing chain of aggregation and activation. 15 Clinical improvement following tirofiban treatment, noticed without any complication, was observed in this case.
Conclusion
Patients with high platelet counts should be evaluated carefully. It should be remembered that ET may result in catastrophic thrombotic complications like MI. Identification and successful treatment of similar cases with tirofiban will help in further understanding the pathophysiology of acute coronary syndromes in patients with ET.
Footnotes
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.